September 2008 [KT 1572] Sub
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Extracranial Course of Cranial Nerves
Extracranial course of cranial nerves Oculomotor, Trochlear, Abducent, Trigeminal, Facial and Accessory nerves Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Dr. Heba Kalbouneh Brainstem Mid brain Pons Medulla Pons Inferior view Facial nerve Anatomically, the course of the facial nerve can be divided into two parts: Motor: Innervates the muscles of facial Intracranial – the course of the nerve through expression, the posterior belly of the the cranial cavity, and the cranium itself. digastric, the stylohyoid and the stapedius Extracranial – the course of the nerve outside muscles. the cranium, through the face and neck. General Sensory: A small area around the concha of the auricle, EAM Special Sensory: Provides special taste sensation to the anterior 2/3 of the tongue. Parasympathetic: Supplies many of the glands of the head and neck, including: 1- Submandibular and sublingual salivary glands (via the submandibular ganglion/ chorda tympani) 2- Nasal, palatine and pharyngeal mucous glands (via the pterygopalatine ganglion/ greater petrosal) 3- Lacrimal glands (via the pterygopalatine ganglion/ greater petrosal) Dr. Heba Kalbouneh Intracranial course The nerve arises in the pons. It begins as two roots; a large motor root, and a small sensory root The two roots travel through the internal acoustic meatus. Pons Here, they are in very close proximity to the inner ear. 7th (motor) 8th Note: The part of the facial nerve that runs between the motor root of facial and vestibulocochlear nerve is sometimes Kalbouneh known as the nervus intermedius It contains the sensory and parasympathetic Heba fibers of the facial nerve Dr. Dr. Still within the temporal bone, the roots leave the internal acoustic meatus, and enter into the facial canal. -

Atlas of the Facial Nerve and Related Structures
Rhoton Yoshioka Atlas of the Facial Nerve Unique Atlas Opens Window and Related Structures Into Facial Nerve Anatomy… Atlas of the Facial Nerve and Related Structures and Related Nerve Facial of the Atlas “His meticulous methods of anatomical dissection and microsurgical techniques helped transform the primitive specialty of neurosurgery into the magnificent surgical discipline that it is today.”— Nobutaka Yoshioka American Association of Neurological Surgeons. Albert L. Rhoton, Jr. Nobutaka Yoshioka, MD, PhD and Albert L. Rhoton, Jr., MD have created an anatomical atlas of astounding precision. An unparalleled teaching tool, this atlas opens a unique window into the anatomical intricacies of complex facial nerves and related structures. An internationally renowned author, educator, brain anatomist, and neurosurgeon, Dr. Rhoton is regarded by colleagues as one of the fathers of modern microscopic neurosurgery. Dr. Yoshioka, an esteemed craniofacial reconstructive surgeon in Japan, mastered this precise dissection technique while undertaking a fellowship at Dr. Rhoton’s microanatomy lab, writing in the preface that within such precision images lies potential for surgical innovation. Special Features • Exquisite color photographs, prepared from carefully dissected latex injected cadavers, reveal anatomy layer by layer with remarkable detail and clarity • An added highlight, 3-D versions of these extraordinary images, are available online in the Thieme MediaCenter • Major sections include intracranial region and skull, upper facial and midfacial region, and lower facial and posterolateral neck region Organized by region, each layered dissection elucidates specific nerves and structures with pinpoint accuracy, providing the clinician with in-depth anatomical insights. Precise clinical explanations accompany each photograph. In tandem, the images and text provide an excellent foundation for understanding the nerves and structures impacted by neurosurgical-related pathologies as well as other conditions and injuries. -

Clinical Anatomy of Greater Petrosal Nerve and Its Surgical Importance
[Downloaded free from http://www.indianjotol.org on Monday, August 18, 2014, IP: 218.241.189.21] || Click here to download free Android application for this journal ORIGINAL ARTICLE Clinical anatomy of greater petrosal nerve and its surgical importance Prashant E Natekar, Fatima M De Souza Department of Anatomy, Goa Medical College, Bambolim, Goa, India Background: Surgical approach towards greater petrosal nerve has to be done with caution as many surgeons ABSTRACT are unfamiliar with the anatomy of the facial nerve. The anatomical landmarks selected must be reliable and above all easy to identify for identification of the greater petrosal nerve so as to avoid injury to the structures in the middle cranial fossa. Observation and Results: The present study is carried out on 100 temporal bones by examining the following measurements of the right and the left sides a) length of the hiatus for grater petrosal superficial nerve b) distance from superior petrosal sinus c) distance from lateral margin of middle cranial fossa d) arcuate eminence and e) distance from exit to the foramen ovale. Conclusion: The anatomical landmarks selected must be reliable and above all easy to identify. Bony structures are more suitable than soft tissue or cartilaginous landmarks because of their rigid and reliable location. These anatomical landmarks will definitely help the surgeon while performing vidian nerve neurectomy and also the anatomical relationship of the facial nerve in temporal bone. The middle fossa approach involves a temporal craniotomy in cases of perineural spread of adenoid cystic carcinomas hence these anatomical landmarks will serve as useful guide for the surgeons and radiologists. -

Parasympathetic Nucleus of Facial Nerve
Neurology of Lacrimation Michael Davidson Professor, Ophthalmology Diplomate, American College of Veterinary Ophthalmologists Department of Clinical Sciences College of Veterinary Medicine North Carolina State University Raleigh, North Carolina, USA Trigeminal Nerve and Lacrimation Sensory afferent from lacrimal gland, adnexa, eye – through ophthalmic division and first branch of maxillary division (zygomatic n.) maxillary branch To trigeminal ganglion ophthalmic branch – adjacent to petrous temporal bone lateral to mandibular branch cavernous sinus near middle ear trigeminal ganglion Terminal branches of trigeminal n. trigeminal nerve distributes sympathetic and parasympathetic efferent to lacrimal gland and face Trigeminal-Lacrimal Reflex Afferent arm = CN V, ophthalmic division ⇒trigeminal ganglion ⇒ principle CN V nuclei Efferent arm = parasympathetic efferent to lacrimal gland(s) Elicits reflex tearing Parasympathetic efferent also supplies basal stimuli for lacrimation www.slideplayer.com Parasympathetic Efferent to Lacrimal Gland CN VII parasympathetic nuclei ⇒ greater petrosal nerve (petrous temporal bone) ⇒ nerve of pterygoid canal (with post ganglionic sympathetics) ⇒ synapse in pterygopalatine ganglion (ventral periorbital region, near apex of orbit) ⇒ zygomatic nerve (CN V, maxillary division)* ⇒ zygomaticotemporal nerve ⇒ acinar cells of lacrimal gland** *some texts state postganglionic parasympathetic fibers also in lacrimal nerve (ophthalmic division CNV) **postganglionic parasympathetic innervation to nictitans -
Orbital Fractures
Vadim P. Nikolaenko Yury S. Astakhov Editors Orbital Fractures A Physician’s Manual 123 Orbital Fractures Vadim P. Nikolaenko • Yury S. Astakhov Editors Orbital Fractures A Physician's Manual Editors Vadim P. Nikolaenko, MD, PhD, DSc Yury S. Astakhov, MD, PhD, DSc Ophthalmology Ophthalmology Saint-Petersburg State Hospital No. 2 I.P. Pavlov First Saint Petersburg State Saint-Petersburg Medical University Russia Saint-Petersburg Russia Authorized translation of the 1st Russian language edition Orbital Fractures – A Physician’s Manual by Vadim P. Nikolaenko and Yury S. Astakhov © LLC Eco-Vektor, Saint-Petersburg, Russia, 2012, www.eco-vector.com All Rights Reserved ISBN 978-3-662-46207-2 ISBN 978-3-662-46208-9 (eBook) DOI 10.1007/978-3-662-46208-9 Library of Congress Control Number: 2015934822 Springer Heidelberg New York Dordrecht London © Springer-Verlag Berlin Heidelberg 2015 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifi cally the rights of translation, reprinting, reuse of illustrations, recita- tion, broadcasting, reproduction on microfi lms or in any other physical way, and transmission or infor- mation storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publica- tion does not imply, even in the absence of a specifi c statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. -

Facial Nerve
Facial nerve 7TH CARNIVAL NERVE Synopsis Introduction Nuclei Anatomical course Branches and it’s distribution FUNCTIONAL COMPONENTS 1. Motor function 2. Special sensory function 3. Parasympathetic functions Ganglia Clinical Relevance INTRODUCTION The facial nerve, CN VII, is the seventh paired cranial nerve. In this article, we shall look at the anatomical course of the nerve, and the motor, sensory and parasympathetic functions of its terminal branches. The facial nerve is associated with the derivatives of the second pharyngeal arch. NUCLEI The fibers of the nerve are connected to four nuclei situated in the lower pons 1. Motor nucleus or branchiomotor 2. Superior salivatory nucleus or parasympathetic 3. Lacrimatory nucleus is also parasympathetic 4. Nucleus to the tractus solitarius The motor nucleus lies deep in the reticular formation of lower pons. The part of nucleus that supplies muscles of upper part of face receives cortico nuclear fibers from motor cortex of both right and left side ANATOMICAL COURSE I Intacranial course: The facial nerve is attached to the brain stem by two roots ,motor and sensory.The sensory root is also called the nerves intermedius The two roots of facial nerve are attached to the later part of the lower border of the pons just medial to the eighth cranial nerve. The two roots run laterally and forwards , with the eighth nerve to reach the internal acoustic meatus In the meatus , the motor root lies in a groove on the eighth nerve, with the sensory root intervening.Here the seventh and eighth nerves are accompanied by labyrinthine vessels. Within the canal , the course of the nerve can be divided into three parts by two bends 1. -

Gross Anatomy; the Back September 10, 2015
Introduction to Gross Anatomy; the Back September 10, 2015 Dr. Pawel Kindler Department of Cellular and Physiological Sciences & MD Undergraduate Program LSC 1545 Following the lecture, you should be able to describe and/or define: Muscles - trapezius - latissimus dorsi intrinsic muscles extrinsic muscles - rhomboid major and minor - levator scapulae Bones deep superficial intermediate - scapula o spine o acromion o superior and inferior angles o superior, lateral and medial borders Nerves Accessory nerve (cranial nerve XI (CN XI)) Indicate the vertebral regions of the body Extrinsic muscles are involved with movements of the upper limbs and thoracic wall. This is in contrast to deep muscles which support and move the vertebral column and participate in moving the head. Extrinsic (superficial and intermediate) muscles acromion of scapula Trapezius serratus posterior superior spine of scapula serratus Latissimus dorsi posterior inferior SUPERFICIAL LAYER INTERMEDIATE LAYER Mainly for movement Mainly for breathing 1 very different innervation Superficial layer in more detail rhomboids are responsible for the movement of the scapula Levator scapulae rhomboid minor Trapezius the point that differentiates between minor and major rhomboid major Latissimus dorsi acromion (articulates with Scapula the clavicle) superior superior angle border Spine of the scapula Deep back muscles responsible for movement of the head medial border lateral border Suboccipital Splenius inferior angle Erector spinae 2 Vertebral regions Example lab exam questions: -Where did this scapule come from? which side? -What part of the spine did this vertebra come from? Cervical (7) CERVICAL -Bifid spinous process -Until C6? Thoracic -Body = heart shaped -Long spinous process -Rib facets exist Thoracic (12) Lumbar -Body = kidney shaped and huge -Short thick spinous process Lumbar (5) Sacral (5 fused) Coccyx (3~4 fused) 3 Introduction to the Nervous System and Spinal Nerves September 17, 2015 STRUCTURALLY, the nervous system is organized into CNS and PNS Dr. -

The Pterygopalatine Fossa
2 Omran Saeed Luma Taweel Mohammad Almohtaseb 1 | P a g e I didn’t include all the photos in this sheet in order to keep it as small as possible so if you need more clarification please refer to slides In this lecture we’re gonna discuss paranasal sinuses and pterygopalatine fossa. The paranasal sinuses are spaces inside skull bones. They’re all lined with respiratory mucosa which is pseudostratified ciliated columnar epithelium but the mucosa here is thin. - All sinuses open by ducts into lateral wall of the nose. - The innervation is branches from “CN V” Trigeminal nerve (the Trigeminal gives rise to three branches: ophthalmic, maxillary and mandibular). Here in paranasal sinuses we’re interested in the first two branches, mandibular nerve don’t innervate these sinuses. - There are 6 ethmoidal sinuses, 2 sphenoid, 2 maxillary, and 2 frontal air sinuses. Functions: 2 | P a g e 1- resonance of the voice. 2- decreased weight of the skull. 3- Protection (by moisturizing and modifying of the temperature and reduce intracranial pressure) Paranasal sinuses: 1- The Frontal air sinus is present in frontal bone and it is triangular in shape. At birth it is small and called rudimental while in adults it becomes bigger. Drainage: frontonasal duct into infundibulum (a space in front of the middle meatus especially hiatus semilunaris) Innervation: it is innervated by the supraorbital nerve, a branch of the ophthalmic nerve that passes through supraorbital foramen. 2- The Ethmoidal air sinuses/ cells three pairs of sinuses; anterior, middle and posterior air sinuses (3 on the right and 3 on the left). -

The Nose Embryology the Nose Developed from the Frontonasal Process
The Nose Embryology The nose developed from the frontonasal process. Anatomy The nose is formed of external nose and nasal cavity (A) The external nose Pyramidal in shape shows: The skeleton is formed of: 1- Bony upper 1/3: - Two nasal bones. - Nasal (frontal) process of maxilla. - Nasal process of frontal bone. 2- Cartilaginous lower 2/3: - Upper lateral cartilage. - Lower lateral cartilage. - Septal cartilage. (B) Nasal cavity Each nasal cavity has 2 openings and 4 walls. 1- Anterior nares or nostrils: separated by the columella. 2- Posterior nares or choanae: open into nasopharynx. 3- Roof: cribriform plate of ethmoid bone, frontal bone ant. 4- Floor: hard palate 5- Medial wall: Septum - Vertical plate of ethmoid: postero superior. - Vomer bone postero inferior. - Quadrangular Septal cartilage - Maxillary crest inferiorly. 6- Lateral wall: formed by medical wall of maxilla(ethmoidal labrynth) , vertical plate of palatine bone, and (inner aspect of nasal bone, frontal process of maxilla, lacrimal bone) it shows: A- 3 bony projections: superior, middle, and inferior conchae or turbinates. B- Each turbinate covers a recess called meatus, there are superior, middle, and inferior meati, in addition to spheno-ethmoidal recess above the superior turbinate. - Inferior meatus drains nasolacrimal duct(site of I.N.A) - Middle meatus drains. 1 Anterior ethmoids via bulla ethmoidalis. Frontal sinus via ant. part of hiatus semilunaris. Maxillary sinus via postero inf. Part or hiatus semi lunaris. - Superior meatus drains: posterior ethmoids. - Spheno- ethmoidal recess drains sphenoid sinus. Blood supply (A) Arterial External nose Nasal cavity - Facial → ECA - Ant and post ethmoidal → ophthalmic. - Ophthalmic → ICA - Spheno palatine → maxillary. -
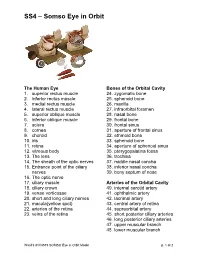
SS4 – Somso Eye in Orbit
SS4 – Somso Eye in Orbit The Human Eye Bones of the Orbital Cavity 1. superior rectus muscle 24. zygomatic bone 2. inferior rectus muscle 25. sphenoid bone 3. medial rectus muscle 26. maxilla 4. lateral rectus muscle 27. infraorbital foramen 5. superior oblique muscle 28. nasal bone 6. inferior oblique muscle 29. frontal bone 7. sclera 30. frontal sinus 8. cornea 31. aperture of frontal sinus 9. choroid 32. ethmoid bone 10. iris 33. sphenoid bone 11. retina 34. aperture of sphenoid sinus 12. vitreous body 35. pterygopalatina fossa 13. The lens 36. trochlea 14. The sheath of the optic nerves 37. middle nasal concha 15. Entrance point of the ciliary 38. inferior nasal concha nerves 39. bony septum of nose 16. The optic nerve 17. ciliary muscle Arteries of the Orbital Cavity 18. ciliary crown 40. internal carotid artery 19. venae vorticosae 41. ophthalmic artery 20. short and long ciliary nerves 42. lacrimal artery 21. macula(yellow spot) 43. central artery of retina 22. arteries of the retina 44. supraorbital artery 23. veins of the retina 45. short posterior ciliary arteries 46. long posterior ciliary arteries 47. upper muscular branch 48. lower muscular branch Ward’s 81V3519 SOMSO Eye in Orbit Model p. 1 of 2 SS4 – Somso Eye in Orbit 49. posterior ethmoid artery 83. branch communication with 50. anterior ethmoid artery nasociliary nerve 51. upper palpebral artery 52. supratrochlear artery The Lacrimal Organs with 53. posterior communicating Eyelid Supports artery 1. lacrimal gland 54. anterior cerebral artery 2. upper part 55. cavernous sinus and internal 3. lower part carotid artery 4. -
Peripheral Nervous System Peripheral Nervous System Comprises: A) Cranial Nerves: 12 in Number, Arise Mainly from Brain Stem
Peripheral nervous system Peripheral nervous system comprises: A) Cranial nerves: 12 in number, arise mainly from brain stem. B) Spinal nerves: arise from spinal cord, varies in number according to species. C) Autonomic nervous system : 1-Sympathetic (thoracolumbar) division. 2-Parasympathetic (craniosacral) division. Cranial nerves They are 12 pairs General features: – They are known by roman numbers from (rostral to caudal) . – Some nerves take their names according to: * Function as olfactory and abducent * Distribution as facial and hypoglossal * Shape as trigeminal. - All cranial nerves have superficial origins on ventral aspect of brain except trochlear nerve originates from dorsal aspect of brain. -All cranial nerves except first one originate from brain stem. - Each nerve emerges from cranial cavity through a foramen. - All cranial nerves except vagus distributed generally in head region. - 3,7,9,10 cranial nerves carry parasympathetic fibers. - Classification of cranial nerves: - They are classified according to the function into: 1-Sensory nerves: 1,2,8. 2-Motor nerves: 3,4,6,11,12. 3-Mixed nerves: 5,7,9,10. I- Olfactory nerves Type: • Sensory for smell. • Represented by bundles of nerve fibers, not form trunk. Origin: • Central processes of olfactory cells of olfactory region of nasal cavity. Course: • They pass though cribriform plate to join olfactory bulb. Vomeronasal nerve: • It arises from vomeronasal organ ,passes through medial border of cribriform plate to terminate in olfactory bulb. II- Optic nerve Type: • Sensory for vision. Origin: • Central processes of ganglion cells of retina. Course: • Fibers converge toward optic papilla forming optic nerve, emerges from eyeball. • Then passes through optic foramen and decussates with its fellow to form optic chiasma. -

Pharynx, Larynx, Nasal Cavity and Pterygopalatine Fossa
Pharynx, Larynx, Nasal cavity And Pterygopalatine Fossa Mikel H. Snow, Ph.D. Dental Anatomy [email protected] July 29, 2018 Pharynx Food & Air Passage Pharynx The pharynx is a skeletal muscle tube that opens anteriorly with 3 regions. The upper part communicates with nasal cavity, the middle communicates with oral cavity, and the lower communicates with the larynx. Nasal cavity Nasal Oral cavity cavity Larynx Air Nasopharynx: between Oral sphenoid sinus & uvula Food/ cavity Oropharynx: between uvula & epiglottis drink Laryngopharynx: between epiglottis & esophagus Esophagus Trachea The posterior and lateral walls are 3 skeletal muscles (constrictors) that propel food/liquid inferiorly to the esophagus. Constrictors innervated by CNX. Additional muscles elevate the pharynx (stylopharyngeus is external). Stylopharyngeus innervated by CNIX. Stylopharyngeus Superior constrictor Middle constrictor Inferior constrictor Two additional internal muscles we’ll get to later… Key relationship: Glossopharyngeal nerve wraps around stylopharyngeus muscle. CN IX wraps around stylopharyngeus muscle and Stylopharyngeus innervates it. Pharyngeal constrictors Pharynx Interior 1 Nasopharynx: 1. Pharyngeal tonsils 2. Auditory tube ostia 2 3 3. Salpingopharyngeal fold 4 4 Oropharynx: 4. Palatine tonsils 5 5 Laryngopharynx: Slit open 5. Piriform recess constrictors to examine interior Lateral Wall of Pharynx 5. Salpingopharyngeus muscle 6. Levator veli palatini muscle 1. Pharyngeal tonsils 7. Tensor veli palatini muscle 2. Torus tubarius 8. Palatine tonsil 3.