Greater Superficial Petrosal Nerve and Its Surgical Importance: a Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
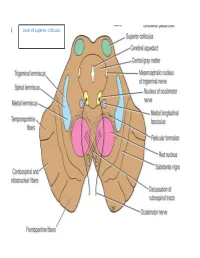
Level of Superior Colliculus ° Edinger- Westphal Nucleus ° Pretectal Nucleus: Close to the Lateral Part of the Superior Colliculus
Level of superior colliculus ° Edinger- Westphal nucleus ° pretectal nucleus: close to the lateral part of the superior colliculus. Red nucleus • Rounded mass of gray matter • Situated bt cerebral aqueduct and substantia nigra • Reddish blue(vascularity & iron containing pigment) • Afferents from: cerebral cortex,cerebellum,substa ntia nigra, thalamic nuclei, spinal cord • Efferent to: spinal cord, reticular formation. thalamus and substantia nigra • involved in motor coordination. Crus cerebri • Corticospinal & corticonuclear fibers (middle) • Frontopontine fibers (medial) • Temporopontine fibers (lateral) these descending tracts connect the cerebral cortex with spinal cord, cranial nerves nuclei, pons & cerebellum Level at superior colliculus ° Superior colliculus ° Occulomotor nucleus (posterior to MLF) ° Occulomotor n emerges through red nucleus ° Edinger-Westphal nucleus ° pretectal nucleus: close to the lateral part of the superior colliculus. ° MLF ° Medial , trigeminal, spinal leminiscus ( no lateral leminiscus) ° Red nucleus ° Substantia nigra ° Crus cerebri ° RF Substantia nigra ° Large motor nucleus ° is a brain structure located in the midbrain ° plays an important role in reward, addiction, and movement. ° Substantia nigra is Latin for "black substance" due to high levels of melanin ° has connections with basal ganglia ,cerebral cortex ° Concerned with muscle tone ° Parkinson's disease is caused by the death of neurons in the substantia nigra Oculomotor Nerve (III) • Main oculomotor nucleus • Accessory parasympathetic nucleus -

The Anatomic Analysis of the Vidian Canal and the Surrounding
Braz J Otorhinolaryngol. 2019;85(2):136---143 Brazilian Journal of OTORHINOLARYNGOLOGY www.bjorl.org ORIGINAL ARTICLE The anatomic analysis of the vidian canal and the surrounding structures concerning vidian neurectomy ଝ using computed tomography scans a,∗ a b Gülay Ac¸ar , Aynur Emine C¸ic¸ekcibas¸ı , ˙Ibrahim C¸ukurova , c a d Kemal Emre Özen , Muzaffer ¸ekerS , ˙Ibrahim Güler a Necmettin Erbakan University, Meram Faculty of Medicine, Department of Anatomy, Konya, Turkey b Health Sciences University, Izmir Tepecik Trainig and Research Hospital, Department of Otolaryngology-Head and Neck Surgery, Izmir, Turkey c Katip C¸elebi University, Faculty of Medicine, Department of Anatomy, Izmir, Turkey d Selcuk University, Faculty of Medicine, Department of Radiology, Konya, Turkey Received 15 September 2017; accepted 8 November 2017 Available online 26 December 2017 KEYWORDS Abstract Intrasphenoid Introduction: The type of endoscopic approach chosen for vidian neurectomy can be specified septum; by evaluating the vidian canal and the surrounding sphenoid sinus structures. Morphometric Objective: The variations and morphometry of the vidian canal were investigated, focusing on analysis; the functional correlations between them which are crucial anatomical landmarks for preoper- Pterygoid process ative planning. pneumatization; Methods: This study was performed using paranasal multidetector computed tomography Vidian canal; images that were obtained with a section thickening of 0.625 mm of 250 adults. Vidian neurectomy Results: The distributions of 500 vidian canal variants were categorized as follows; Type 1, within the sphenoid corpus (55.6%); Type 2, partially protruding into the sphenoid sinus (34.8%); Type 3, within the sphenoid sinus (9.6%). The pneumatization of the pterygoid process is mostly seen in vidian canal Type 2 (72.4%) and Type 3 (95.8%) (p < 0.001). -

Extracranial Course of Cranial Nerves
Extracranial course of cranial nerves Oculomotor, Trochlear, Abducent, Trigeminal, Facial and Accessory nerves Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Dr. Heba Kalbouneh Brainstem Mid brain Pons Medulla Pons Inferior view Facial nerve Anatomically, the course of the facial nerve can be divided into two parts: Motor: Innervates the muscles of facial Intracranial – the course of the nerve through expression, the posterior belly of the the cranial cavity, and the cranium itself. digastric, the stylohyoid and the stapedius Extracranial – the course of the nerve outside muscles. the cranium, through the face and neck. General Sensory: A small area around the concha of the auricle, EAM Special Sensory: Provides special taste sensation to the anterior 2/3 of the tongue. Parasympathetic: Supplies many of the glands of the head and neck, including: 1- Submandibular and sublingual salivary glands (via the submandibular ganglion/ chorda tympani) 2- Nasal, palatine and pharyngeal mucous glands (via the pterygopalatine ganglion/ greater petrosal) 3- Lacrimal glands (via the pterygopalatine ganglion/ greater petrosal) Dr. Heba Kalbouneh Intracranial course The nerve arises in the pons. It begins as two roots; a large motor root, and a small sensory root The two roots travel through the internal acoustic meatus. Pons Here, they are in very close proximity to the inner ear. 7th (motor) 8th Note: The part of the facial nerve that runs between the motor root of facial and vestibulocochlear nerve is sometimes Kalbouneh known as the nervus intermedius It contains the sensory and parasympathetic Heba fibers of the facial nerve Dr. Dr. Still within the temporal bone, the roots leave the internal acoustic meatus, and enter into the facial canal. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

Morphometry and Morphology of Foramen Petrosum in Indian Population
Basic Sciences of Medicine 2020, 9(1): 8-9 DOI: 10.5923/j.medicine.20200901.02 Morphometry and Morphology of Foramen Petrosum in Indian Population Rajani Singh1,*, Nand Kishore Gupta1, Raj Kumar2 1Department of Anatomy, Uttar Pradesh University of Medical Sciences Saifai 206130 Etawah UP India 2Department of Neurosugery Uttar Pradesh University of Medical Sciences Saifai 206130 Etawah UP India Abstract Greater wing of sphenoid contains three constant foramina, Foramen ovale, foramen rotundum and foramen spinosum. The presence of foramen Vesalius and foramen petrosum are inconsistent. Normally foramen ovale transmits mandibular nerve, accessory meningeal artery, lesser petrosal nerve and emissary vein. When foramen petrosum is present, lesser petrosal nerve passes through petrosal foramen instead of foramen ovale. Lesser petrosal nerve distribute postganglionic fibers from otic ganglion to parotid gland. In absence of knowledge of petrosal foramen transmitting lesser petrosal nerve, the clinician may damage the nerve during skull base surgery creating complications like hyperemia of face and profuse salivation from the parotid gland (following atropine administration), lacrimation (crocodile tears syndrome) and mucus nasal secretion. Considering clinical implications associated with petrosal foramen, the study was carried out. The aim of the study is to determine the prevalence of petrosal foramen in Indian Population and to bring out associated clinical significance. The study was conducted in the department of Anatomy UPUMS Saifai Etawah Indian. 30 half skulls were observed for the presence of petrosal foramina and morphometry was also done. Literature search was carried out, our findings were compared with previous work and associated clinical implications were bought out. Keywords Petrosal foramen, Lesser petrosal nerve, Foramen ovale patients. -
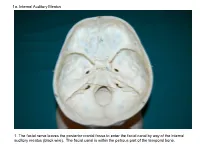
1A. Internal Auditory Meatus
1a. Internal Auditory Meatus 1. The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). The facial canal is within the petrous part of the temporal bone. 1b. Internal Auditory Meatus The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). 2. Hiatus of the Canal and Groove for the Greater Superficial Petrosal Nerve The greater superficial petrosal nerve leaves the facial canal to enter the middle cranial fossa by way of the hiatus of the canal for the greater superficial petrosal nerve (black wire). 3. Pterygoid Canal at Anterior Lip of the Lacerate Foramen The greater superficial petrosal nerve is joined by the deep petrosal nerve to form the nerve of the pterygoid canal (black and red wire). This nerve leaves the middle cranial fossa to enter the pterygopalatine fossa by way of the pterygoid canal. The posterior opening of the pterygoid canal is at the anterior lip of the lacerate foramen. The greater superficial nerve and the deep petrosal nerve travel within the cavernous sinus. 4. Pterygopalatine Fossa Seen Through the Pterygomaxillary Fissure The anterior opening of the pterygoid canal is into the pterygopalatine fossa (black wire). The pterygopalatine fossa is located medial to the pterygomaxillary fissure and contains the pterygopalatine ganglion. 5. External Auditory Meatus The chorda tympani nerve leaves the facial canal and crosses the middle ear (black wire). It then leaves the middle ear to arrive in the infratemporal fossa by way of the petrotympanic fissure. -

Trigeminal Cave and Ganglion: an Anatomical Review
Int. J. Morphol., 31(4):1444-1448, 2013. Trigeminal Cave and Ganglion: An Anatomical Review Cavo y Ganglio Trigeminal: Una Revisión Anatómica N. O. Ajayi*; L. Lazarus* & K. S. Satyapal* AJAYI, N. O.; LAZARUS, L. & SATYAPAL, K. S. Trigeminal cave and ganglion: an anatomical review. Int. J. Morphol., 31(4):1444- 1448, 2013. SUMMARY: The trigeminal cave (TC) is a special channel of dura mater, which extends from the posterior cranial fossa into the posteromedial portion of the middle cranial fossa at the skull base. The TC contains the motor and sensory roots of the trigeminal nerve, the trigeminal ganglion (TG) as well as the trigeminal cistern. This study aimed to review the anatomy of the TC and TG and determine some parameters of the TC. The study comprised two subsets: A) Cadaveric dissection on 30 sagitally sectioned formalin fixed heads and B) Volume injection. We found the dura associated with TC arranged in three distinct layers. TC had relations with internal carotid artery, the cavernous sinus, the superior petrosal sinus, the apex of petrous temporal bone and the endosteal dura of middle cranial fossa. The mean volume of TC was 0.14 ml. The mean length and breadth of TG were 18.3 mm and 7.9 mm, respectively, mean width and height of trigeminal porus were 7.9 mm and 4.1 mm, respectively, and mean length of terminal branches from TG to point of exit within skull was variable. An understanding of the precise formation of the TC, TG, TN and their relations is important in order to perform successful surgical procedures and localized neural block in the region of the TC. -

Brain Structure and Function Related to Headache
Review Cephalalgia 0(0) 1–26 ! International Headache Society 2018 Brain structure and function related Reprints and permissions: sagepub.co.uk/journalsPermissions.nav to headache: Brainstem structure and DOI: 10.1177/0333102418784698 function in headache journals.sagepub.com/home/cep Marta Vila-Pueyo1 , Jan Hoffmann2 , Marcela Romero-Reyes3 and Simon Akerman3 Abstract Objective: To review and discuss the literature relevant to the role of brainstem structure and function in headache. Background: Primary headache disorders, such as migraine and cluster headache, are considered disorders of the brain. As well as head-related pain, these headache disorders are also associated with other neurological symptoms, such as those related to sensory, homeostatic, autonomic, cognitive and affective processing that can all occur before, during or even after headache has ceased. Many imaging studies demonstrate activation in brainstem areas that appear specifically associated with headache disorders, especially migraine, which may be related to the mechanisms of many of these symptoms. This is further supported by preclinical studies, which demonstrate that modulation of specific brainstem nuclei alters sensory processing relevant to these symptoms, including headache, cranial autonomic responses and homeostatic mechanisms. Review focus: This review will specifically focus on the role of brainstem structures relevant to primary headaches, including medullary, pontine, and midbrain, and describe their functional role and how they relate to mechanisms -

Clinical Anatomy of the Trigeminal Nerve
Clinical Anatomy of Trigeminal through the superior orbital fissure Nerve and courses within the lateral wall of the cavernous sinus on its way The trigeminal nerve is the fifth of to the trigeminal ganglion. the twelve cranial nerves. Often Ophthalmic Nerve is formed by the referred to as "the great sensory union of the frontal nerve, nerve of the head and neck", it is nasociliary nerve, and lacrimal named for its three major sensory nerve. Branches of the ophthalmic branches. The ophthalmic nerve nerve convey sensory information (V1), maxillary nerve (V2), and from the skin of the forehead, mandibular nerve (V3) are literally upper eyelids, and lateral aspects "three twins" carrying information of the nose. about light touch, temperature, • The maxillary nerve (V2) pain, and proprioception from the enters the middle cranial fossa face and scalp to the brainstem. through foramen rotundum and may or may not pass through the • The three branches converge on cavernous sinus en route to the the trigeminal ganglion (also called trigeminal ganglion. Branches of the semilunar ganglion or the maxillary nerve convey sensory gasserian ganglion), which contains information from the lower eyelids, the cell bodies of incoming sensory zygomae, and upper lip. It is nerve fibers. The trigeminal formed by the union of the ganglion is analogous to the dorsal zygomatic nerve and infraorbital root ganglia of the spinal cord, nerve. which contain the cell bodies of • The mandibular nerve (V3) incoming sensory fibers from the enters the middle cranial fossa rest of the body. through foramen ovale, coursing • From the trigeminal ganglion, a directly into the trigeminal single large sensory root enters the ganglion. -

Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens After Decalcification
Hindawi Publishing Corporation International Journal of Otolaryngology Volume 2012, Article ID 418650, 7 pages doi:10.1155/2012/418650 Research Article Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens after Decalcification Longping Liu, Robin Arnold, and Marcus Robinson Discipline of Anatomy and Histology, University of Sydney, Anderson Stuart Building F13, Sydney, NSW 2006, Australia Correspondence should be addressed to Marcus Robinson, [email protected] Received 29 July 2011; Revised 10 November 2011; Accepted 12 December 2011 AcademicEditor:R.L.Doty Copyright © 2012 Longping Liu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The whole course of the chorda tympani nerve, nerve of pterygoid canal, and facial nerves and their relationships with surrounding structures are complex. After reviewing the literature, it was found that details of the whole course of these deep nerves are rarely reported and specimens displaying these nerves are rarely seen in the dissecting room, anatomical museum, or atlases. Dissections were performed on 16 decalcified human head specimens, exposing the chorda tympani and the nerve connection between the geniculate and pterygopalatine ganglia. Measurements of nerve lengths, branching distances, and ganglia size were taken. The chorda tympani is a very fine nerve (0.44 mm in diameter within the tympanic cavity) and approximately 54 mm in length. The mean length of the facial nerve from opening of internal acoustic meatus to stylomastoid foramen was 52.5 mm. -

Facial Nerves Was Found in This Patient with a Unilateral Pure Motor Stroke Due to Ischaemia in the Pons
73272ournal ofNeurology, Neurosurgery, and Psychiatry 1995;58:732-734 SHORT REPORT J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.58.6.732 on 1 June 1995. Downloaded from Volitional type of facial palsy associated with pontine ischaemia Rudolf T6pper, Christoph Kosinski, Michael Mull Abstract nounced during voluntary contraction A dissociation between voluntary and whereas emotionally triggered contractions emotional facial innervation is described are preserved or at times even exaggerated on in a patient with a pure motor stroke due the paretic side.' In the emotional type of to a unilateral ischaemic pontine infarc- facial palsy the opposite phenomenon can be tion. Voluntary facial innervation of the seen: whereas voluntary triggered contrac- contralateral orbicularis oris muscle was tions are normal, there is facial impairment affected whereas emotionally induced during emotionally triggered movements. innervation of the same muscle was Automatic voluntary dissociation is not spared. This report provides evidence restricted to muscles supplied by the facial that fibres conveying voluntary and emo- nerve: in the bilateral anterior opercular syn- tional commands are still separated in drome automatic voluntary dissociation is Department of the pons. Whereas corticobulbar tracts also seen in masticatory muscles supplied by Neurology carry the information for voluntary facial the trigeminal nerve, in the tongue, and in R Topper innervation, efferents from the amygdala muscles involved in swallowing.2 Whereas the C Kosinski and the lateral hypothalamus are candi- volitional type of facial palsy is thought to be Department of Neuroradiology, dates for the somatomotor aspects of caused by a lesion in the motor cortex or in Technical University emotions. -

CT of Perineural Tumor Extension: Pterygopalatine Fossa
731 CT of Perineural Tumor Extension: Pterygopalatine Fossa Hugh D. Curtin1.2 Tumors of the oral cavity and paranasal sinuses can spread along nerves to areas Richard Williams 1 apparently removed from the primary tumor. In tumors of the palate, sinuses, and face, Jonas Johnson3 this "perineural" spread usually involves the maxillary division of the trigeminal nerve. The pterygopalatine fossa is a pathway of the maxillary nerve and becomes a key landmark in the detection of neural metastasis by computed tomogaphy (CT). Oblitera tion of the fat in the fossa suggests pathology. Case material illustrating neural extension is presented and the CT findings are described. Perineural extension is possibly the most insidious form of tumor spread of head and neck malignancy. After invading a nerve, tumor follows the sheath to reach the deeper connections of the nerve, escaping the area of a planned resection. Thus, detection of this form of extension is important in treatment planning and estimation of prognosis. The pterygopalatine fossa (PPF) is a key crossroad in extension along cranial nerve V. The second branch of the trigeminal nerve passes from the gasserian ganglion through the foramen rotundum into the PPF. Here the nerve branches send communications to the palate, sinus, nasal cavity, and face. Tumor can follow any of these routes proximally into the PPF and eventually to the gasserian ganglion in the middle cranial fossa. The PPF contains enough fat to be an ideal subject for computed tomographic (CT) evaluation. Obliteration of this fat is an important indicator of pathology, including perineural tumor spread. Other signs of perineural extension include enlargement of foramina, increased enhancement in the region of Meckel cave (gasserian ganglion), and atrophy of the muscles innervated by the trigeminal nerve.