The San Marino
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Repubblica Di San Marino
http://www.consigliograndeegenerale.sm/new/proposte_di_legge/vis_lavo...posta=6870&colonnakey=idlegge&tabella=leggi&colonna=testDISCLAIMER: As Member States provide national legislations, hyperlinks and explanatory notes (if any), UNESCO does not guarantee their accuracy, nor their up-datingolegge&testo= on this web site, and is not liable for any incorrect information. COPYRIGHT: All rights reserved.This information may be used only for research, educational, legal and non- commercial purposes, with acknowledgement of UNESCO Cultural Heritage Laws Database as the source (© UNESCO). LEGGE 28 ottobre 2005 n.147 REPUBBLICA DI SAN MARINO Elenco dei manufatti o immobili con valore di monumento di cui al Capo VII, Sezione I della Legge 19 luglio 1995 n.87 (Testo Unico delle Leggi Urbanistiche ed Edilizie) Noi Capitani Reggenti la Serenissima Repubblica di San Marino Promulghiamo e mandiamo a pubblicare la seguente legge approvata dal Consiglio Grande e Generale nella seduta del 28 ottobre 2005. Art.1 (Valore di monumento) Il valore di monumento è attribuito ad un manufatto o immobile in base a quanto disposto dall'articolo 1 della Legge 10 giugno 1919 n.17 e dall'articolo 197 capo VII sezione I della Legge 19 luglio 1995 n. 87. Fanno parte dell'elenco dei manufatti o immobili con valore di monumento i manufatti o immobili di interesse archeologico e paletnologico ed i manufatti o immobili di interesse storico ed artistico nonchè culturale ed ambientale la cui costruzione risalga ad almeno cinquant'anni o che comunque siano attribuiti ad autore non vivente. Art.2 (Dell’elenco) L'elenco, redatto sulla base delle indicazioni e delle valutazioni fornite dalla Commissione per la Conservazione dei Monumenti e degli Oggetti d'Antichità ed Arte (CCM), contiene manufatti o immobili con valore di monumento individuati mediante documentata catalogazione di cui all'allegato A della presente legge. -

Iv-Agosto-2007.Pdf 365KB
IV Settembre 2007 - Anno I CF e Periodico a cura dell’Ente Cassa di Faetano zi ti numerose iniziative, alcune delle quali sono settori ed interessi molto diversi, tuttavia una o illustrate anche su queste pagine, mentre presenza significativa dei Soci alle iniziative n altri importanti progetti prenderanno avvio. dell’Ente rappresenta per noi un obiettivo Probabilmente ve ne state accorgendo an- desiderato e perseguito, oltre che un inco- La parola al Presidente che dagli inviti che vi giungono con frequen- raggiamento a proseguire in un’attività che si UN AUTUNNO RICCO za sempre maggiore. Non si tratta di inviti di fa sempre più intensa e complessa. DI GRANDI circostanza, spediti per pura formalità; al Il nostro Ente sta crescendo nel numero APPUNTAMENTI contrario vogliono essere delle opportunità e nella qualità delle iniziative proposte e si concrete offerte a tutti noi, non solo per so- sta rivelando sempre più una risorsa per la L’Ente Cassa di Faetano si cializzare ma anche per conoscere, per nostra Repubblica. Di questo crediamo sia appresta a vivere un autunno gustare, per crescere. E’ evidente che non lecito andare giustamente fieri. veramente “caldo” nel corso del tutti i Soci potranno partecipare a tutte le quale giungeranno a realizzazione iniziative proposte che peraltro spaziano in ARTE PER MARE: SULLE ORME DEI SANTI MARINO E LEONE Tra gli eventi destinati a lasciare un segno natale sono fino ad oggi scarse, la città di Salona profondo nella Repubblica si colloca in un posto al di là dal mare e Rimini, sulla costa opposta, di rilievo la mostra dedicata ai Santi Marino e offrono una sicura base di partenza per l’avvio del Leone.“Arte per mare - Dalmazia, Titano e Mon- percorso espositivo. -

Match Press Kits
EUROPEAN QUALIFIERS - 2021/22 SEASON MATCH PRESS KITS San Marino Stadium - Serravalle Sunday 5 September 2021 20.45CET (20.45 local time) San Marino Group I - Matchday 5 Poland Last updated 05/09/2021 10:58CET EUROPEAN QUALIFIERS OFFICIAL SPONSORS Previous meetings 2 Squad list 3 Match officials 5 Match-by-match lineups 6 Legend 8 1 San Marino - Poland Sunday 5 September 2021 - 20.45CET (20.45 local time) Match press kit San Marino Stadium, Serravalle Previous meetings Head to Head FIFA World Cup Stage Date Match Result Venue Goalscorers reached Ales. Della Valle 22; Zieliński 10, 66, 10/09/2013 QR (GS) San Marino - Poland 1-5 Serravalle Błaszczykowski 23, Sobota 34, Mierzejewski 75 Lewandowski 21 (P), 50 (P), Piszczek 28, 26/03/2013 QR (GS) Poland - San Marino 5-0 Warsaw Teodorczyk 61, Kosecki 90+2 FIFA World Cup Stage Date Match Result Venue Goalscorers reached Boguski 1, 27, Smolarek 18, 60, 72, 81, Lewandowski 43, 01/04/2009 QR (GS) Poland - San Marino 10-0 Kielce Jeleń 51, M. Lewandowski 63, Saganowski 88 Smolarek 36, 10/09/2008 QR (GS) San Marino - Poland 0-2 Serravalle Lewandowski 68 UEFA EURO 2004 Stage Date Match Result Venue Goalscorers reached Szymkowiak 3, Ostrowiec 02/04/2003 PR (GS) Poland - San Marino 5-0 Kosowski 26, Kuźba Swietokrzyski 54, 90+3, Karwan 81 Kaczorowski 75, 07/09/2002 PR (GS) San Marino - Poland 0-2 Serravalle Kukiełka 88 FIFA World Cup Stage Date Match Result Venue Goalscorers reached Lesniak 52, 80, 19/05/1993 QR (GS) San Marino - Poland 0-3 Serravalle Warzycha 57 28/04/1993 QR (GS) Poland - San Marino 1-0 Lodz Furtok 71 Final Qualifying Total tournament Home Away Pld W D L Pld W D L Pld W D L Pld W D L GF GA Total San Marino 4 0 0 4 4 0 0 4 - - - - 8 0 0 8 1 33 Poland 4 4 0 0 4 4 0 0 - - - - 8 8 0 0 33 1 2 San Marino - Poland Sunday 5 September 2021 - 20.45CET (20.45 local time) Match press kit San Marino Stadium, Serravalle Squad list San Marino Current season Overall Qual. -
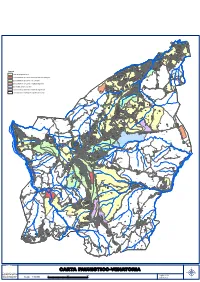
1:12.000 M U.G.R.A.A
Rovereta Dogana Fornace Falciano Ca' Valentino Campolungo Ranco Mauro Legenda Galazzano Ca' Ragni La Creta Oasi di ripopolamento Bosche Mondarco Saponaia Zanetta Zona di divieto di caccia - Riserva Naturale Integrale Torraccia Crete Ca' Marozzo Ponte Mellini Rancidello Zona di divieto di caccia - Area Parco Ca' Mercato Ca' Mazzola Piandolano Zona di divieto di caccia - Impianto Sportivo Rancaglia Cinque Vie Zona addestramento cani Olivella Ciarulla Zone di caccia destinate alla sola migratoria Molino Zone di caccia controllata e gestione sociale Serravalle Sant' Andrea Laiala Poggio Ruggine Ca' Baldino Coste Casvir Laghi Monte Olivo Le Tane Ca' Borgo San Michele Lesignano Grotte Valle Giurata Rancione Seggiano Fiorina Lagucci Ranco Pozzo delle Campore Ventoso Il Benefizio Cailungo di Sotto Ca' Tabarrino Serra Macero Serra Paradiso Paderna La Schiera Torraccia La Ciuffa Gualdicciolo Brugneto Toscana Ca' Giannino Ca' Carlo Ca' Gozi Ca' Taliano Il Grasso Gaviano Ca' Vagnetto Ca' Bartoletto Sterpeto Ginestre Molino dei Frati Moricce Ca' Riccio Ca' Amadore Cailungo di Sopra Domagnano Ca' Melone Montelupo Brandolina Fiumicello Tavolucci Valdicella Ca' Bertone Ca' Baudasso Ca' Martino Campagnaccio Acquaviva La Morra Il Fosso Monte Cerreto Colombaia Calintufo Bottaccione Piandavello Ca' Bugli Casetti Boschetti Molino della Genga Poggiolo Fiumicello Ca' Nino Casetta Valdragone Sotto Corianino Molino Magi Bigelli Gengone Vignale Baldasserona Fornace Borgo Maggiore Serrate Caitasso La Chiesuola Montalbo La Costa Cerreto Gaggio Ca' Moraccino Friginetto -

XII Mediterranean Cup San Marino 3/6 October 2019 Silver Qualification Event
XII Mediterranean Cup San Marino 3/6 October 2019 Silver Qualification Event Competition Rules and Regulations XII Mediterranean Cup San Marino 3/6 October 2019 Silver Qualification Event 1 - Venue Competitions will take place at the CONS gym - Multieventi Sport Domus in San Marino; training venue is in the same place Multieventi Sport Domus. 2 - Accommodation Two hotels will be at the disposal of delegations, “HOTEL I DESIGN” (Murata, San Marino) and “PALACE HOTEL” (Serravalle San Marino), Grand Hotel Primavera (Borgo Maggiore). The headquarter will be arranged at the Palace Hotel (via Cinque Febbraio, 47899, Serravalle San Marino. Tel +378 900190). How to get to San Marino: San Marino is connected to the Italian A14 highway, exit RIMINI SUD. The nearest airport is in Bologna, Italy, 120km from San Marino. 3 - Competition Rules and Regulations The competition is held in accordance with IWF Technical and Competition Rule&Regulations (TCRR). Eligibility Participating athletes must be 15 years of age and over (year of birth 2004 of earlier). With reference to article 5.6.5 of the IWF Antidoping Policy 2018, an athlete who is not listed on IWF’s registered testing pool but wishes to participate in an IWF event shall provide accurate and complete whereabouts information as set out ay Annex 1 of the international standard for testing and investigation for a period of at least two months prior to the IWF events in question (by august 04). An Athlete does not comply with this provision is not eligible to compete at the IWF event. Bodyweight Categories The ten categories M+W are eligible to compete. -

Ati San Marino
AZIENDA AUTONOMA DI STATO PER I SERVIZI PUBBLICI REPUBBLICA DI SAN MARINO ORARIO AUTOLINEE TRASPORTI INTERNI - AGGIORNATO A MARZO 2017 1 CITTÀ P9 CONFINE CONFINE CITTÀ P9 CITTÀ CENTRO CITTÀ EX STAZIONE MURATASTUDI FIORENTINO TEGLIO CHIESANUOVA CHIESANUOVA TEGLIO FIORENTINO MURATA EX STAZIONE 7.05 7.08 7.12 / 7.15 7.22 7.24 7.26 7.30 7.35 7.39 7.49 7.51 7.56 8.00 11.30 11.33 11.37 / 11.40 11.47 11.50 11.55 12.05 12.07 12.09 12.18 12.20 12.23 12.25 12.50 12.53 12.57 13.00 13.10 13.17 13.20 13.25 14.00 14.03 14.05 14.15 14.20 14.25 / 13.00 13.03 13.05 / 13.07 13.15 13.17 13.20 14.30 14.33 14.35 14.45 14.47 14.50 14.55 13.45 13.48 13.52 / 13.55 14.02 14.04 14.05 17.35 17.38 17.40 17.47 17.50 17.55 18.00 17.05 17.08 17.12 / 17.15 17.22 17.25 17.30 18.30 18.33 18.35 18.42 18.45 18.48 18.53 18.05 18.08 18.10 / 18.15 18.20 18.25 18.30 Coincidenza con CIRCOLARE 3d Coincidenza con CIRCOLARE 3s Estivo Il sabato questa corsa non sarà effettuata solo nel periodo invernale 2 CITTÀ P9 MOLARINI MOLARINI CITTÀ P9 CITTÀ CENTRO BORGO BORGO CENTRO CITTÀ EX STAZIONE MURATA STUDI MAGGIORE VENTOSO GUALDICCIOLO GUALDICCIOLO VENTOSO MAGGIORE MURATA STUDI EX STAZIONE 6.25 6.28 6.30 / 6.33 6.38 6.50 6.55 7.10 7.15 7.35 7.40 7.43 7.45 7.52 7.55 7.55 / / / 8.00 8.05 8.15 8.20 7.25 7.30 7.45 7.50 7.55 / 7.58 7.59 11.20 11.25 11.28 / 11.31 11.36 11.49 11.55 9.00 9.05 9.20 9.25 9.28 / 9.35 9.40 12.50 12.55 12.58 13.00 13.10 13.15 13.30 13.35 12.05 12.10 12.20 12.25 12.28 / 12.35 12.40 13.00 13.03 13.05 / 13.10 13.15 13.25 13.30 14.10 14.13 14.25 14.30 14.33 / 14.40 -

N. Tipo Utilizzo Ubicazione Nr. Fogli O Nr. Part Nr. Sub Canone Annuale 1
IMMOBILI ECC.MA CAMERA CEDUTI IN LOCAZIONE FABBRICATI E TERRENI NON AD USO AGRICOLO Rif. Catastali Nr. Nr. Nr. Canone N. Tipo Utilizzo Ubicazione Fogli Part Sub Annuale o 1 VIA DEL GENGONE, 9 1 APPARTAMENTO 31 866 2 2.344,36 47893 - BORGO MAGGIORE 3 PIAZZA MARINO TINI, 23 2 TERRENO 2 8.139,60 47891 - DOGANA VIA DEL SERRONE, 69 1 3 TERRENO 45 299 12.563,93 47890 - MURATA 2 VIALE DEL CIMITERO, 10 4 TERRENO 28 506 690,36 47890 - SANTA MUSTIOLA VIA OVELLA, 20 5 CAPANNONE 30 781 2 9.000,00 47893 - VALDRAGONE 781 3 STRADA SERRABOLINO, 89 6 CAPANNONE 30 1 27.000,00 47893 - BORGO MAGGIORE 105 2 VIA DELLE CARRARE, 17 7 TERRENO 54 relitto stradale 21,17 47890 - MURATA VIA GUARDIA DI ROCCA, 14 8 TERRENO 3 370 644,33 47899 - SERRAVALLE VIA TONNINI, 17 1 9 APPARTAMENTO 42 179 1.828,56 47890 - SAN MARINO CITTA' 2 STR. DEI SERALLI, 2A 10 TERRENO 48 559 57,53 47896 - FAETANO VIA MARCADANTE, 7 11 TERRENO 17 565 90,30 47892 - ACQUAVIVA VIA CINQUE FEBBRAIO, 194 12 TERRENO 13 991 115,05 47899 - SERRAVALLE 32 VIA DEL DRAGONE, 7 13 APPARTAMENTO 66 33 2 6.242,40 47898 - MONTEGIARDINO 34 3 VIA LA TOSCANA 14 TERRENO 21 950 56,44 47893 BORGO MAGGIORE VIA LA TOSCANA 15 TERRENO 21 951 57,53 47893 BORGO MAGGIORE 485 VIA PRATO DELLE VALLI 16 TERRENO 19 486 345,17 47892 - ACQUAVIVA 487 VIA 5 FEBBRAIO, 149 17 TERRENO 13 419 210,33 47899 - SERRAVALLE VIA GUARDIA DEL CONSIGLIO, 18 TERRENO 32 3 443 2.071,07 47899 - SERRAVALLE VIA DEL SERRONE, 65 19 BAR 47890 - MURATA - SAN 45 127 2.500,00 MARINO 1 Rif. -

Variante Di Piano Regolatore Generale Approvate Successivamente All’Entrata in Vigore Della Predetta Legge N.126/1995
REPUBBLICA DI SAN MARINO Noi Capitani Reggenti la Serenissima Repubblica di San Marino Visto l’articolo 4 della Legge Costituzionale n.185/2005 e l’articolo 6 della Legge Qualificata n.186/2005; Promulghiamo e mandiamo a pubblicare la seguente legge ordinaria approvata dal Consiglio Grande e Generale nella seduta del 30 aprile 2010: LEGGE 5 MAGGIO 2010 N.81 MODIFICHE ALLA LEGGE 29 GENNAIO 1992 N. 7 - PIANO REGOLATORE GENERALE (P.R.G.) PER L’ATTUAZIONE DI INTERVENTI A FAVORE DELLE IMPRESE E PER LA REALIZZAZIONE DI INFRASTRUTTURE PUBBLICHE Art.1 1. Gli allegati B e C della Legge 29 gennaio 1992 n.7 (Piano Regolatore Generale) sono modificati in conformità a quanto previsto al comma 2. 2. Le particelle, situate in Serravalle, località Ciarulla, contraddistinte al Foglio di Mappa 10, n.15 (in parte), n.459, n.460, n.461, n.462 (in parte), n.490, n.491, n.514 (in parte) ed alle Strade Pubbliche del Foglio di Mappa 3 e 10 (in parte), destinate sulla tavola di Piano Regolatore Generale a “Zone per i Servizi - sp” (articolo 48 della Legge n.7/1992), sono trasformate in “Zone D1:aree produttive a Piano Particolareggiato” (articolo 41 della Legge n.7/1992), il tutto come rappresentato nell’Allegato “A” della presente legge. Art. 2 1. Gli allegati B e C della Legge 29 gennaio 1992 n.7 (Piano Regolatore Generale) sono modificati in conformità a quanto previsto ai commi successivi. 2. Le particelle situate in Serravalle, località Ciarulla, contraddistinte al Foglio di Mappa 13, n.44 e n.520, destinate sulla tavola di Piano Regolatore Generale a “Zone E:aree agricole” (articolo 43 della Legge n.7/1992), sono trasformate in “Zone D1:aree produttive a Piano Particolareggiato” (articolo 41 della Legge n.7/1992). -

Elenco Strade Della Repubblica Di San Marino
San Marino lì 16/07/2012 Elenco Strade della Repubblica di San Marino CodVia Urbanistico via cap Castello 20112 98717 ACQUAVIVA -RSM- 47892 ACQUAVIVA 20066 34834 CENTRO GUALDICCIOLO 47892 ACQUAVIVA 20017 8305 LOC. CA' AMADORE 47892 ACQUAVIVA 20028 10203 LOC. CA' NINO 47892 ACQUAVIVA 20029 10212 LOC. CA' PAOLETTO 47892 ACQUAVIVA 20027 10197 NUCLEO CA'MURACCINO 47892 ACQUAVIVA 20032 10681 NUCLEO CA'TABARRINO 47892 ACQUAVIVA 20065 34342 NUCLEO IL GRASSO 47892 ACQUAVIVA 20011 396 VIA ACQUAVIVA PAESE 47892 ACQUAVIVA 20072 46244 VIA MOLINO GENGA 47892 ACQUAVIVA 10957 73040 COSTA DEL SANTO 47892 ACQUAVIVA 284 68893 COSTA DELLO SPINO 47892 ACQUAVIVA 20002 33 IRREPERIBILE 47892 ACQUAVIVA 1030 80008 PARCO DELLE FONTANE AZZURRE 47892 ACQUAVIVA 1031 80011 PARCO MARINO NICOLINI PRIMO MAESTRO 47892 ACQUAVIVA 788 36564 PIAZZA CASTELLO MONTECERRETO 47892 ACQUAVIVA 1025 80002 PIAZZALE CAVA DELLA FONTE 47892 ACQUAVIVA 1029 80007 PIAZZALE IL CASTAGNETO 47892 ACQUAVIVA 789 36630 PONTE DEI MULINI 47892 ACQUAVIVA 286 8273 STRADA CA' AMADORE 47892 ACQUAVIVA 267 8901 STRADA CA' BIGIO 47892 ACQUAVIVA 268 14290 STRADA CAPOGLIETTO 47892 ACQUAVIVA 301 5753 STRADA DEL BIANCOSPINO 47892 ACQUAVIVA 293 23742 STRADA DEL COLOMBARO 47892 ACQUAVIVA 302 37048 STRADA DEL LAVORO 47892 ACQUAVIVA 269 57134 STRADA DEL RE 47892 ACQUAVIVA 285 73729 STRADA DEL VIGNALE 47892 ACQUAVIVA 474 24585 STRADA DELLA CRETA ROSSA 47892 ACQUAVIVA 281 47751 STRADA DELLE MORICCE 47892 ACQUAVIVA 10270 31790 STRADA DI GAVIANO 47892 ACQUAVIVA Pag. 1 di 42 San Marino lì 16/07/2012 Elenco Strade della -

Zona N° 1 Acquaviva–Gualdicciolo-Chiesanuova- Fiorentino-Capanne
San Marino 12-04-2018 Programma di intervento di disinfestazione indirizzato contro Aedes Albopictus predisposto in base Ai monitoraggi effettuati sul Territorio dal personale dell’U.G.R.A.A.e verificati dal S.I.A. ZONA N° 1 ACQUAVIVA–GUALDICCIOLO-CHIESANUOVA- FIORENTINO-CAPANNE ACQUAVIVA-GUALDICCIOLO • VIA BIGELLI • STRADA DELLA BALDASSERONA • VIA GENGHE DI ATTO ZONA PARCO • VIA GUIDUCCIO • CIMITERO • STRADA DEL COLOMBARO • STRADA MOLINO MAGI • STRADA MOLINO GENGA • VIA NITELLA (SCUOLE) • STRADA DELLA MARGHERITINA • VIA DEGLI ACERI • STRADA LAMATICCIE (FOSSO DEL RE ) • VIA FABRIZIO DA MONTEBELLO • STRADA DEL LAVORO CHIESANUOVA • CIMITERO • VIA SOLAIOLO (CHIESA-SCUOLE) • PARCHEGGIO DI FIANCO ALLA PIAZZA • BENTIVEGNA DELLA VALLE ZONA CAMPO SPORTIVO FIORENTINO • PIAZZA XII OTTOBRE • CIMITERO • VIA G.CORBELLI (SCUOLE) • VIA LA RENA • VIA ZANONE • VIA VASCONE PARCO • ZONA GUALDRE MONTEGIARDINO • VIA DELLA BANDIROLA (PARCO) • VIA SALICE PARCO (SCUOLA) • STR..DELLE MACCHIE ZONA PONTICELLO ZONA N° 2 FAETANO–CAILUNGO-SERRAVALLE-TORRACCIA FAETANO • STRADA DI MAIANO • STRADA FOSSO DI TANCREDI (ZONA MENSA) • VIA PRIMO MAGGIO • STRADA CAMPO DEL FIUME • VIA TONSO DI GUALTIERO • STRADA DEL MARANO • C .VILLANI SCUOLE ELEMENTARI CORIANINO • CIMITERO • PIAZZA MASSARO • VIA CALCINELLI CAILUNGO • VIA VILLA DI SOPRA • VIA PRADACCI • VIA DOMOPORA • Via VERNIE • VIA TONACCI • VIA LA TOSCANA • VIA A. DI SUPERCHIO • STRADA SAN MICHELE • STRADA DEI BUGARI ZONA PONTE • VIA ZUCCARI • VIA FURINI • VIA PALMA IL GIOVANE • VIA DELLA QUERCIA FERITA SERRAVALLE • VIA -

LEGGE 14 Marzo 1997 N.36
LEGGE 14 marzo 1997 n.36 Regolamento per la disciplina della campagna elttorale Noi Capitani Reggenti la Serenissima Repubblica di San Marino Promulghiamo e mandiamo a pubblicare la seguente legge approvata nella seduta del Consiglio Grande e Generale del 14 marzo 1997. Art.1 1. La campagna elettorale è aperta il ventesimo giorno precedente a quello delle elezioni e cessa alle ore 24.00, del secondo giorno antecedente a quello delle elezioni. 2. Prima e dopo il termine di cui al primo comma è vietata ogni forma di propaganda elettorale con qualsiasi mezzo la stessa sia attuata. Art.2 Dalla data di apertura della campagna elettorale, di cui all'articolo 1, l'affissione di stampati, giornali murali od altro, di figure o immagini rappresentative del pensiero e di manifesti che, attraverso qualunque forma, costituiscano manifestazione di propaganda elettorale, è consentita esclusivamente negli spazi a ciò destinati nel territorio dei singoli Castelli e con l'osservanza delle norme di cui al presente regolamento. Art.3 1. La Commissione Elettorale di cui all'articolo 6 della Legge Elettorale, entro il cinquatesimo giorno successivo a quello di convocazione dei comizi elettorali, stabilisce, attraverso tabelloni di dimensioni uniformi da collocare nei singoli Castelli, gli spazi destinati all'affissione del materiale di cui all'articolo 2, attenendosi alle seguenti indicazioni: CASTELLO DI SAN MARINO - CITTA' Città: n. 5; Castellaro: n.1; Casole: n.1; Canepa: n.1; Cà Berlone: n.1; Santa Mustiola: n.1; Montalbo: n.1; Murata: n. 1. CASTELLO DI BORGO MAGGIORE Borgo Maggiore: n.2; Valdragone (di sopra): n.1; Valdragone (di sotto): n.1; Cà Melone: n.1; Cailungo (di sopra): n.1; Cailungo (di sotto): n.1; Ventoso: n.1; San Giovanni: n.1; Cà Rigo: n.1. -

Orari E Percorsi Della Linea Bus 4
Orari e mappe della linea bus 4 4 Città Visualizza In Una Pagina Web La linea bus 4 (Città) ha 3 percorsi. Durante la settimana è operativa: (1) Città: 10:10 - 18:40 (2) Città - Ex Stazione: 07:20 (3) Rovereta: 06:45 - 18:05 Usa Moovit per trovare le fermate della linea bus 4 più vicine a te e scoprire quando passerà il prossimo mezzo della linea bus 4 Direzione: Città Orari della linea bus 4 45 fermate Orari di partenza verso Città: VISUALIZZA GLI ORARI DELLA LINEA lunedì 10:10 - 18:40 martedì 10:10 - 18:40 Dogana - Rovereta mercoledì 10:10 - 18:40 Rovereta giovedì 10:10 - 18:40 Strada Rovereta venerdì 10:10 - 18:40 Strada Rovereta, Cerasolo sabato 10:10 - 18:40 Via Dei Paceri Via dei Pacieri, Cerasolo domenica Non in servizio Falciano - Paceri Via Rivus Falzani Informazioni sulla linea bus 4 Via Dei Paceri Direzione: Città Fermate: 45 Falciano - Bargello Durata del tragitto: 39 min Strada del Bargello, Serravalle La linea in sintesi: Dogana - Rovereta, Rovereta, Strada Rovereta, Via Dei Paceri, Falciano - Paceri, Via Strada Del Bargello Rivus Falzani, Via Dei Paceri, Falciano - Bargello, Strada Del Bargello, Via Giuseppe Badolini, Dogana Via Giuseppe Badolini Bassa - Consiglio Dei Sessanta, Dogana Bassa - Campolungo, Via Consiglio Dei Sessanta, Serravalle - Centro Atlante, Serravalle - Ponte Mellini, Via IV Dogana Bassa - Consiglio Dei Sessanta Giugno, Serravalle - Sovrapasso, Via Quattro Giugno, Via Cinque Febbraio, Domagnano - Fiorina Santolini, Dogana Bassa - Campolungo Domagnano - Fiorina Hotel Gasperoni, Via Cinque Via Campolungo, Serravalle Febbraio, Via Ornera, Domagnano - Giannoni, Domagnano - Carducci, Domagnano - Meridiano, Via Consiglio Dei Sessanta Domagnano - Chiesa, Domagnano - Gualdaria, Via Venticinque Marzo, Borgo Maggiore - Tavolucci, Serravalle - Centro Atlante Borgo Maggiore - Piscina, Borgo Maggiore - Casetti, Via Quattro Giugno, Serravalle Via Ventotto Luglio, Strada Sottomontana, Strada Sottomontana, San Marino - Bivio S.