Neurophysiologic Pattern and Severity Grading Scale of Carpal Tunnel
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
AAHS New Objective Grading System to Provide Prognostic Value To
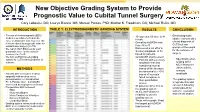
New Objective Grading System to Provide Prognostic Value to Cubital Tunnel Surgery Cory Lebowitz, DO; Lauryn Bianco, MS; Manuel Pontes, PhD; Mitchel K. Freedman, DO; Michael Rivlin, MD INTRODUCTION TABLE 1: ELECTRODIAGNOSTIC GRADING SYSTEM RESULTS CONCLUSION • The use of electrodiagnostic (EDX) • • 101 patients; 60 male & 41 Electrodiagnostic studies is well documented on its female studies not only aid a value as diagnostic tool, however, little clinical diagnosis of is known about its prognostic value for • Overall quickDASH went from 38 to 41 CuTS but can cubital tunnel surgery (CuTS) provide a framework • We report which EDX results yield • Discovered a cut off of a for the outcome of prognostic value for the surgical Sensory Amplitude of 38 treatment for CuTS based on patients surgery • We form an EDX based grading quickDASH improvement • system for CuTS that is predictive of • Patients with a sensory Specifically when outcome amplitude that was looking at the considered normal MCV across the METHODS based off the literature elbow with the but abnormal (i.e <38) sensory • Patients with CuTS were treated based off our data amplitude surgically with an ulnar nerve failed to improve in decompression +/- transposition their quickDASH • The grading system • Pre & Postoperative quickDASH scores is reproducible and scores and demographics reviewed • 97 patients (96%) fit in to can aid in following • Preoperative EDX reviewed: similar patient for • EMG the grading system • 93.8% inter-observer outcome evaluation • Motor Amplitudes and clinical studies • Motor Conduction Velocities reliability to use the • Sensory Amplitude grading system • Conduction Block • Those with a grade 3 had • Grading system constructed solely on the largest quickDASH EDX: nerve conduction studies and improvement electromyography variable. -

Electrophysiological Grading of Carpal Tunnel Syndrome
ORIGINAL ARTICLE Electrophysiological Grading of Carpal Tunnel Syndrome MUHAMMAD WAZIR ALI KHAN ABSTRACT Background: Carpal Tunnel Syndrome (CTS) is the most common entrapment neuropathy caused by a conduction block of distal median nerve at wrist. Women are affected more commonly than men. Clinical signs are quite helpful in diagnosis but electrophysiological tests yield accurate diagnosis and severity grading along with follow-up and management. Aim: To utilize nerve conduction studies (NCS) to diagnose carpal tunnel syndrome and further classify its severity according to the AAEM criteria. Methods: This descriptive study was conducted at the Department of Neurology, Sh. Zayed Medical College/Hospital, Rahim Yar Khan from June 2013 to Dec 2014. Overall, 90 patients and 180 hands were evaluated through nerve conduction studies. Patients with clinically high suspicion of CTS were included for NCS. Clinical grading was done using the AAEM criteria for CTS. Other variables like duration of symptoms, handedness, bilateral disease and gender were noted. Mean and median were calculated for age of the patients. Results: Ninety patients and 126 hands were identified with carpal tunnel syndrome. Most patients (80%) were females with age range from 19 to 75 years. More than one third had bilateral disease. Dominant hand was involved in majority of the patients. Most patients had (42.8%) severe CTS as per AAEM criteria. Also duration of symptoms directly correlated with severity of disease. Conclusion: Nerve conduction study is a valuable tool in accurate diagnosis and grading of carpal tunnel syndrome. Keywords: Phalen sign, Tinel Sign, electrophysiology, median nerve INTRODUCTION 4,5,6 electrophysiological findings, are quite valuable . -

CHAPTER 9. SITE DEVELOPMENT Article 1. Grading, Excavation and Filling Sec
Walnut Creek Municipal Code TITLE 9. BUILDING REGULATIONS CHAPTER 9. SITE DEVELOPMENT CHAPTER 9. SITE DEVELOPMENT Article 1. Grading, Excavation and Filling Sec. 9-9.01. Purpose. It is the declared intent of the City of Walnut Creek to promote the conservation of natural resources, including the natural beauties of the land, streams and water sheds, hills and vegetation, and as described in Sec. 10-2.1301 of the Walnut Creek Municipal Code and Government Code §65560(b) (1) to protect the health and safety, including the reduction or elimination of the hazards of earth slides, mud flows, rock falls, undue settlement, erosion, siltation and flooding, or other special conditions as described in Government Code §65560(b) (4) by minimizing the adverse effects of grading, cut and fill operations, water runoff and soil erosion. Therefore, the following regulatory provisions of this chapter are hereby adopted for the purpose of stringent control of all aspects of grading operations. (§1, Ord. 1193, eff. December 26, 1973) Sec. 9-9.02. Permits Required. No person shall do any grading without first having obtained a grading permit from the City except for the following: a. An excavation below finished grade for basements and footings of a building, retaining wall, swimming pool or other structure authorized by a valid building permit. This statement shall not exempt from permit requirements any fill made with the material from such excavation nor exempt any excavation having an unsupported height greater than five feet after the completion of such structure; b. Cemetery graves; c. Refuse disposal sites controlled by other regulations; d. -

Section 31 22 13 ‐ Site Grading
University of Houston Master Construction Specifications Insert Project Name SECTION 31 22 13 ‐ SITE GRADING PART 1 ‐ GENERAL 1.1 SCOPE OF WORK A. This Section pertains to the earthwork generally consisting of excavation, filling, backfilling and subgrade preparation as required for construction of site retaining walls/structures, slab on grade walks, pavement surfaces, landscaped areas and the general shaping of the site as shown, described or reasonably inferred on the drawings. B. Subsurface data is available from the *Owner. Contractor is urged to carefully analyze the site conditions. C. This section excludes work necessary for building pad preparations. Work within the building footprint and surrounding 5 feet shall be accomplished under technical specification 31 23 00 Excavation and Fill prepared by *STRUCTURAL ENGINEER]. D. Construction Means, Methods, Techniques, Sequences and Procedures: 1. The Contractor is solely responsible for, and has sole control over, construction means, methods, techniques, sequences and procedures, and for coordinating all portions of the Work. 2. Shoring that is required to complete the Work, is considered a method or technique and is the sole responsibility of the Contractor. If a regulatory agency requires a licensed engineer to design, approve or provide drawings for shoring, then it is the sole responsibility of the Contractor to engage the services of a qualified Engineer for shoring design services. 1.2 RELATED WORK SPECIFIED ELSEWHERE A. Drawings and general provisions of the Contract, including A‐procurement and Contracting Requirements, Division 00 and Division 01 apply to this section. B. Section 31 11 00 Clearing and Grubbing C. Section 31 23 33 Trenching, Backfilling and Compaction D. -

Unsealed Road Grading Your Questions Answered
Unsealed Road Grading Your Questions Answered What is maintenance grading? Council grades unsealed roads to reshape and re-compact the road, to reduce lumps and bumps and ensure that the road will shed water away from the centre after rain. A grading maintenance schedule is adhered to every 6 or 12 months, depending upon the road condition, the amount of use and the effects of wet weather. What is gravel re-sheeting? Gravel re-sheeting is when new gravel is added to the road. This is due to the severe deterioration of the road that can compromise the safety of road users. The gravel is generally laid in loose layers and then trimmed and compacted using a grader, water cart and roller so that the new road generally has a depth of about 150mm. Why does my road lose gravel? Gravel wears away over time due to the combination of the environment (wetness and dryness), the type and volume of traffic and excessive traffic speed. Softer gravel rock will wear away faster than harder gravel rock. Unsealed roads are made up of a mixture of gravel of differing sizes, clay and soils. This mixture affects the strength of the pavement and how long it will last. The rock gives the pavement strength and the clay and other soils binds the gravel together. Where possible, the grader drivers will recover as much of the loose gravel as they can during the grading of a road and turn it from the edge back into the centre of the road. Why is does my road appear to be shrinking? As the road wears down over time the edges of the road pavement will wear and the width can become less. -

F Responses Studied with Single Fibre EMG in Normal Subjects and Spastic Patients1
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.41.1.45 on 1 January 1978. Downloaded from Journal ofNeurology, Neurosurgery, andPsychiatry, 1978, 41, 45-53 F responses studied with single fibre EMG in normal subjects and spastic patients1 H. H. SCHILLER AND E. STALBERG From the Department of Neurology, University Hospital, Zurich, Switzerland, and the Department of Clinical Neurophysiology, Academic Hospital, Uppsala, Sweden S U M M A R Y Recurrent responses of single human motor neurones after antidromic activation, the so-called F response, have been studied in the abductor digiti minimi muscle in normal subjects and in spastic patients with the single fibre EMG technique. The F response occurs rarely and in groups. Half of all motor neurones did not produce any F response within an arbitrarily chosen time interval of 200 successive stimuli at 1 and 2 Hz. Spastic patients had as many silent neurones as the normal subjects but the responding neurones more frequently produced F responses (P<0.001). When a neurone has few responses at rest the frequency increases under activation of the contralateral or ipsilateral muscle (P<0.05). When there are many responses in the relaxed state there is a decrease (P<0.001) under activation. The Protected by copyright. behaviour of an individual neurone is consistent in different activation periods. After stimulation of a peripheral nerve, a late response is always preceded by an identical response may be recorded with surface electrodes M response and has a jitter only slightly greater over the corresponding muscle at a latency of than that of the M response, usually less than about 20 to 30 ms in the upper extremities (Conrad 50 ,ts (Fig. -

Nerve Conduction Studies: Essentials and Pitfalls in Practice
NERVE CONDUCTION STUDIES: J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.2005.069138 on 16 June 2005. Downloaded from ESSENTIALS AND PITFALLS IN PRACTICE A Mallik, A I Weir ii23 J Neurol Neurosurg Psychiatry 2005;76(Suppl II):ii23–ii31. doi: 10.1136/jnnp.2005.069138 neurologist has sent a patient for nerve conduction studies (NCS) and has received the report, but what does it mean? We hope to remove some of the mysteries that may Asurround NCS. The techniques and how they are affected by disease are described in general terms. These principles can be applied to specific conditions discussed elsewhere. We also discuss the numerous pitfalls that may be encountered with NCS. Understanding these basic concepts will allow you to get the most from your clinical neurophysiology department. NCS are only part of a complete peripheral neurophysiological examination (PNE) and are frequently accompanied by a needle electromyogram (EMG). The combination of both techniques and those detailed in other articles in this issue are often required for a complete diagnostic study. The process of choosing the appropriate tests is the responsibility of the clinical neurophysiologist (CN) and not the referring doctor and is planned as a dynamic series of steps designed to answer specific questions about nervous system function raised by the clinical picture. c ABBREVIATIONS Clinical neurophysiologists can employ a confusing number of terms and abbreviations. Box 1 lists the ones we use frequently. WHAT DO YOU TELL THE PATIENT ABOUT THE TESTS? NCS involve activating nerves electrically with small safe pulses over several points on the skin of copyright. -

Chapter 3 Earthwork
Topic #625-000-007 Plans Preparation Manual, Volume 1 January 1, 2016 Chapter 3 Earthwork 3.1 General ...................................................................................... 3-1 3.2 Classification of Soils ................................................................. 3-3 3.3 Cross Sections - A Design Tool .................................................. 3-3 3.4 Earthwork Quantities .................................................................. 3-4 3.4.1 Method of Calculating ................................................. 3-4 3.4.2 Earthwork Tabulation ................................................. 3-4 3.4.3 Earthwork Accuracy ................................................... 3-5 3.4.3.1 Projects with Horizontal and Vertical Controlled Cross Sections .......................... 3-5 3.4.3.2 Projects without Horizontal and Vertical Controlled Cross Sections .......................... 3-6 3.4.4 Variation in Quantities ................................................ 3-6 3.5 Earthwork Items of Payment ...................................................... 3-7 3.5.1 Guidelines for Selecting Earthwork Pay Items ............ 3-7 3.5.2 Regular Excavation .................................................... 3-8 3.5.3 Embankment .............................................................. 3-9 3.5.4 Subsoil Excavation ..................................................... 3-9 3.5.5 Lateral Ditch Excavation ............................................. 3-9 3.5.6 Channel Excavation ................................................ -

Fundamentals of Site Grading Design
188.pdf A SunCam online continuing education course Fundamentals of Site Grading Design by Joshua A. Tiner, P.E. 188.pdf Fundamentals of Site Grading A SunCam online continuing education course Table of Contents A. Introduction B. Basics • Background: • Existing Conditions: • Contour Lines: • Spot Elevations / Spot Grades: • Other Standard Annotations: • Slope • Plan Setup • Limit of Disturbance / Transition between Existing and New Grades • The Inverse Slope/Contour Calculation Method C. Design Parameters and Other Limitations • Design Parameters • Positive Drainage • Rules of Thumb o Maximum Access Drive Slope: 8% o Maximum Parking Lot Slope: 5% o Maximum Slope in Maintainable Grassed Landscaped Areas 3:1 o Maximum Slope in Stabilized Landscaped Areas 2:1 o Slopes exceeding 2:1 o Minimum Slope of Asphalt: 1.5% o Minimum Slope of Concrete: 0.75% o Minimum Slope of Concrete Curb: 0.75% o Loading Dock grading: 2.0% for 60’ • ADA Requirements • Cut-Fill Analysis • Rock Ledge walls D. Other Grading Features • Berms • Swales • Ridge Lines • Retaining Walls E. Problem Areas and Other Locations of Importance • Landscaped Islands and Peninsulas • ADA Parking Spaces • Longitudinal Islands with Sidewalks • Flush Ramps • Drainage Outfall Location • Setting the Finished Floor • Property Line grading F. Summary and Conclusion www.SunCam.com Copyright 2014 Joshua A. Tiner, P.E. Page 2 of 24 188.pdf Fundamentals of Site Grading A SunCam online continuing education course A. Introduction This course is developed to identify the fundamentals of site grading design to those who are not experienced with site grading design, as well as a refresher to anyone who has worked in Civil Engineering and/or Land Development. -
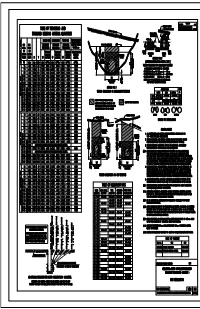
Table of Trenching and Standard Bedding Material
REVISIONS DESCRIPTION DATE GRADING TEMPLATE RE-ISSUE W/METRIC 1999 SPECS. TABLE OF TRENCHING AND STD. BACKFILL MATERIAL Recalc. Std. Bed. Dims. & Quants. lgc 7/99 GRADING TEMPLATE. STANDARD BEDDING MATERIAL QUANTITIES TOP OF INITIAL EMBANKMENT 600 600 SINGLE PIPE DOUBLE PIPE TRIPLE PIPE SPECIAL TRENCHING SINGLE, DOUBLE & PIPE PIPE STANDARD STANDARD STANDARD TRIPLE PIPE OPTIONS TOP OF INITIAL EMBANKMENT. DIAM. DIAM. TRENCHING TRENCHING TRENCHING W+300 mm NATURAL GROUND OR OR STANDARD STANDARD STANDARD ADD'L STANDARD 100 100 600 OR 150 EXCAVATION BACKFILL OR 150 DESIGN DESIGN ( MIN.) BEDDING BEDDING BEDDING BEDDING ELLIPTICAL PIPE PHASE PHASE 300 EQUIV. EQUIV. H T W MATERIAL W MATERIAL W MATERIAL MATERIAL (MIN.) CONDUIT. METHOD NO. 2 ( T ) WALL 3 3 3 3 ( OPTIONAL INSTALLATION FOR R. C. PIPE ) CONCRETE / METAL IN. mm mm mm mm m /m mm m /m mm m /m m /m THICKNESS 18 450 976 63 876 0.594 1401 0.846 1851 1.025 0.293 H TRENCH EXCAVATION IN EMBANKMENT SECTIONS MATERIAL. HEIGHT OF AVERAGE HEIGHT OF EMBANKMENT HEIGHT PRIOR TO EXCAVATION 24 600 1150 75 1200 0.938 2100 1.531 3000 2.125 0.345 TRENCH EXCAVATION. PIPE SIZES FROM 450 mm TO 1050 mm = = 750 mm 30 750 1326 88 1376 1.151 2501 1.969 3626 2.788 0.398 STANDARD BEDDING PIPE SIZES FROM 1200 mm TO 2100 mm = = 2/3 DIAMETER 36 900 1500 100 1850 1.825 3200 2.899 4550 3.974 0.450 W PIPE SIZES LARGER THAN 2100 mm = = 1500 mm 42 1050 1676 113 2026 2.117 3601 3.478 5176 4.839 0.503 METHOD NO. -

Preliminary Soils Reports Geotechnical Reports "As Graded" Soils Reports
APPENDIX A - Guidelines for: Preliminary Soils Reports Geotechnical Reports "As Graded" Soils Reports PRELIMINARY SOILS REPORTS A. GENERAL 1. Signature and professional registration number of project Geotechnical Engineer (G.E.) or Registered Civil Engineer (R.C.E.); 2. Job Address. 3. Location description and/or location index map with north arrow, bar scale, etc.; 4. Description of site conditions including topography, relief, vegetation index map with north arrow, ban, man-made features, drainage and watershed; 5. Proposed grading including general scope, amount, special equipment and/or methods if applicable; 6. Planned construction including type of structure and use, type of construction and foundation/floor system, number of stories. B. FIELD INVESTIGATION 1. Scope of work including date of work, investigative methods, logs of exploratory excavations, and real or assumed elevation of exploratory excavations for reference of soil materials and samples to finished grade or footing elevations. 2. Plan with legend including site limits, terrain features, man-made features, locations of exploratory excavations, soil of formational contacts, proposed improvements (including slopes with ratios, daylight lines, paving areas, retaining/crib walls, subdrains, overexcavation/cleanout/uncompacted fill areas). 3. Location of all surface and subsurface soil samples collected. 4. Ground water conditions and potential for future natural or artificial seepages. C. ENGINEERING/MATERIAL CHARACTERISTICS AND TESTING 1. Test methods used, type or condition of samples, applicable engineering graphics, results of all tests, and locations of all test samples. 2. Unified soil classification of materials. 3. Material competency and strength a. Field densities and moisture content, as well as relative compactions where pertinent. b. -

1 Section 32 90 00 Fine Grading and Soil
SECTION 32 90 00 FINE GRADING AND SOIL PREPARATION PART 1 ‐ GENERAL 1.01 SECTION INCLUDES A. Examination. B. Preparation. C. Subsoil Preparation. D. Placing Topsoil. E. Soil Tests. F. Coordination of Soil Amendments. G. Fine Grading. H. Tolerances. I. Field Quality Control J. Adjusting. K. Cleaning L. Protection. 1.02 REFERENCES A. Colorado Division of Labor Rules and Regulations: Excavation. B. State Department of Highways, Division of Highways, State of Colorado, Standard Specifications for Road and Bridge Construction, Section 207 of the latest edition. C. ANSI/ASTM D698 ‐ Test Methods for Moisture‐Density Relations of Soils and Soil‐Aggregate Mixtures, Using 5.5 lb (2.49 Kg) Rammer and 12 inch (304.8 mm) Drop. D. ANSI/ASTM D1556 ‐ Test Method for Density of Soil in Place by the Sand‐Cone Method. E. Association of Official Agricultural Chemists: Topsoil Analysis. 1.03 DEFINITIONS A. WEEDS: Includes Goatheads, Bindweed, Twitch, Dandelion, Jimsonweed, Quackgrass, Horsetail, Morning Glory, Rush Grass, Mustard, Lambsquarter, Chickweed, Cress, Crabgrass, Canadian Thistle, Nutgrass, Poison Oak, Blackberry, Tansy Ragwort, Bermuda Grass, Johnson Grass, Poison Ivy, Nut Sedge, Nimble Weed, Bindweed, Bent Grass, Wild Garlic, Perennial Sorrel, and Broom Grass. 1.04 SUBMITTAL PROCEDURES A. TOPSOIL TESTING: 1. After topsoil spreading, submit, for Architect's approval, topsoil samples and test results from: a. Each topsoil source. 2. Each location submission shall include: Great Work Montessori School FINE GRADING AND SOIL PREPARATION 32 90 00 ‐ 1 a. 1 qt. representative sample in air tight container. b. Agricultural analysis by a qualified soils laboratory made in accordance with “Methods of Soils Analysis – Agronomy #9” as published by the American Society of Agronomy, and testing will be done at the Contractor’s expense.