Assessing the Environmental Impacts of Urbanization in Siddharthanagar, Nepal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Logistics Capacity Assessment Nepal
IA LCA – Nepal 2009 Version 1.05 Logistics Capacity Assessment Nepal Country Name Nepal Official Name Federal Democratic Republic of Nepal Regional Bureau Bangkok, Thailand Assessment Assessment Date: From 16 October 2009 To: 6 November 2009 Name of the assessors Rich Moseanko – World Vision International John Jung – World Vision International Rajendra Kumar Lal – World Food Programme, Nepal Country Office Title/position Email contact At HQ: [email protected] 1/105 IA LCA – Nepal 2009 Version 1.05 TABLE OF CONTENTS 1. Country Profile....................................................................................................................................................................3 1.1. Introduction / Background.........................................................................................................................................5 1.2. Humanitarian Background ........................................................................................................................................6 1.3. National Regulatory Departments/Bureau and Quality Control/Relevant Laboratories ......................................16 1.4. Customs Information...............................................................................................................................................18 2. Logistics Infrastructure .....................................................................................................................................................33 2.1. Port Assessment .....................................................................................................................................................33 -

Integrated Urban Development Project- Siddharthanagar Municipality
Draft Initial Environmental Examination September 2011 NEP: Integrated Urban Development Project- Siddharthanagar Municipality Prepared by the Government of Nepal, Ministry of Physical Planning and Works for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 5 August 2011) Currency unit – Nepalese rupee (NRs/NRe) NRs1.00 = $0.01391 $1.00 = NRs 71.874 ABBREVIATIONS ADB - Asian Development Bank CBO - community building organization CLC - City Level Committees CPHEEO - Central Public Health and Environmental Engineering Organization CTE - Consent to Establish CTO - Consent to Operate DSMC - Design Supervision Management Consultant EAC - Expert Appraisal Committee EIA - Environmental Impact Assessment EMP - Environmental Management Plan GRC - Grievance Redress Committee H&S - health and safety IEE - initial environmental examination IPCC - Investment Program Coordination Cell lpcd - liters per capita per day MFF - Multitranche Financing Facility MSW - municipal solid waste NEA - national-level Executing Agency NGO - nongovernmental organization NSC - National level Steering Committee O&M - operation and maintenance PMIU - Project Management and Implementation Unit PSP - private sector participation SEA - State-level Executing Agency SEIAA - State Environment Impact Assessment Authority SIPMIU - State-level Investment Program Management and Implementation Units SPS - Safeguard Policy Statement TOR - terms of reference UD&PAD - Urban Development & Poverty Alleviation Department UDD - Urban Development Department ULB - urban local body WEIGHTS AND MEASURES dbA – decibels ha – hectare km – kilometer km2 – square kilometer l – liter m – meter m2 – square meter M3 – cubic meter MT – metric tons MTD – metric tons per day NOTE In this report, "$" refers to US dollars. This initial environmental examination is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. -

Short Listed Candidates for the Post
.*,ffix ryryffi-ffiffiWffir@fuffir. rySW{Jrue,€ f,rc, "*,*$,S* S&s#ery W€ryff$,,,SffWryf ryAeW Notice for the Short Listed Candidates applying in the post of "Trainee Assistantrr Details fot Exam: a. 246lestha,2076: Collection of Entrance Card (For Surrounding Candidates). b. 25nJestha, 2076: Collection of Entrance Card 8:00AM to 9:45AM in Exam Center (For Others). (Please carry Original Citizenship Certificate and l passport size photo). Written Test (Exam) : Date : 25'hJesth, 2076 Saurday (8ftJune, 2019). Time : 10:00 AM to 11:30 AM tVenue : Oxford Higher Secondary School, Sukhkhanagar, Butwal, Rupandehi. Paper Weightage : 100 Marks Composition Subjective Questions : 02 questions @ 10 marks = 20 marks Objective Questions : 40 questions @ 02 marks = B0 marks Contents 1,. General Banking Information - 10 objective questions @ 2 marks = 20 marks 2. Basic Principles & Concept of Accounting - 10 objective questions @2marks = 20 marks 3. Quantitative Aptitude 10 objective questions @ 2 marks = 20 marks 4. General ISowledge - 10 objective questions @ 2 marks = 20 marks (2 Subjective questions shall be from the fields as mentioned above). NOTE: ,/ I(ndly visit Bank's website for result and interview notice. For Futther Information, please visit : Ffuman Resource Department Shine Resunga Development Bank Limited, Central Office, Maitri Path, But'ural. enblrz- *rrc-tr fffir tarmrnfrur *ffi ffi{" ggffrus gevrcgemmrup w mes'g:iwme ffiAru${ frffi. S4tq t:e w r4r4.q klc S.No. Name of Applicant Address 7 Aakriti Neupane Sainamaina-03, M u reiva RuoanriEh] -

SASEC Road Improvement Project
Social Monitoring Report Semiannual Report (July-December 2018) January 2019 NEP: SASEC Road Improvement Project Prepared by Department of Roads, Project Directorate (ADB), for Ministry of Physical Infrastructure & Transport and the Asian Development Bank. This social monitoring report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. pGovernment of Nepal Ministry of Physical Infrastructure and Transport DEPARTMENT OF ROADS Project Directorate (ADB) Bishalnagar, Kathmandu, Nepal CONSULTANCY SERVICES FOR CONSTRUCTION SUPERVISION OF SASEC ROADS IMPROVEMENT PROJECT (SRIP) (ADB Loan No.: 3478-NEP) SEMI-ANNUAL REPORT NO. 3 (SOCIAL MONITORING) SASEC Roads Improvement Project Package 1: EWH- Narayanghat Butwal Road, Section I (64.425 Km) Package 2: EWH- Narayanghat Butwal Road, Section II (48.535 Km) Package 3: Bhairahawa – Lumbini - Taulihawa Road, (41.130 Km) (July - December) 2018 Submitted by M/S Korea Engineering Consultants Ltd. Corp.- MEH Consultant (P) Ltd., Kyong Dong Engineering Co. Ltd. JV In association with MULTI – Disciplinary Consultants (P) Ltd. & Seoul, Korea. SOIL Test (P) Ltd. SEMI-ANNUAL (SOCIAL MONITORING) REPORT 3 July - December 2018 Social Monitoring Report Semi-Annual Report No. 3 (July - December 2018) NEP: Loan No. 3478 SASEC Road Improvement Project (SRIP) Prepared by: Department of Roads, Project Directorate (ADB), for Ministry of Physical Infrastructure & Transport and the Asian Development Bank. -

The Gaze Journal of Tourism and Hospitality (2021) 12:1, 23-43 the GAZE JOURNAL of TOURISM and HOSPITALITY
The Gaze Journal of Tourism and Hospitality (2021) 12:1, 23-43 THE GAZE JOURNAL OF TOURISM AND HOSPITALITY Th e Impact of COVID-19 on Tourism: A Case Study of Lumbini, Nepal Bhim Bahadur Kunwar Lecturer, Lumbini Buddhist University, Lumbini [email protected] Article History Abstract Received 31 August 2020 Accepted 18 October 2020 Th is research aims to discover and present the impacts of COVID-19 in tourism in the context of Lumbini and its premises. As COVID-19 spread globally, it has created many challenges in health and security, daily lives, the national economy, and the global tourism industry. Th e COVID- 19 outbreak has been considered as the most challenging tragedy that occurred in the world aft er the 2nd world war. Keywords Th e World Health Organization (WHO) had listed Nepal also COVID-19, tourism, as a country with a high-risk zone of COVID-19.Th e travel Lumbini - Nepal, restriction and nationwide lock-down implemented by many insecurity, impacts countries including Nepal have resulted in a stranded traveler’s movement. As the consequences ticket reservation, fl ight services, transportation, hotel, and restaurants were closed and several job losses were registered in the tourism sector. Th e negative eff ects like fear, threat, frustration, and losing the confi dence of tourism entrepreneurs appeared. Th is has brought changes in the tourists’ behavior and their motivation to travel for the next few years. In Lumbini businesses like Corresponding Editor Ramesh Raj Kunwar lodges, hotels, restaurants, and travel offi ces were also severely [email protected] aff ected by the pandemic. -

List of Banks and Financial Institutions As of Mid Jul, 2019 (Licensed by NRB)
List of Banks and Financial Institutions As of Mid Jul, 2019 (Licensed by NRB) Class: "A" (Commercial Banks) (Rs. in Crore) Operation Paid up S.No. Name Head Office Working Area Date (A.D.) Capital 1 Nepal Bank Ltd. 1937/11/15 Dharmapath,Kathmandu 981.11 National Level 2 Agriculture Development Bank Ltd. 1968/01/21 Ramshahpath, Kathmandu 1444.82 National Level 3 Nabil Bank Ltd. 1984/07/12 Beena Marg, Kathmandu 901.18 National Level 4 Nepal Investment Bank Ltd. 1986/03/09 Durbarmarg, Kathmandu 1286.97 National Level 5 Standard Chartered Bank Nepal Ltd. 1987/02/28 Nayabaneshwor, Kathmandu 801.14 National Level 6 Himalayan Bank Ltd. 1993/01/18 Kamaladi, Kathmandu 852.03 National Level 7 Nepal SBI Bank Ltd. 1993/07/07 Kesharmahal, Kathmandu 844.93 National Level 8 Nepal Bangaladesh Bank Ltd. 1994/06/06 Kamaladi, Kathmandu 808.83 National Level 9 Everest Bank Ltd. 1994/10/18 Lazimpat , Kathmandu 810.69 National Level 10 Kumari Bank Ltd. 2001/04/03 Durbarmarg, Kathmandu 868.56 National Level 11 Laxmi Bank Ltd. 2002/04/03 Hattisar, Kathmandu 892.05 National Level 12 Citizens Bank International Ltd. 2007/04/20 Narayanhitipath, Kathmandu 837.11 National Level 13 Prime Commercial Bank Ltd. 2007/09/24 Kamalpokhari, Kathmandu 931.86 National Level 14 Sunrise Bank Ltd. 2007/10/12 Gairidhara, Kathmandu 815.26 National Level 15 Century Commercial Bank Ltd. 2011/03/10 Putalisadak , Kathmandu 841.55 National Level 16 Sanima Bank Ltd. 2012/02/15 Nagpokhari, Kathmandu 800.13 National Level 17 Machhapuchhre Bank Ltd. 2012/7/9* Lazimpat , Kathmandu 805.57 National Level 18 NIC Asia Bank Ltd. -

Revisit to Functional Classification of Towns in Nepal
The Geographical Journal of Nepal Vol. 10: 15-27, 2017 Central Department of Geography, Tribhuvan University, Kathmandu, Nepal Revisit to functional classification of towns in Nepal Chandra Bahadur Shresthaa, and Shiba Prasad Rijalb aSanepa, Lalitpur, Nepal; bDepartment of Geography Education, Tribhuvan University, Kirtipur, Kathmandu, Nepal; *Corresponding author Email: [email protected] The present study on functional classification of the towns in Nepal is a revisit to the study made in 1980 applying the similar methodology. The previous study was based on census data of 1971 and the present study on census data of 2011. The percentages of surplus labour force in proportion to national level were computed considering five activities groups involved in non-agricultural sectors. Then, the arithmetic means of each activity group were calculated and the standard deviations from the means were taken for measuring the functional specialization.The study revealed that both the degree of urbanization and level of functional specialization have considerably increased during a period of four decades. There were only 16 towns in 1971, which increased to 58 in 2011. The number of specialized towns has increased by six folds from 4 in 1971 to 26 in 2011. The level of urbanization has now been a prominent phenomenon as compared to that in 1971. In 1971, even the then large towns were with high agricultural labor force. Now, the proportion of agricultural labor force has declined considerably. However, agriculture labor forces constitute to be dominant in more than 15 smaller towns. It indicates that urban economic base is not being taken into account while incorporating places as municipalities in several cases. -
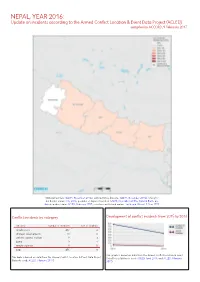
NEPAL, YEAR 2016: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 9 February 2017
NEPAL, YEAR 2016: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 9 February 2017 National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; China/In- dia border status: CIA, 2006; geodata of disputed borders: GADM, November 2015a; Natural Earth, un- dated; incident data: ACLED, February 2017; coastlines and inland waters: Smith and Wessel, 1 May 2015 Conflict incidents by category Development of conflict incidents from 2015 to 2016 category number of incidents sum of fatalities riots/protests 432 4 strategic developments 11 0 violence against civilians 9 3 battle 3 1 remote violence 1 0 total 456 8 This graph is based on data from the Armed Conflict Location & Event This table is based on data from the Armed Conflict Location & Event Data Project Data Project (datasets used: ACLED, April 2016, and ACLED, February (datasets used: ACLED, February 2017). 2017). NEPAL, YEAR 2016: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 9 FEBRUARY 2017 LOCALIZATION OF CONFLICT INCIDENTS Note: The following list is an overview of the incident data included in the ACLED dataset. More details are available in the actual dataset (date, location data, event type, involved actors, information sources, etc.). In the following list, the names of event locations are taken from ACLED, while the administrative region names are taken from GADM data which serves as the basis for the map above. In Central, 207 incidents killing 1 person were reported. The following locations were affected: Bhaktapur, Bharatpur, Bidur, Birganj, Bishrampur, Brahmapuri, Chandranigahapur, Chandrapur, Charikot, Chautara, Dharhari, Dhulikhel, Dhunche, Gamhariya Birta, Gaur, Gokarneshwar, Jaleswar, Janakpur, Kalaiya, Kamalamai, Kathmandu, Kirtipur, Kritipur, Madi, Mahottari, Malangwa, Patan, Rasuwa Ghadhi, Sanepa. -

Saath-Saath Project
Saath-Saath Project Saath-Saath Project THIRD ANNUAL REPORT August 2013 – July 2014 September 2014 0 Submitted by Saath-Saath Project Gopal Bhawan, Anamika Galli Baluwatar – 4, Kathmandu Nepal T: +977-1-4437173 F: +977-1-4417475 E: [email protected] FHI 360 Nepal USAID Cooperative Agreement # AID-367-A-11-00005 USAID/Nepal Country Assistance Objective Intermediate Result 1 & 4 1 Table of Contents List of Acronyms .................................................................................................................................................i Executive Summary ............................................................................................................................................ 1 I. Introduction ........................................................................................................................................... 4 II. Program Management ........................................................................................................................... 6 III. Technical Program Elements (Program by Outputs) .............................................................................. 6 Outcome 1: Decreased HIV prevalence among selected MARPs ...................................................................... 6 Outcome 2: Increased use of Family Planning (FP) services among MARPs ................................................... 9 Outcome 3: Increased GON capacity to plan, commission and use SI ............................................................ 14 Outcome -

Nepal General Evaluation 1
Nepal general evaluation 1 NEPAL A COUNTRY PROFILE Nepal is a land-locked country sandwiched between two neighbouring giants China (in the north) and India (in the east, south and west). One of the 49 Least Developed Countries (LDCs), with an annual per capita income of US$ 230, Nepal is ranked as 143rd (out of 175 countries) in the Human Development Index (HDI) of UNDP, and falls under the category of ‘low human development’ countries in the human development aggregates (UNDP 2003). Nepal, which stretches in an area of 147,181 sq km, is a land of enormous geographical diversity divided east-west into three distinct ecological zones: the plains (terai) on the south, hills and mountains in the middle and the Himalayas on the north. Thousands of rivers and streams that flow north-south bisect the landscape into hundreds of small hills and hillocks isolating the residents from each other and from the rapidly evolving world of information and development because of the lack of linking infrastructure (transport and communication). These three regions also display an immense diversity of human settlement patterns, population, land distribution, productive resources and levels of economic development. Home to nearly 24 million people, Nepal is a mosaic of over 61 ethnic groups who have their own distinct languages, cultures life styles. Officially, however, it is a Hindu State with a rigid caste system that compartmentalizes the people into 4-tire hierarchy. This caste framework finds a close nexus historically with the system of governance, in which the upper caste, the bahun and chhettri castes in particular, have always held the positions of power and privileges, and by virtue of their being in lower tiers, other groups are routinely discriminated against and deprived of accessing decisive State structures and institutions. -
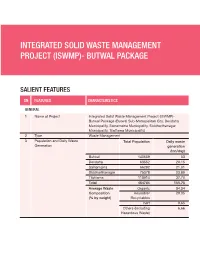
Integrated Solid Waste Management Project (Iswmp)- Butwal Package
INTEGRATED SOLID WASTE MANAGEMENT PROJECT (ISWMP)- BUTWAL PACKAGE SALIENT FEATURES SN FEATURES CHARACTERISTICS GENERAL 1 Name of Project Integrated Solid Waste Management Project (ISWMP)- Butwal Package (Butwal Sub-Metropolitan City, Devdaha Municipality, Sainamaina Municipality, Siddharthanagar Municipality, Tilottama Municipality) 2 Type Waste Management 3 Population and Daily Waste Total Population Daily waste Generation generation (ton/day) Butwal 140659 53 Devdaha 63552 20.15 Sainamaina 66282 21.01 Siddharthanagar 75378 23.89 Tilottama 118914 37.70 Total 464784 155.75 Average Waste Organic 54.34 Composition Reusable/ 29.35 (% by weight) Recyclables Inert 9.65 Others (Including 6.66 Hazardous Waste) SN FEATURES CHARACTERISTICS PROJECT LOCATION 1 Province Province 5 (Location Map) LAND AVAILABILITY 1 Butwal Sub-metropolitan city Bhanbhane basin in Shivapur community forest, ward number 9 of Butwal Sub-metropolitan city 2 Siddharthanagar Municipality Acquired land in Pattheuli in total area of 3.06 acres for landfill site. 3 Tilottama Municipality 14.01 Acres of land available PROJECT COMPONENT/TECHNOLOGY 1 Collection of waste n Household and commercial collection of waste on certain interval 2 Anaerobic Digestion n Mesophilic (35-38°C) / Thermophilic (above 50°C) n The methane gas will be compressed, bottled and sold to local market n Organic Fertilizer and Pesticide will be generated MARKET ASSESSMENT 1 Project Demand Scenario n There is a pressure on municipalities to Improve and modernize the collection methods and disposal technology. n There is a need to reduce the pressure on waste disposal practices and prices n 80% reduction in the current volume of waste going to landfill site which will extend the life of landfill site in the future. -

World Bank Document
Document of The World Bank FOR OFFICIAL USE ONLY Report No: 59291-NP Public Disclosure Authorized PROJECT APPRAISAL DOCUMENT ON A PROPOSED CREDIT IN THE AMOUNT OF SDR 8.80 MILLION (US$13.75 MILLION EQUIVALENT) AND A Public Disclosure Authorized PROSPOSED GRANT IN THE AMOUNT OF SDR 7.20 MILLION (US$11.25 MILLION EQUIVALENT) TO NEPAL FOR THE URBAN GOVERNANCE AND DEVELOPMENT PROGRAM: Public Disclosure Authorized EMERGING TOWNS PROJECT APRIL 6, 2011 Sustainable Development Department Urban and Water Unit South Asia Region This document has a restricted distribution and may be used by recipients only in the Public Disclosure Authorized performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective February 28, 2011) Currency Unit = NEPALESE RUPEES NPR1 = US$0.014 US$1 = NPR72.43 FISCAL YEAR July 16 – July 15 ABBREVIATIONS AND ACRONYMS ADB Asian Development Bank BOT Build Operate and Transfer CBO Community Based Organization CBS Central Bureau of Statistics CDO Chief District Officer DDC District Development Committee DTCO District Treasury Controller Office DUDBC Department of Urban Development and Building Construction ED Executive Director EO Executive Officer FNCCI Federation of Nepalese Chambers of Commerce and Industry GIZ Deutsche Gesellschaft für Internationale Zusammenarbeit GmbH GTZ Deutsche Gesellschaft für Technische Zusammenarbeit GmbH GON Government of Nepal ID Institutional Development IDA International Development Association IEG