Special Edition Inside
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Central Park
Hunter College Geology Field Trip Central Park Shruti Philips Field Trip stops in Central Park Stop #1 N Stop #2 Enter CP here on 5th Ave Stop #3 Between 66th Stop #2 and 67th street Field trip Stop #1 path Stop #3 Enter the Park from 5th Ave between 66th and 67th street Walk past the Billy Johnson Playground (on your right) and approach a small intersection. You will see a rock exposure ahead of you. Stop-1 Outcrop A Foliated metamorphic Rock Outcrop A Foliated metamorphic Rock STOP-1: Outcrop A The direction of foliation at stop-1 Click on the video to see the direction of foliation on a compass. This rock displays layering (foliation) on the outcrop scale as well as the hand specimen scale Foliation displays differential weathering Why do we see these high-grade metamorphic rocks on the surface in Central Park? A map of the world 449 Million years ago when the rocks in Central Park were forming Note that New York is ~20 0 S of the equator at that time. It was a shallow seafloor then accumulating sediments. How the rocks in Central Park formed and metamorphosed during the Paleozoic Era About 400 million year ago, this region was shallow sea floor, off the coast of the American Continent, and was the site of deposition of great thicknesses of sediment derived from the erosion of the nearby land (Fig. 1). Fig. 2: A new, convergent plate boundary developed here, along which ocean lithosphere was pushed under continental lithosphere (forming a subduction zone). -

Qualitative Changes in Ethno-Linguistic Status : a Case Study of the Sorbs in Germany
Qualitative Changes in Ethno-linguistic Status: A Case Study of the Sorbs in Germany by Ted Cicholi RN (Psych.), MA. Submitted in fulfilment of the requirements for the degree of Doctor of Philosophy Political Science School of Government 22 September 2004 Disclaimer Although every effort has been taken to ensure that all Hyperlinks to the Internet Web sites cited in this dissertation are correct at the time of writing, no responsibility can be taken for any changes to these URL addresses. This may change the format as being either underlined, or without underlining. Due to the fickle nature of the Internet at times, some addresses may not be found after the initial publication of an article. For instance, some confusion may arise when an article address changes from "front page", such as in newspaper sites, to an archive listing. This dissertation has employed the Australian English version of spelling but, where other works have been cited, the original spelling has been maintained. It should be borne in mind that there are a number of peculiarities found in United States English and Australian English, particular in the spelling of a number of words. Interestingly, not all errors or irregularities are corrected by software such as Word 'Spelling and Grammar Check' programme. Finally, it was not possible to insert all the accents found in other languages and some formatting irregularities were beyond the control of the author. Declaration This dissertation does not contain any material which has been accepted for the award of any other higher degree or graduate diploma in any tertiary institution. -

Recommended Methods for the Identification and Analysis of Fentanyl and Its Analogues in Biological Specimens
Recommended methods for the Identification and Analysis of Fentanyl and its Analogues in Biological Specimens MANUAL FOR USE BY NATIONAL DRUG ANALYSIS LABORATORIES Laboratory and Scientific Section UNITED NATIONS OFFICE ON DRUGS AND CRIME Vienna Recommended Methods for the Identification and Analysis of Fentanyl and its Analogues in Biological Specimens MANUAL FOR USE BY NATIONAL DRUG ANALYSIS LABORATORIES UNITED NATIONS Vienna, 2017 Note Operating and experimental conditions are reproduced from the original reference materials, including unpublished methods, validated and used in selected national laboratories as per the list of references. A number of alternative conditions and substitution of named commercial products may provide comparable results in many cases. However, any modification has to be validated before it is integrated into laboratory routines. ST/NAR/53 Original language: English © United Nations, November 2017. All rights reserved. The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. Mention of names of firms and commercial products does not imply the endorse- ment of the United Nations. This publication has not been formally edited. Publishing production: English, Publishing and Library Section, United Nations Office at Vienna. Acknowledgements The Laboratory and Scientific Section of the UNODC (LSS, headed by Dr. Justice Tettey) wishes to express its appreciation and thanks to Dr. Barry Logan, Center for Forensic Science Research and Education, at the Fredric Rieders Family Founda- tion and NMS Labs, United States; Amanda L.A. -

Chinese Terracotta Warriors
28 How Paul Janssen’s Drugs Saved the CCHHIINNEESSEE TTEERRRRAACCOOTTTTAA WWAARRRRIIOORRSS Rebecca J. Anderson The Chinese Terracotta Army, dating from approximately the late third century BCE, was discovered on March 29, 1974 to the east of Xi’an in Shaanxi Province, China. Photo: Shutterstock The Pharmacologist • March 2015 29 Chinese museum officials gazed with dismay at their Janssen label (3). These included repackaging and priceless army of ancient statues. For 22 centuries, the distributing generic penicillin and sulfonamides, which terracotta warriors had been protected and preserved in the were increasingly in demand after the war. Paul’s mother, soil of China’s Yellow River valley (1). Now, less than 20 Margriet Fleerakers, served as office manager and also years after these old soldiers emerged from their supervised the production line, including quality control (3). subterranean fortress, many of them had become infected Paul finished high school in 1943. To avoid forced and were suffering from a mysterious rash (2). Local labor in the German factories, he secretly enrolled in archeologists suspected the warriors’ moldy rash was due to college (at the age of 16) with the help of his uncle, Emiel fungi, but they lacked specialized laboratory equipment and Janssen (3). The 12 Jesuit teachers at the Faculté Notre- had only limited expertise to diagnose and treat the ailment. Dame de la Paix in Namur, Belgium, offered intensive The detective who stepped forward to solve this courses in physics, biology, philosophy, and chemistry to a mystery and thwart an archeological catastrophe was an handful of students, including Paul, without the knowledge unlikely hero: a businessman, physician, and scientist who of the German occupiers (2, 3). -
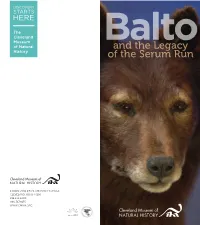
And the Legacy of the Serum Run
Baltoand the Legacy of the Serum Run 1 WADE OVAL DRIVE, UNIVERSITY CIRCLE CLEVELAND, OHIO 44106 216.231.4600 800.317.9155 WWW.CMNH.ORG Nome, Alaska, appeared on the map during one of the world’s great gold rushes at the end of the 19th century. Located on the Seward Peninsula, the town’s population had swelled to 20,000 by 1900 after gold was discovered on beaches along the Bering Sea. By 1925, however, much of the gold was gone and scarcely 1,400 people were left in the remote northern outpost. Nome was icebound seven months of the year and the nearest railroad was more than 650 miles away, in the town of Nenana. The radio telegraph was the most reliable means by which Nome could communicate with the rest of the world during the winter. Since Alaska was a U.S. territory, the government also maintained a route over which relays of dog teams carried mail from Anchorage to Nome. A one- way trip along this path, called the Iditarod Trail, took about a month. The “mushers” who traversed the trail were the best in Alaska. A RACE FOR LIFE JANUarY 27 The serum arrived in Nenana by train, and the relay to the On January 20, 1925, a radio signal went out, carried for stricken city began. “Wild Bill” Shannon lashed the life- miles across the frozen tundra: saving cargo to his sled and set off westward. Except for the Nom e c alling... dogs’ panting and the swooshing of runners on the snow, No m e c alling.. -

Speaker Bios
Moores UCSD Cancer Center Industry/Academia Translational Oncology Symposium Speaker Bios David R. Bentley, D.Phil. Vice President & Chief Scientist, Illumina, Inc. David Bentley, Ph.D., is Chief Scientist for Illumina’s Sequencing business. His major research interest is the study of human sequence variation. He was previously Head of Human Genetics and founding member of the Board of Management at the Wellcome Trust Sanger Institute where he played leading roles in the Institute’s contribution to the human genome referencing sequence, the SNP Consortium and the International HapMap Project. Dr. Bentley earned a degree in Natural Sciences from the University of Cambridge, took a DPhil at the University of Oxford, and is currently a Fellow of the Academy of Medical Sciences. Clara D. Bloomfield, M.D. Distinguished University Professor William G. Pace III Professor of Cancer Research Cancer Scholar and Senior Advisor, Ohio State University Comprehensive Cancer Center and James Cancer Hospital and Solove Research Institute Education &Academic Appointments: 1968 M.D. U Chicago; 1973-80, Assistant, Associate Prof. of Medicine, U Minnesota (U. MN), Minneapolis, MN; 1980-89 Prof. of Medicine, Div. of Oncology, U.MN; 1989-97 Prof. of Medicine & Chief, Div. of Oncology, State University of NY at Buffalo; 1989-97 Chair, Department of Medicine, Roswell Park Cancer Institute (RPCI), Buffalo, NY; 1997-2001 Director, Div. of Hematology & Oncology, Department of Internal Medicine, The Ohio State University College of Medicine & Public Health (OSU COMPH), Columbus, OH; 1997- William G. Pace III Endowed Chair in Cancer Research & Prof, OSU; 1997-2003 Director, Comprehensive Cancer Center (CCC) & Deputy Director, James Cancer Hospital & Solove Research Institute (JCH), OSU; 2003- Cancer Scholar & Senior Advisor, OSUCCC & JCH; 2006- Distinguished University Prof. -

John Burchenal Oral History Interview
Joseph Burchenal Interview, January 26, 2001 1 National Cancer Institute Oral History Interview Project Interview with Joseph Burchenal Conducted on January 26, 2001 by Peggy Dillon Darien, Connecticut PD: Good morning. This is Peggy Dillon of History Associates Incorporated. I am speaking with Dr. Joseph Burchenal for the NCI oral history interview series. We are at his home in Darien, Connecticut. Today is January 26, 2001. JB: Good morning. PD: I would like to talk with you today about your work in cancer chemotherapy in general and also your involvement with the National Cancer Institute in particular. Before we get into your career overall and NCI, I'd like to ask you about your background. If you could just tell me a little bit about your upbringing and education . I understand that you were interested in chemistry from a very early age. JB: I was born in Milford, Delaware, but I lived in Wilmington, Delaware, for the first part of my life. My mother died when I was three, in childbirth. So I lived with my father in Wilmington. He was a lawyer. I went to school at Tower Hill School. The majority of my friends in the school had fathers or mothers–fathers mainly–who worked for Dupont. They were very likely to, so that there was a lot of interest in chemistry there. In fact, it was the same way on the street where we lived, where the fathers were mostly chemists. But my interest in chemistry, I guess, started when I was eight years old and I had a cousin who was eleven who was given a Chemcraft set and he used to show us all of the interesting things that he could do with it. -

Physiologist President Earl H
THE AMERICAN PHYSIOLOGICAL SOCIETY Founded in 1887 for the purpose of promoting the increase of The physiological knowledge and its utilization. OFFICERS Physiologist President Earl H. Wood, Mayo Med. Sch., Rochester, MN President-Elect Francis J . Haddy, Uniformed Services Univ. of Hlth. Sci., Volume 24, No. 2, April 1981 Bethesda, MD Past President TABLE OF CONTENTS Ernst Knobil, Univ. of Pittsburgh HISTORICAL ARTICLES Council George H. Whipple --- Horace W. Davenport. Earl H. Wood, Francis J. Haddy, Ernst Knobil, Jack L. Kostyo, Centennial Celebration 5 S. McD. McCann, Paul C. Johnson, Leon Farhi SOCIETY AFFAIRS Executive Secretary-Treasurer Notes from Capitol Hill. 6 Orr E. Reynolds, 9650 Rockville Pike, Bethesda, Maryland Legislation and Animal Experimentation ... Earl Wood and Helene Cecil. 7 20014 Invitation to Membership in the NSMR. 9 SUSTAINING MEMBERS Frontiers in the Teaching of Physiology . 10 Abbott Laboratories Merrell Res. Ctr., Div. of APS Sections: How to Become Affiliated . ... 11 Burroughs Wellcome Co. Richardson-Merrell Inc. Member Contributions. 11 CIBA Geigy Corp. Pfizer, Inc. International Satellite Symposium. 12 Grass Instrument Co. Revlon Health Care Group Clearance Sale 18 Hoechst-Roussel Pharmaceu- A.H. Robins Co., Inc. Travel Awards and Application ... 19 tical Co., Inc. Sandoz, Inc. Membership Instructions and Application 21 Hoffmann-La Roche, Inc. G. D. Searle & Co. CAS Brief . 25 ICI Americas lnc. Smith Kline & French Labs. ANNOUNCEMENTS International Minerals & I.A. Squibb & Sons, Inc. Future Meetings. II Chemical Corp. The Upjohn Co. Symposium: Basic Biology of Muscles .. 5 Eli Lilly and Co. Waverly Press MIT Summer Course . 5 McNeil Laboratories Wyeth Laboratories, Inc. Fulbright Appointments 1981-83 10 Merck Sharp & Dohme Symposium on Respiratory System. -

Balcomk41251.Pdf (558.9Kb)
Copyright by Karen Suzanne Balcom 2005 The Dissertation Committee for Karen Suzanne Balcom Certifies that this is the approved version of the following dissertation: Discovery and Information Use Patterns of Nobel Laureates in Physiology or Medicine Committee: E. Glynn Harmon, Supervisor Julie Hallmark Billie Grace Herring James D. Legler Brooke E. Sheldon Discovery and Information Use Patterns of Nobel Laureates in Physiology or Medicine by Karen Suzanne Balcom, B.A., M.L.S. Dissertation Presented to the Faculty of the Graduate School of The University of Texas at Austin in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy The University of Texas at Austin August, 2005 Dedication I dedicate this dissertation to my first teachers: my father, George Sheldon Balcom, who passed away before this task was begun, and to my mother, Marian Dyer Balcom, who passed away before it was completed. I also dedicate it to my dissertation committee members: Drs. Billie Grace Herring, Brooke Sheldon, Julie Hallmark and to my supervisor, Dr. Glynn Harmon. They were all teachers, mentors, and friends who lifted me up when I was down. Acknowledgements I would first like to thank my committee: Julie Hallmark, Billie Grace Herring, Jim Legler, M.D., Brooke E. Sheldon, and Glynn Harmon for their encouragement, patience and support during the nine years that this investigation was a work in progress. I could not have had a better committee. They are my enduring friends and I hope I prove worthy of the faith they have always showed in me. I am grateful to Dr. -

Government of Andhra Pradesh Note on Demand No. Xviii Education Department of Education
GOVERNMENT OF ANDHRA PRADESH NOTE ON DEMAND NO. XVIII EDUCATION 1996-97 DEPARTMENT OF EDUCATION NOTE ON DEMAND NO- XVIII EDUCATION 1996 - 97 SUBMITTED TO THE BUDGET SESSION ANDHRA PRADESH LEGISLATURE NIEPA DC D10831 By B. DURGAPRASAD RAO Minister for School Education Public Libraries and Archaeology & Museums D-1 AlWtMiy & B8CUMW r ATHM GEVru -National lactitate of PiMUiiQg ead A4mi&iitrftCi«t. Sri /teKdVin<do Maxf, n^L--™ JIE3E2s»D D -lx CONTENTS S/JVb. Name o f the Department Page No. 1. School Education 1 2. Jawahar Bal Bhavan 34 3. Public Libraries 40 4. A. P. Govt. Text Book Press 44 5. Registrar of Publications 45 6. Adult Education 47 7. Intermediate Education 51 8. Collegiate Education 53 9. A. P. State Council of Higher Education 59 10. Archaeology and Museums 63 11. Oriental Manuscripts Library and Research Institute 66 12. State Archives and Research Institute 67 13. National Cadet Corps 72 14. Sports Authority 74 15. Sports School 75 16. Cultural Affairs 76 17. Youth Welfare 78 18. Academies .... 80 - 88 19. Educational Statistics and Charts .... 1 - 8 111 Speaker Sir, I seek the permission of the Chair to move this composite demand for Rs. 2039,78,23,000/- which covers General Education, Sports, Art and Culture. The Directive Principle of State Policy imder Article 45 of the Indian Constitution adopted on 26th January, 1950, enjoined upon the State to pro vide free and Compulsory Elementary Education to all children upto the a^e of 14 By 1960. During the past five decades, there has Been a phenominal expansion of Elementary Education as a result of which 98% of the niral population in the State have schools within a Walking distance of 1 Km. -
Book Review Paul Janssen
BOOK REVIEW PAUL JANSSEN: PIONEER IN PHARMA & IN CHINA By Geerdt Magiels, Dundee: Dundee University Press, 2008, 258 pp. (incl. appendices and bibliography), £15.00, ISBN 978-1-84586-53-0 The history of Janssen Pharmaceutica and its evolvement in China is central to this homage to Paul Janssen, who set up the company in 1953; led it through a merger with Johnson & Johnson in 1961; built up relations with China from the 1960s onwards; and left clear footprints on its research agenda and company management style. The book owes its existence to Paul Janssen, who commissioned it to the author Geerdt Magiels. However, Janssen died shortly after their first meeting in 2003. The book aims to make known the scientific, business and human achievements of Paul Janssen. As such, there are scatterings of descriptions of major events in Janssen’s life; group photographs of important occasions and celebrations; and advice and adages on how to collaborate (for example, to have an open mind; to be creative; to allow local people to run the business; to work through friendship and compromise; to have patience; and to show mutual respect). The book gives corporate meaning to a global audience of the role of large pharmaceutical companies in developing countries. A role that involves the efforts made by such companies to advertise themselves as a bridge between rich and poor; their motivation by concerns for global health; and contributors to the well-being and development of people in developing countries. As a eulogy, this book can hardly be expected to meet academic standards. -
Front Matter (PDF)
CancerResearch AN OFFICIAL JOURNAL OF THE AMERICAN ASSOCIATION FOR CANCER RESEARCH July 1, 1996 Volume 56 •¿Number 13 PP. 2881-3163 ISSN 0008-5472 •¿CNREA 8 The Definitive Reference for Your Lab and Library >^~^ Encyclopedia of CancerEditor-in-Chief JOSEPH R. BERTINO Sloan-Kettering Institute for Cancer Research. Memorial Sloan-Kettering Cancer Center, New York. New York, and Past President of the American Association for Cancer Research From the Prepublication Reviews PraisefortheArticle"AtaxiaTelangiectasiaSyndrome" PraisefortheArticle"Hypertnermia" TOPICSCOVERED "Covers every aspect of the disease from its clinical "The manuscript is well written by two authors very features to its underlying cellular and molecular knowledgeable in the subject, and the materia/ covered mechanisms in a concise and well-organized is broad enough and in depth enough for the purpose •¿Antisense,Ribosomes stated in the publishers descriptor." fashion...The material presented was complete and up-to-date." •¿BiologyofCancer —¿MICHAELBORRELLI,William Beaumont Hospital —¿MICHAEL B.KASTAN. Johns Hopkins Hospital Royal Oak. Michigan Johns Hopkins University. Baltimore. Maryland PraisefortheArticle"RadiotherapyandConcomitantChemotherapy" Praise for the Article "Interactions Between Drugs and Regulators "This is a comprehensive review of the subject, dealing in the Treatment of Leukemia" with rationale, toxicity, and applications of combined "Excellent review and discussion by the author of an chemoradiotherapy. The coverage of various tumor types Chemotherapy important area." is particularly broad and well organized." GeneTherapy —¿ERICJ. FELDMAN. New York Medical College. Valhalla —¿PHILIPC. HOFFMAN. University of Chicago Medical Center, Illinois Praise for the Article "Differentiation & Cancer" Oncogenes "This is a clearly written article." Praisefor theArticle"RASGeneAlterationsin HumanLungCancer" "Excellent/" —¿GARYS.STEIN.