Vermont Nurse Connection
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

How to Convert Desktop Apps to Universal Windows Platform Apps with Desktop Bridge
How to convert desktop apps to Universal Windows Platform apps with Desktop Bridge If you're looking to bring your traditional app to the Universal Windows Platform, this guide walks you through the steps to use the DesktopAppConverter to convert your app. On Windows 10, Microsoft is not only adding new features and making the operating system more secure, but it's also investing on making the Windows Store the single place for users to acquire apps. The caveat with the Windows Store is that it doesn't include support for distribution of traditional desktop applications -- you're only able to download Universal Windows Platform (UWP) apps. However, Microsoft is making some changes, and now thanks to Desktop Bridge, we're slowly starting to see desktop apps and tools available in the Store. What's Desktop Bridge? How does Desktop Bridge works? Things you need before converting an app How to prepare your computer to convert apps How to convert desktop apps into Windows Store apps How to install a converted app on Windows 10 What's Desktop Bridge? It's all part of an initiative called Project Centennial, which now you know as Desktop Bridge. The new approach is essentially a "bridge" that let developers take traditional desktop applications and convert them into Universal Windows Platform (modern) apps. The idea behind Desktop Bridge is that great apps take time and effort, and if they're already working, Microsoft doesn't want you to abandon that code. With Desktop Bridge, you can take your existing desktop application (Win32, WPF, and Windows Forms), make a little modification (if necessary), and bring that great code to the new platform, which can also take advantage of many new features. -

Windows 10 to Stop Asking You for Feedback 2
Table of Contents SYSTEM o Display o Advance Display Settings o Color calibration o ClearType text o Advanced sizing of text and other items o Display adapter properterties o Notification & actions o Select which icons appear on the taskbar o Turn system icons on or off o Apps & Features o Manage optional features o See optional feature history o Programs And Features o Multitasking o Tablet Mode o Battery Saver o Battery Use o Change Background App Settings o Change Battery Saver Settings o Battery Saver Settings o Power & Sleep o Additional power settings o Storage o Offline Maps o Choose default apps o Choose Defaults Apps By File Type o Choose Defaults Apps By Protocol o Set Defaults By App o About o Change product key or upgrade your edition of Windows o Read the Privacy Statement for Windows and Microsoft services o Read the Microsoft Services Agreement that applies to our services o Read the Microsoft Software License Terms o Additional Administrative Tools o Bitlocker settings o DeviceManager 1 | Page o System info DEVICES o Printers & Scanners o Devices & Printers o DeviceManager o Connected devices o Mouse And Touchpad o Additional Mouse Options o Typing o Pen o AutoPlay o Default app settings o USB Network & Internet o WiFi o WirelessNetworkConnection o Advanced options o Manage Wi-Fi Settings o Your email and accounts o Sign in with a Microsoft account instead o Add a work or school account o Change adapter options o Change Advanced Sharing Options o Network and Sharing Center o HomeGroup o Windows Firewall o Airplane mode -

Quick Guide Page | 1
Quick Guide Page | 1 Contents Welcome to Windows 10 ................................................................................................................................................................................................... 3 Key innovations ...................................................................................................................................................................................................................... 3 Cortana ................................................................................................................................................................................................................................. 3 Microsoft Edge .................................................................................................................................................................................................................. 4 Gaming & Xbox ................................................................................................................................................................................................................ 5 Built-in apps ....................................................................................................................................................................................................................... 7 Enterprise-grade secure and fast ................................................................................................................................................................................... -
Shortcut Keys for Windows 10
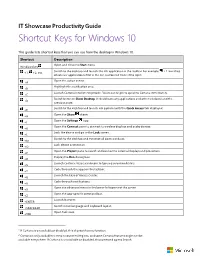
IT Showcase Productivity Guide Shortcut Keys for Windows 10 This guide lists shortcut keys that you can use from the desktop in Windows 10. Shortcut Description Open and close the Start menu. Windows key Switch to the desktop and launch the nth application in the taskbar. For example, +1 launches +1, +2, etc. whichever application is first in the list, numbered from left to right. Open the action center. +A Highlight the notification area. +B Launch Cortana into listening mode.1 Users can begin to speak to Cortana immediately. +C Switch between Show Desktop (hides/shows any applications and other windows) and the +D previous state. Switch to the desktop and launch File Explorer with the Quick Access tab displayed. +E Open the Share charm. +H Open the Settings app. +I Open the Connect pane to connect to wireless displays and audio devices. +K Lock the device and go to the Lock screen. +L Switch to the desktop and minimize all open windows. +M Lock device orientation. +O Open the Project pane to search and connect to external displays and projectors. +P Display the Run dialog box. +R Launch Cortana.2 Users can begin to type a query immediately. +S Cycle through the apps on the taskbar. +T Launch the Ease of Access Center. +U Cycle through notifications. +V Open the advanced menu in the lower-left corner of the screen. +X Open the app-specific command bar. +Z Launch Narrator. +ENTER Switch input language and keyboard layout. +SPACEBAR Open Task view. +TAB 1 If Cortana is unavailable or disabled, this shortcut has no function. -
Windows 10 Open the Start Menu This Pamphlet Online Windows 10 - Press Start Button Or the Icon Resize App Tile on the Start Menu
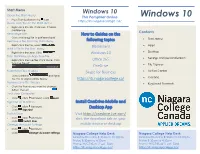
Start Menu Windows 10 Open the Start Menu This Pamphlet Online Windows 10 - Press Start button or the icon https://its.niagaracollege.ca/ Resize App Tile on the Start Menu - Right click the Tile, Click size, Choose preference Contents Rearrange Tiles How to Guides on the - Click and drag tile to preferred spot following topics Start Menu Remove a Tile from the Start Menu - Right click the tile, select Blackboard Apps Add a Tile to the Start Menu Desktop - Right click the app, Click Windows 10 Stop Updating on Apps Live Tile Settings and personalization - Right click the live Tile, Click More, Click Office 365 Turn live tile off File Explorer OneDrive Search for Files or Apps Action Center Skype for Business - Click Cortana and type Cortana the File or Applications Name https://its.niagaracollege.ca/ Rename Live Tile Groups Keyboard Shortcuts - Click the Name you want to change. Adjust the text Lock your Computer - Click , click Account, Click Lock Sign Out of Windows Install OneDrive Mobile and - Click , click Account, Desktop App Click Sign Out Switch Users Visit https://onedrive.live.com/ - Click , click Account, click the download tab on your Click Switch User Change Account Settings mobile device or desktop - Click , click Account, Click Change Account Settings Niagara College Help Desk Niagara College Help Desk Monday-Thursday 8:30am to 10:00pm Monday-Thursday 8:30am to 10:00pm Friday 8:30am to 4:30pm Friday 8:30am to 4:30pm Phone: 905-735-2211 ext. 7642 Phone: 905-735-2211 ext. 7642 https://its.niagaracollege.ca/ https://its.niagaracollege.ca/ -
Students, Faculty and Staff Guide for Windows 10
Students, Faculty and Staff Guide for Windows 10 Prepared by Information Technology Division Lehman College, CUNY Revised - January 31, 2020 This document was originally prepared by Microsoft. It was modified and adapted for use at Lehman College. Information Technology Division Lehman College, CUNY Guide contents The purpose of this guide is to introduce you to the key features in Windows 10, and give you tips and tricks on how to get started using those features. You’ll find information on the following topics: A few feature highlights Cortana Using Microsoft Office Personalization • Start menu • What can Cortana do? 365 with Windows 10 and Settings • Access your email • A new look • How to search • Cortana’s Notebook • Use Office 365 on • Personalize your lock • Using tiles Microsoft Edge mobile devices screen • Task view • Hub • Use Office 365 with • Get started with themes • Virtual desktops OneDrive for Business to • Web Notes • Change your desktop work with files anywhere • Windows behavior in • Reading List background and color modern applications • Sign in to Office 365 Apps and the • Charms functionality in Setting things up • Create a file action center modern applications • Set up your email and • Share a file calendar • Snap enhancements • Synchronize a file • Change your • Quick access tools account picture • Protect your PC Information Technology Division Lehman College, CUNY A few feature highlights in Windows 10 Windows 10 is designed to please both touch and mouse users. It’s also designed to be intuitive for users of both Windows 7 and Windows 8.1, incorporating the “best of both worlds” to enhance your experience and help you be more productive. -

Windows 10 Quick Reference Card
Microsoft® Windows 10 Quick Reference Card Windows Desktop and Start Menu Keyboard Shortcuts General App List Tile Group App Tile Start menu ........................... 0 Copy a file or folder .............. Ctrl + C Cut a file or folder ................. Ctrl + X Paste a file or folder .............. Ctrl + V Action Center ....................... + A Task view ............................. + Tab Close an app ........................ Alt + F4 Lock computer ..................... + L Print ..................................... Ctrl + P Start Menu File Explorer ......................... + E Account Run dialog box ..................... + R Document Ease of Access Center. ........ + U Picturess Task Manager ...................... Ctrl + Shift Settings Esc Power Capture screenshot .............. + PrtScn Show Open Search ........................ + S Desktop Open Narrator ...................... + Enter Start Search Task Pinned Taskbar System Button Field View Apps Icons Settings Shortcuts Windows settings ................. + I Start Menu Apps Connect pane ...................... + K Open the Start Menu: Click the Start button Launch an App: Click the app’s tile in the Start Sharing pane ........................ + H on the taskbar, or, press the key. menu. Or, scroll through the list of apps at the left Display options for of the Start Menu and select the app you want to second screen ..................... + P Resize an App Tile in the Start Menu: Right- open. click a tile, select Resize, and select a size. Quick Link menu .................. + X Search for an App: Click within the Search field Rearrange Tiles: Click and drag a tile to a new and type a keyword for the app you want to Desktop Shortcuts location in a group. Or, drag a tile between open. groups to start a new group. Show/hide desktop .............. + D Jump to an Open App: Click the Task View Maximize window ................ -
Getting to Know Windows 10 for Employees
Getting to know Windows 10 for employees Microsoft IT Showcase microsoft.com/itshowcase Familiar and better than ever Windows 10 is the best combination of the Windows you Windows 10 was designed to be the safest Windows already know, plus lots of great improvements you’ll love. ever. The Creators Update adds comprehensive security It helps you do what matters, faster. capabilities and privacy tools on top of what was already available in Windows 10. Our new Creators Update is designed to spark and The new Surface devices for Windows 10 are a balance unleash creativity, bringing 3D and mixed reality to of craftsmanship, performance, and versatility, designed everyone. Combined with Office 365, Cortana, and with you at the center. Microsoft Edge, you’ll have new ways of working that increase and enhance your productivity. And the IT management tools, services, and advances like AutoPilot and Microsoft Store for Business will make the work of IT organizations easier and more systematic. Microsoft IT Showcase microsoft.com/itshowcase Getting to know Windows 10 Creators Update Boost productivity • Start menu • Task view • Edge • Quick access menu • Virtual desktop • Office365 • Using tiles • Personalization • Windows Ink • Snap enhancements • Action center and notifications • Paint 3D • Tablet mode • Cortana Comprehensive security Devices and Windows 10 S Modern IT • Windows Hello • Meet the Surface family • AutoPilot • Windows Defender features • Windows 10 S • Microsoft Store for Business • Microsoft Edge • Security Guards • Windows Information Protection Microsoft IT Showcase microsoft.com/itshowcase The Start menu: More options, easy access Windows 10 brings back the familiar Windows desktop and Start menu from Windows 7. -

Quick Start Guide to Windows 10 Making Your Move to Windows 10 Quick and Simple Table of Contents
Quick Start Guide to Windows 10 Making your move to Windows 10 quick and simple Table of Contents Understanding your desktop Security, privacy and scam protection Take a tour of the Windows 10 desktop. Learn how to be more Your security and privacy mean a lot to us. Windows 10 features a productive using the Windows Start menu, Taskbar and Action full security dashboard, with personal privacy settings and our most center. advanced safety measures yet. Setup and personalization Accessibility Make it yours! Windows 10 is all about you, from personalized Microsoft’s accessibility features make tasks easier for users with a backgrounds to custom language choices. Create a Microsoft disability. Enlarge screen text to make it easier to read and change account to unlock the full Microsoft universe of features. narration and dictation settings. Apps and programs Windows updates and upgrades Now that you’ve made yourself at home, it’s time to take Windows 10 provides regular updates to keep your device Windows 10 to the next level: adding apps. Whether you want secure and bring new features to you. Windows 7 users can find to tackle more tasks around the house or at work, or have fun resources to transition to Windows 10. playing games, it’s all here. Tips and tricks Additional resources Do more with Windows 10! Our tips and tricks will get you off and We’re here to help you make the most of Windows 10 from Day running in no time. 1 to Day 101—and beyond! Get to know these resources. -

Windows 10 for Beginners
Windows 10 for beginners Windows 10 is the latest version of the Windows operating system. New PCs will typically come with Windows 10 installed. If you have an older computer and would like to purchase Windows 10, it starts at $119. Find out more at: https://www.microsoft.com/en-us/windows/get- windows-10 Signing in There are two ways to sign in to your Windows 10 computer: with a local account or a Microsoft account. A local account means all of your files and settings are only accessible on the computer you log into. (Just like usual, to many of us!) A Microsoft account (Outlook, Hotmail, Live, MSN) allows you to sync your information between multiple devices, and would even let you sign into your account from a friend’s Windows 10 device. You need a Microsoft account to use features like Cortana, download from the Windows Store, and activate Find My Device. If you don’t have a Microsoft account, Windows 10 will walk you through setting one up. You can switch between a local and Microsoft account at any time. Windows 10 desktop screen Icons and shortcuts Start menu Cortana Task View Edge File Explorer Store Internet signal Sound Action Center La Crosse Public Library Windows 10 for beginners p.1 Start menu Microsoft now calls most things “apps”. Click on the Windows logo in the lower left corner to open your Start menu and see your apps. Get to your most These are called tiles. If they are used apps. If you’re animated, they’re called live tiles. -

Windows 10 Quick Reference Guide Free Cheat Sheets Visit Ref.Customguide.Com
Microsoft® Windows 10 Quick Reference Guide Free Cheat Sheets Visit ref.customguide.com Windows Desktop and Start Menu Keyboard Shortcuts General App List Tile Group App Tile Start menu .......................... 0 Copy a file or folder .............. Ctrl + C Cut a file or folder ................ Ctrl + X Paste a file or folder ............. Ctrl + V Action Center ...................... + A Task view ............................ + Tab Close an app ....................... Alt + F4 Lock computer .................... + L Print .................................... Ctrl + P Start Menu File Explorer ........................ + E Account Run dialog box ..................... + R Documents Ease of Access Center. ........ + U Pictures Task Manager ..................... Ctrl + Shift Settings Esc Power Capture screenshot ............. + PrtScn Show Open Search ....................... + S Desktop Open Narrator ..................... + Enter Start Search Task Pinned Taskbar System Button Field View Apps Icons Settings Shortcuts Windows settings ................. + I Start Menu Apps & Taskbar Connect pane ...................... + K Open the Start Menu: Click the Start button on Launch an App: Click the app’s tile in the Start Sharing pane ....................... + H the taskbar, or, press the key. menu. Or, scroll through the list of apps at the left Display options for of the Start menu and select the app you want to second screen ..................... + P Resize an App Tile in the Start Menu: Right-click a open. tile, select Resize, and select a size. Quick Link menu .................. + X Install an App: Click the Microsoft Store icon on Rearrange Tiles: Click and drag a tile to a new the taskbar. Browse or search for the app you Desktop Shortcuts location in a group. Or, drag a tile between groups want and click it. Click Get to install a free app or to start a new group. -

Windows 10: Part 1
Windows 10: Part 1 Updated: May 2018 Price: $2.00 A Special Note on Terminology Windows 10 accepts both mouse and touch commands. This means that you could use either mouse clicks or touch gestures interchangeably. Throughout this document, you will read either click, tap, or click/tap. Please note that you can click on anything that says “tap,” and you can tap on anything that says “click.” Click = Tap Double Click = Double Tap Click and Drag = Tap and Drag Right Click = Tap and Hold NOTE: You must have a touchscreen to use touch commands. What is Windows 10? Windows 10 is Microsoft’s latest operating system for home and work computers. An operating system (OS) is a collection of software that enables the user to interact with the computer. Currently, Windows is still the most popular OS on the market for personal or home computers. The Microsoft Account Before we go further, let’s talk about the Microsoft Account. When you first upgrade to Windows 10, or purchase a computer with Windows 10, you will have the opportunity to create a Microsoft ID. NOTE: You do not have to create an ID, but some features require you to create an account. A Microsoft ID allows you to access Internet-connected apps, the Microsoft Store, and Cortana. If these terms are new to you—don’t worry!—we will explain them later. For now, know that as you get more used to the computer, you may need to create a Microsoft account to use additional features in Windows. Lesson 1: Touring Windows 10 The Desktop After you start your computer and sign into Windows, you will see the desktop.