World Bank ‐ Third Party Monitoring Service Progress Report Contract
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dethoma, Melut County, Upper Nile State 31 January 2014
IRNA Report: Dethoma, Melut, 31 January 2014 Initial Rapid Needs Assessment: Dethoma, Melut County, Upper Nile State 31 January 2014 This IRNA Report is a product of Inter-Agency Assessment mission conducted and information compiled based on the inputs provided by partners on the ground including; government authorities, affected communities/IDPs and agencies. 0 IRNA Report: Dethoma, Melut, 31 January 2014 Situation Overview: An ad-hoc IDP camp has been established by the Melut County Commissioner at Dethoma in order to accommodate Dinka IDPs who have fled from Baliet county. Reports of up to 45,000 based in Paloich were initially received by OCHA from RRC and UNMISS staff based in Melut but then subsequent information was received that they had moved to Dethoma. An IRNA mission from Malakal was conducted on 31 January 2014. Due to delays in the deployment by helicopter, the RRC Coordinator was unable to meet the team but we were able to speak to the Deputy Paramount Chief, Chief and a ROSS NGO at the site. The local NGO (Woman Empowerment for Cooperation and Development) had said they had conducted a preliminary registration that showed the presence of 3,075 households. The community leaders said that the camp contained approximately 26,000 individuals. The IRNA team could only visually estimate 5 – 6000 potentially displaced however some may have been absent at the river. The camp is situated on an open field provided and cleared by the Melut County Commissioner, with a river approximately 300metres to the south. There is no cover and as most IDPs had walked to this location, they had carried very minimal NFIs or food. -
Project Proposal
Project Proposal Organization GOAL (GOAL) Project Title Provision of treatment to children aged 659 months and pregnant and lactating women diagnosed with moderate acute malnutrition (MAM) or severe acute malnutrition (SAM) for children aged 659 month and pregnant and lactating women in Melut County, Upper Nile State Fund Code SSD15/HSS10/SA2/N/INGO/526 Cluster Primary cluster Sub cluster NUTRITION None Project Allocation 2nd Round Standard Allocation Allocation Category Type Frontline services Project budget in US$ 150,000.01 Planned project duration 5 months Planned Start Date 01/08/2015 Planned End Date 31/12/2015 OPS Details OPS Code SSD15/H/73049/R OPS Budget 0.00 OPS Project Ranking OPS Gender Marker Project Summary Under the proposed intervention, GOAL will provide curative responses to severe acute malnutrition (SAM) and moderate acute malnutrition (MAM) through the provision of outpatient therapeutic programmes (OTPs) and targeted supplementary feeding programmes (TSFPs) for children 659 months and pregnant and lactating women (PLW). The intervention will be targeted to Melut County, Upper Nile State – which has been heavily affected by the ongoing conflict. This includes continuing operations in Dethoma II IDP camp as well as expanding services to the displaced populations in Kor Adar (one facility) and Paloich (two facilities). GOAL also proposes to fill the nutrition service gap in Melut Protection of Civilians (PoC) camp. In the PoC, GOAL will be providing static services, with complementary primary health care and nutrition programming. In the same locations, GOAL will conduct mass outreach and mid upper arm circumference (MUAC) screening campaigns within communities, IDP camps, and the PoC with children aged 659 months and pregnant and lactating women (PLW) in order to increase facility referrals. -

1 AU Commission of Inquiry on South Sudan Addis Ababa, Ethiopia P. O
AU Commission of Inquiry on South Sudan Addis Ababa, Ethiopia P. O. Box 3243 Telephone: +251 11 551 7700 / +251 11 518 25 58/ Ext 2558 Website: http://www.au.int/en/auciss Original: English FINAL REPORT OF THE AFRICAN UNION COMMISSION OF INQUIRY ON SOUTH SUDAN ADDIS ABABA 15 OCTOBER 2014 1 Table of Contents ACKNOWLEDGEMENTS ............................................................................................... 3 ABBREVIATIONS ........................................................................................................... 5 CHAPTER I ..................................................................................................................... 7 INTRODUCTION ............................................................................................................. 8 CHAPTER II .................................................................................................................. 34 INSTITUTIONS IN SOUTH SUDAN .............................................................................. 34 CHAPTER III ............................................................................................................... 110 EXAMINATION OF HUMAN RIGHTS VIOLATIONS AND OTHER ABUSES DURING THE CONFLICT: ACCOUNTABILITY ......................................................................... 111 CHAPTER IV ............................................................................................................... 233 ISSUES ON HEALING AND RECONCILIATION ....................................................... -

Resident Coordinator Support Office, Upper Nile State Briefing Pack
Resident Coordinator Support Office, Upper Nile State Briefing Pack Table of Contents Page No. Table of Contents 1 State Map 2 Overview 3 Security and Political History 3 Major Conflicts 4 State Government Structure 6 Recovery and Development 7 State Resident Coordinator’s Support Office 8 Organizations Operating in the State 9-11 1 Map of Upper Nile State 2 Overview The state of Upper Nile has an area of 77,773 km2 and an estimated population of 964,353 (2009 population census). With Malakal as its capital, the state has 13 counties with Akoka being the most recent. Upper Nile shares borders with Southern Kordofan and Unity in the west, Ethiopia and Blue Nile in the east, Jonglei in the south, and White Nile in the north. The state has four main tribes: Shilluk (mainly in Panyikang, Fashoda and Manyo Counties), Dinka (dominant in Baliet, Akoka, Melut and Renk Counties), Jikany Nuer (in Nasir and Ulang Counties), Gajaak Nuer (in Longochuk and Maiwut), Berta (in Maban County), Burun (in Maban and Longochok Counties), Dajo in Longochuk County and Mabani in Maban County. Security and Political History Since inception of the 2005 Comprehensive Peace Agreement (CPA), Upper Nile State has witnessed a challenging security and political environment, due to the fact that it was the only state in Southern Sudan that had a Governor from the National Congress Party (NCP). (The CPA called for at least one state in Southern Sudan to be given to the NCP.) There were basically three reasons why Upper Nile was selected amongst all the 10 states to accommodate the NCP’s slot in the CPA arrangements. -

Upper Nile State SOUTH SUDAN
COMMUNITY CONSULTATION REPORT Upper Nile State SOUTH SUDAN Bureau for Community Security South Sudan Peace and Small Arms Control and Reconciliation Commission United Nations Development Programme Ministry of Foreign Affairs of the Netherlands The Bureau for Community Security and Small Arms Control under the Ministry of Interior is the Gov- ernment agency of South Sudan mandated to address the threats posed by the proliferation of small arms and community insecurity to peace and development. The South Sudan Peace and Reconciliation Commission is mandated to promote peaceful co-existence amongst the people of South Sudan and advises the Government on matters related to peace. The United Nations Development Programme in South Sudan, through the Community Security and Arms Control Project, supports the Bureau strengthen its capacity in the area of community security and arms control at the national, state and county levels. The consultation process was led by the Government of South Sudan, with support from the Govern- ment of the Netherlands’ Ministry of Foreign Affairs. Cover photo: A senior chief from Upper Nile. © UNDP/Sun-ra Lambert Baj COMMUNITY CONSULTATION REPORT Upper Nile State South Sudan Published by South Sudan Bureau for Community Security and Small Arms Control South Sudan Peace and Reconciliation Commission United Nations Development Programme MAY 2012 JUBA, SOUTH SUDAN CONTENTS Acronyms ........................................................................................................................... i Foreword .......................................................................................................................... -

The Conflict in Upper Nile State (18 March 2014 Update)
The Conflict in Upper Nile State (18 March 2014 update) Three months have elapsed since widespread conflict broke out in South Sudan, and Malakal, Upper Nile’s state capital, remains deserted and largely burned to the ground. The state is patchwork of zones of control, with the rebels holding the largely Nuer south (Longochuk, Maiwut, Nasir, and Ulang counties), and the government retaining the north (Renk), east (Maban and Melut), and the crucial areas around Upper Nile’s oil fields. The rest of the state is contested. The conflict in Upper Nile began as one between different factions within the SPLA but has now broadened to include the targeted ethnic killing of civilians by both sides. With the status of negotiations in Addis Ababa unclear, and the rebel’s 14 March decision to refuse a regional peacekeeping force, conflict in the state shows no sign of ending in the near future. With the first of the seasonal rains now beginning, humanitarian costs of ongoing conflict are likely to be substantial. Conflict began in Upper Nile on 24 December 2013, after a largely Nuer contingent of the Sudan People’s Liberation Army’s (SPLA) 7th division, under the command of General Gathoth Gatkuoth, declared their loyalty to former vice-president Riek Machar and clashed with government troops in Malakal. Fighting continued for three days. The central market was looted and shops set on fire. Clashes also occurred in Tunja (Panyikang county), Wanding (Nasir county), Ulang (Ulang county), and Kokpiet (Baliet county), as the SPLA’s 7th division fragmented, largely along ethnic lines, and clashed among themselves, and with armed civilians. -

South Sudan 2015 Human Rights Report
SOUTH SUDAN 2015 HUMAN RIGHTS REPORT EXECUTIVE SUMMARY South Sudan is a republic operating under a transitional constitution signed into law upon declaration of independence from Sudan in 2011. President Salva Kiir Mayardit, whose authority derives from his 2010 election as president of what was then the semiautonomous region of Southern Sudan within the Republic of Sudan, led the country. While the 2010 Sudan-wide elections did not wholly meet international standards, international observers believed Kiir’s election reflected the will of a large majority of Southern Sudanese. International observers considered the 2011 referendum on South Sudanese self-determination, in which 98 percent of voters chose to separate from Sudan, to be free and fair. President Kiir is a founding member of the Sudan People’s Liberation Movement (SPLM) political party, the political wing of the Sudan People’s Liberation Army (SPLA). Of the 27 ministries, only 21 had appointed ministers in charge, of which 19 are SPLM representatives. The bicameral legislature consists of 332 seats in the National Legislative Assembly (NLA), of which 296 were filled, and 50 seats in the Council of States. SPLM representatives controlled the vast majority of seats in the legislature. Through presidential decrees Kiir replaced eight of the 10 state governors elected since 2010. The constitution states that an election must be held within 60 days if an elected governor has been relieved by presidential decree. This has not happened. The legislature lacked independence, and the ruling party dominated it. Civilian authorities failed at times to maintain effective control over the security forces. In 2013 armed conflict between government and opposition forces began after violence erupted within the Presidential Guard Force (PG) of the SPLA, also known as the Tiger Division. -

1.1 Million 3.2 Million 4.9 Million
South Sudan Crisis Situation report as of 10 April 2014 Report number 31 This report is produced by OCHA South Sudan in collaboration with humanitarian partners. It covers the period from 4 to 10 April 2014. The next report will be published on or around 18 April 2014. Highlights Clashes were reported in northern Upper Nile State, with tension mounting in and around Melut. So far, aid agencies have reached around 1.1 million people, around one third of the people to be assisted by June. Over 960,000 people have been reached with medical interventions. Over 100,000 people are reported to be displaced in and around Kodok, Lul and Wau Shiluk in Upper Nile State. They are in urgent need of assistance. Multi-sector rapid response was ongoing in eight locations in Jonglei, Unity and Upper Nile states, with partners also ready to begin response in Kodok, Upper Nile State. 4.9 million 3.2 million 1.1 million 817,700 People in need of People to be assisted People reached with People internally humanitarian by aid organizations by humanitarian displaced by violence assistance June assistance* since 15 Dec 2013 *This includes people internally displaced, refugees from other countries sheltering in South Sudan and other vulnerable communities who have received assistance since January 2014. This does not mean that the needs of these people have been comprehensively met. Situation overview Clashes were reported in Upper Nile State the Central Equatoria Jonglei 250,000 last days, including in Kaka, 40 kilometres northwest of Melut on 7-8 April, heightening Lakes Unity 200,000 tension in the state and causing some pre- Upper Nile emptive movements of people. -

Ulang Town, Nyangora, Barmach, Ulang County, Upper Nile State
IRNA Report: [Ulang Town, Nyangora, Barmach, Ulang County, Upper Nile State] [18-20 September 2014] This IRNA Report is a product of Inter-Agency Assessment mission conducted and information compiled based on the inputs provided by partners on the ground including; government authorities, affected communities/IDPs and agencies. Highlights: • Displacement was primarily within Ulang county and IDPs and host community are well integrated • In Ulang town people are primarily returning IDPs while in Nyangora and Barmach they are a mix of IDPs and host community • Preliminary numbers are 8,440 returning IDPs in Ulang town, 4,000 IDPs and 8,000 host community in Nyangora, and 6,300 IDPs and 7,600 host community in Barmach • Proxy malnutrition at very high rates, SAM 16.6%, MAM 28.4%, and GAM 45% Food distribution and re-establishment of health and nutrition services also high priorities • • NGOs planning response include GOAL (health and nutrition), ADRA (education), Nile Hope (protection), NP (protection), Medair (WASH), and Food For the Hungry with WFP (FSL) • As Ulang is on the Malakal – Nasir road, it is vulnerable to attack in the dry season. Contingencies to move operations to Nyangora (across the river in sight of Ulang town) must therefore be in place, or response should focus on Nyangora to begin with. Situation overview From 18-20 September a joint assessment team visited Ulang town, Nyangora, and Barmach in Ulang County, Upper Nile State, to assess reports of humanitarian need resulting from conflict-related displacement that occurred in the first half of 2014. On 18 and 20 September the team assessed Ulang town and on 19 September the team split and assessed Nyangora and Barmach, across the Sobat river from Ulang town. -
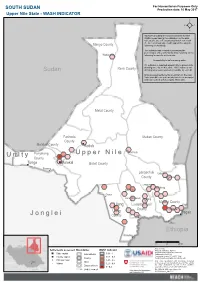
Jonglei Unity Upper Nile
For Humanitarian Purposes Only SOUTH SUDAN Production date: 10 May 2017 Upper Nile State - WASH INDICATOR REACH calculated the areas more likely to have WASH needs basing the estimation on the data collected between February and March 2017 with the Area of Knowledge (AoK) approach, using the Manyo County following methodology. The indicator was created by averaging the percentages of key informants (KIs) reporting on the Wadakona following for specific settlements: - Accessibility to safe drinking water 0% indicates a reported impossibility to access safe Renk County drinking water by all KIs, while 100% indicates safe Sudan drinking water was reported accessible by each KI. Only assessed settlements are shown on the map. Values for different settlements have been averaged and represented with hexagons 10km wide. Melut County Fashoda Maban County County Malakal County Kodok Panyikang Guel Guk Ogod U p p e r N i l e U n i t y County Tonga Malakal Baliet County Pakang Longochuk Udier County Chotbora Longuchok Mathiang Kiech Kon Dome Gum (Kierwan) Mading Maiwut County Ulang Luakpiny/Nasir Kigili County Maiwut Ulang Pagak J o n g l e i County Jikmir Jikou Ethiopia Wanding Sudan 0 25 50 km Data sources: Ethiopia Settlements assessed Boundaries WASH indicator Thematic indicators: REACH Administrative boundaries: UNOCHA; State capital International 0.81 - 1 Settlements: UNOCHA; County capital 0.61 - 0.8 Coordinate System:GCS WGS 1984 C.A.R. County Contact: [email protected] Principal town 0.41 - 0.6 Note: Data, designations and boundaries contained Juba State Village 0.21 - 0.4 on this map are not warranted to be error-free and do not imply acceptance by the REACH partners, Disputed area associates, donors or any other stakeholder D.R.C. -

Sudan's North
Concordis International Sudan Report September 2010 MORE THAN A LINE: SUDAN’S NORTH - SOUTH BORDER SEPTEMBER 2010 02 Concordis International Sudan Report Contents Contents 04 Acknowledgements 50 Abyei 1.1 Snapshot Summary 1.2 Conflict Drivers 05 Glossary 1.2.1 National Political Context 1.2.2 Border Demarcation and the 08 Executive Summary Abyei Referendum 1.1 General Findings 1.2.3 Physical Demarcation 1.2 Thematic Findings 1.2.4 Land 1.3 Conflict Prone Areas 1.2.5 Militarisation 14 Introduction 1.3.6 Additional Factors 1.1 General Findings 1.4 Conflict Management 1.2 Thematic Findings 1.3 Conflict Prone Areas 67 Southern Kordofan/Unity 1.1 Snapshot Summary 28 South Darfur-Western Bahr al Ghazal 1.2 Conflict Drivers 1.1 Snapshot Summary 1.2.1 Transhumance 1.2 Conflict Drivers 1.2.2 Political Marginalisation 1.2.1 Border demarcation 1.2.3 Hardening Conflict Memory 1.2.2 Militarisation 1.2.4 Land/Oil and Demarcation 1.2.3 SPLA-Rezeigat Clashes 1.2.5 Community Land 1.2.4 Other Armed Groups 1.2.6 Militarisation 1.2.5 Wider Regional Instability 1.2.7 Community Conflict Management 1.2.6 Conflict Trends 1.3 Conflict Trends and Mitigation 1.3 Conflict Mitigation 79 Southern Kordofan 38 South Darfur-Northern Bahr al Ghazal 1.1 Snapshot Summary 1.1 Snapshot Summary 1.2 Conflict Drivers 1.2 Conflict Drivers 1.2.1 National Political Context 1.2.1 Contested Rights Along the 1.2.2 Land Grazing Area 1.2.3 Socio-economic Underdevelopment 1.2.2 Transportation of Arms 1.2.4 Integration of Adminstration 1.2.3 Militarisation 1.2.5 Security Integration and -

Fashoda Youth Forum Allocation Type
Requesting Organization : Fashoda Youth Forum Allocation Type : 1st Round Standard Allocation Primary Cluster Sub Cluster Percentage EDUCATION 100.00 100 Project Title : Lifesaving Education program for Upper Nile State Allocation Type Category : Frontline services OPS Details Project Code : SSD-16/E/88945 Fund Project Code : SSD-16/HSS10/SA1/E/NGO/695 Cluster : Education Project Budget in US$ : 119,995.15 Planned project duration : 6 months Priority: 1 Planned Start Date : 01/01/2016 Planned End Date : 30/06/2016 Actual Start Date: 01/01/2016 Actual End Date: 30/06/2016 Project Summary : The aim of this project is to provide life-saving education and youth-focused life skills vocational training for a total of 3,350 children, that is –1650 displaced children and 1700 host community children of both (girls and boys) and 125 adult (60 Teachers and 65 PTAs (men and women) in both Lul and Kodok Payams of Fashoda County. The project will provide training and services in life skills, PSS and child protection in schools, and also provide youth-focused PSS and Life Skills training for young people out of school in order to enroll them back into schools activities. TLS constructed earlier will be maintained to provide access to learning activities for the children school facilities will be rehabilitated also to provide child-friendly spaces which can continue to deliver lifesaving messages to the children. Sanitation facilities will be provided also to all the school facilities to prevent the spread of diseases and awareness on cholera will be raised thus promoting healthy and hygienic school environments.