Thoracic Wall Foreign Bodies Following Penetrating Trauma in Pediatric Age Group: Report of Two Cases with Literature Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

THORAX ANATOMY LAB 1: LEARNING OBJECTIVES Thoracic Wall, Pleural Cavities, and Lungs
THORAX ANATOMY LAB 1: LEARNING OBJECTIVES Thoracic Wall, Pleural Cavities, and Lungs Primary Learning Objectives 1. Define thorax and state the structures that form its anatomical boundaries. 2. Describe the locations and boundaries of the superior thoracic aperture (clinical: thoracic outlet) and the inferior thoracic aperture. Identify the costal arch (margin) and state the ribs that form the arch. 3. Identify and palpate the bones that compose the sternum (manubrium, body, and xiphoid process) and associated osteological features: jugular notch, clavicular notch, and sternal angle. 4. For the sternal angle, identify its associated vertebral level, state its anatomical relationship to the trachea and aorta, state its significance in creating an anatomical division of the mediastinum, and identify the ribs that join the sternum at its location. 5. Identify and palpate the clavicle, sternum, ribs, costal cartilages, intercostal spaces, and thoracic vertebrae. 6. Differentiate true ribs from false and floating ribs. 7. Identify the following osseous features on a rib: head, necK, rib (costal) tubercle, body, shaft, and the costal groove. 8. State the weaKest region of the rib that is commonly fractured and describe the anatomy and physiology involving flail chest. 9. Describe the possible clinical manifestations of supernumerary ribs. 10. Identify the following rib joints: costovertebral (costotransverse joint and vertebral body joint) and sternocostal. 11. Identify the transversus thoracis muscle, the external, internal, and innermost intercostal muscles, and state their innervation, blood supply, and functions. 12. State the structures that compose the neurovascular bundle within each intercostal space and identify each neurovascular bundle by number. 13. Identify the neurovascular bundle inferior to the twelfth rib and state the names of each structure composing the bundle (subcostal artery, subcostal vein, and subcostal nerve). -

E Pleura and Lungs
Bailey & Love · Essential Clinical Anatomy · Bailey & Love · Essential Clinical Anatomy Essential Clinical Anatomy · Bailey & Love · Essential Clinical Anatomy · Bailey & Love Bailey & Love · Essential Clinical Anatomy · Bailey & Love · EssentialChapter Clinical4 Anatomy e pleura and lungs • The pleura ............................................................................63 • MCQs .....................................................................................75 • The lungs .............................................................................64 • USMLE MCQs ....................................................................77 • Lymphatic drainage of the thorax ..............................70 • EMQs ......................................................................................77 • Autonomic nervous system ...........................................71 • Applied questions .............................................................78 THE PLEURA reections pass laterally behind the costal margin to reach the 8th rib in the midclavicular line and the 10th rib in the The pleura is a broelastic serous membrane lined by squa- midaxillary line, and along the 12th rib and the paravertebral mous epithelium forming a sac on each side of the chest. Each line (lying over the tips of the transverse processes, about 3 pleural sac is a closed cavity invaginated by a lung. Parietal cm from the midline). pleura lines the chest wall, and visceral (pulmonary) pleura Visceral pleura has no pain bres, but the parietal pleura covers -

Variations in Dimensions and Shape of Thoracic Cage with Aging: an Anatomical Review
REVIEW ARTICLE Anatomy Journal of Africa, 2014; 3 (2): 346 – 355 VARIATIONS IN DIMENSIONS AND SHAPE OF THORACIC CAGE WITH AGING: AN ANATOMICAL REVIEW ALLWYN JOSHUA, LATHIKA SHETTY, VIDYASHAMBHAVA PARE Correspondence author: S.Allwyn Joshua, Department of Anatomy, KVG Medical College, Sullia- 574327 DK, Karnataka,India. Email: [email protected]. Phone number; 09986380713. Fax number – 08257233408 ABSTRACT The thoracic cage variations in dimensions and proportions are influenced by age, sex and race. The objective of the present review was to describe the age related changes occurring in thoracic wall and its influence on the pattern of respiration in infants, adult and elderly. We had systematically reviewed, compared and analysed many original and review articles related to aging changes in chest wall images and with the aid of radiological findings recorded in a span of four years. We have concluded that alterations in the geometric dimensions of thoracic wall, change in the pattern and mechanism of respiration are influenced not only due to change in the inclination of the rib, curvature of the vertebral column even the position of the sternum plays a pivotal role. Awareness of basic anatomical changes in thoracic wall and respiratory physiology with aging would help clinicians in better understanding, interpretation and to differentiate between normal aging and chest wall deformation. Key words: Thoracic wall; Respiration; Ribs; Sternum; vertebral column INTRODUCTION The thoracic skeleton is an osteocartilaginous cage movement to the volume displacement of the frame around the principal organs of respiration lungs was evaluated by (Agostoni et al,m 1965; and circulation. It is narrow above and broad Grimby et al., 1968; Loring, 1982) for various below, flattened antero-posteriorly and longer human body postures. -

LATISSIMUS DORSI FLAP for HEAD and NECK RECONSTRUCTION Patrik Pipkorn, Ryan Jackson, Bruce Haughey
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY LATISSIMUS DORSI FLAP FOR HEAD AND NECK RECONSTRUCTION Patrik Pipkorn, Ryan Jackson, Bruce Haughey The latissimus dorsi is the largest muscle in Benefits the body by surface area. It can be as large as 20 x 40cms, enabling latissimus dorsi • Easy flap to learn to harvest flaps to cover very large defects (Figure 1). • Large thin muscle that can cover very large defects • Long (5-15cm) vascular pedicle if dis- sected up to the subscapular artery • The subscapular artery has a diameter of 2-5mm • Minimal long-term donor site morbidity • Can be harvested as a muscle flap or with a skin paddle • Can be harvested as a chimeric flap (multiple otherwise independent flaps that each have an independent vascular supply with all pedicles linked to a common source vessel) along with other flaps based on a singular subscapular artery Caveats • Donor site is close to head and neck area making two team harvest difficult, though not impossible Figure 1: Large pedicled latissimus dorsi • Because the donor site is on the back, it flap makes positioning more tedious • Large wound and potential dead space The flap can be harvested as a pedicled or after harvest has high risk of a seroma free flap and as a muscular or myocuta- neous flap with an overlying skin paddle. It can also be harvested along with any other Surgical anatomy flap based on the subscapular vascular system as a chimeric or subscapular “mega- The latissimus dorsi mainly adducts and flap”. Despite its size it can be harvested medially rotates the arm. -
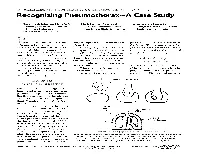
Recognizing Pneumothorax-A Case Study
Recognizing Pneumothorax-A Case Study Mary Black Johnson, PhD, ATC Mark Haines, MA, ATC Brian Barry, MA, ATC Metropolitan State College Assistant Athletic Trainer The Jim Davis Connection Denver, Colorado San Diego State University Carlsbad, California 9%-neumothorax injuries are lung to expand fully within its own position and air is expired from infrequent but can be life threat- pleural sac. the lungs. The passive expiration ening. They are most often associ- During inspiration, the dia- process becomes active and is facili- ated with blunt trauma of the phragm contracts and flattens tated by contraction of abdominal chest. The trauma causes rib frac- while the ribs are lifted by contrac- and chest muscles during exercise. ture, which in turn perforates the tion of the intercostal muscles. pleural wall. Thus, air or gas accu- Thus, the negative pressure in- 9njuw Changes mulates in the pleural cavity and creases, resulting in air flow from in Respiration causes the lung to collapse. It is the atmosphere into the increased critical to recognize the signs and area of the lungs. When the chest wall is pierced, in symptoms of this condition in or- When the muscles involved in either an open or closed chest in- der to provide prompt and suc- respiration relax, the diaphragm jury, normal pressure gradients cessful treatment in what can be a returns to its dome-shaped resting are altered. The normal pressure medical emergency. , fluid-filled balloon Dynamics 1 , of Normal Breathing Within the thoracic cage, each lung resides in a separate com- partment, the pleural sac. Between the thoracic wall and the pleural sac is a thin layer of intrapleural fluid (Vander et al., 1985) (Fig- ure 1). -

Human Anatomy: Thoracic Wall
Thoracic wall - structure, blood supply and innervation Ingrid Hodorová UPJŠ LF, Dept. of Anatomy MediTec training for students 1.-15.9.2019, Kosice, Slovakia Thoracic borders external - Upper: jugular notch, clavicule, acromion scapulae, spine of C7 (vertebra prominens) Lower: xiphoid process, costal arches (right and left), Th12 internal - Upper: superior thoracic aperture: jugular notch, 1. pair of ribs, Th1 Lower: inferior thoracic aperture: diaphragm (right side - to 4. ICS left side - to 5. ICS) Lines of orientation Anterior axillary l. Anterior median line (midsternal) Scapular l. Sternal line Middle axillary l. Paravertebral l. Parasternal l. Posterior median line Midclavicular l. Posterior axillary l. Layers of thoracic wall ► Deep layer - osteothorax, muscles of proper thoracic wall + intrinsic muscles of the back, deep structures, endothoracic fascia ► Middle layer - thoracohumeral mm., spinohumeral mm., spinocostal mm., (fascie, vessels, nerves) ► Superficial layer - skin, subcutaneous tissue, superficial structures, mammary gland ►Deep layer Osteothorax - ribs - sternum - thoracic vertebrae Osteothorax Ribs Types of ribs: Sternum - manunbrium of sternum - body of sternum - xiphoid process - manunbriosternal and xiphisternal synchondrosis(synostosis) Movement of the ribs and sternum during breathing Thoracic vertebrae - body - arch (lamina+pedicles) - spinous process - transverse processes - superior and inferior articular processes Joints of the ribs anteriorly ►sternocostal joints (2nd-5th ribs) posteriorly ►costovertebral -

Thorax Syllabus
THORAX COURSE CONTENT COMPETENCIES The first year medical student should be able to understand and describe the gross anatomy of thoracic wall, mediastinum and the contents of thoracic cavity, correlate the anatomical basis of clinical manifestations /clinical procedures pertaining to thorax and describe the radiological anatomy of thorax. REGIONS AND ORGANS THORACIC WALL THORACIC INLET Boundaries and contents Level 2: Details Level 3: Thoracic outlet syndrome THORACIC OUTLET Boundaries, diaphragm,attachments, major openings and their vertebral levels Level 2: Functional correlation; Minor openings Level 3: Development and congenital anomalies RIB CAGE THORAX Typical intercostal space – Boundaries and contents; Atypical intercostal space; Movements of respiration Level 2: Accessory muscles of respiration Level 3: Applied aspects: Barrel chest, pectus excavatum, rickety rosary MEDIASTINUM Divisions and major contents Level 2: Details Level 3: Applied aspects: Mediastinitis, mediastinoscopy SUPERIOR AND POSTERIOR MEDIASTINA Boundaries and contents: Trachea, Oesophagus, Aorta, Azygos system, Thoracic duct Level 2: Superior mediastinal Syndrome, Course, relation and branches / area of drainage Level 3: Applied aspects: Coarctation of aorta, aneurysm, developmental anomalies PLEURA Pleural reflections, recesses, innervation Level 2: Functional importance of recesses Level 3: Pleuritis, pleural effusion, pleural tap, posterior approach to kidney (importance of pleural reflection) 41 LUNGS Gross description including lobes, fissures and bronchopulmonary -

Osteoradionecrosis of the Anterior Thoracic Wall After Radiation
J Korean Soc Radiol 2019;80(5):1003-1007 Case Report https://doi.org/10.3348/jksr.2019.80.5.1003 pISSN 1738-2637 / eISSN 2288-2928 Received February 23, 2018 Revised August 9, 2018 Accepted December 18, 2018 Osteoradionecrosis *Corresponding author Jung-Hee Yoon, MD Department of Radiology, of the Anterior Thoracic Wall Haeundae Paik Hospital, Inje University College of Medicine, 875 Haeun-daero, Haeundae-gu, after Radiation Therapy Busan 48108, Korea. Tel 82-51-797-0355 Fax 82-51-797-0379 for Breast Cancer E-mail [email protected] 유방암으로 방사선 치료를 받은 후 흉벽에 발생한 This is an Open Access article distributed under the terms of 방사선 골괴사 the Creative Commons Attribu- tion Non-Commercial License 1 2 (https://creativecommons.org/ Young Seon Kim, MD , Jung-Hee Yoon, MD * licenses/by-nc/4.0) which permits 1 Department of Radiology, Yeungnam University Medical Center, College of Medicine, unrestricted non-commercial use, distribution, and reproduc- Yeungnam University, Daegu, Korea 2 tion in any medium, provided the Department of Radiology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea original work is properly cited. ORCID iDs Although osteoradionecrosis of the thoracic wall is rare, severe complications following radia- Jung-Hee Yoon tion therapy for breast cancer can occur. The authors report the case of a 65-year-old woman https:// orcid.org/0000-0001-5152-6668 who developed osteoradionecrosis in the left thoracic wall 17 years after undergoing radiation Young Seon Kim therapy for breast cancer. Chest CT revealed fractures in the left third and fourth ribs as well as https:// in the sternal body, with severe sclerotic and lytic changes and cortical irregularity. -
Thoracic Wall
Thoracic wall . Region of the body between the neck and abdomen . Flattened in front and behind, but rounded on the sides . The bony framework of the walls is called the thoracic cage, which is formed of: . Vertebral column . Ribs & intercostal spaces . Sternum and costal cartilages Superiorly: It communicates1st rib with the neck through an opening bounded:1 . Posteriorly by 1st thoracic vertebra . Laterally by medial border of the 1st ribs and their costal cartilages . Anteriorly by superior border of manubrium sterni Suprapleural This opening is occupied: membrane . In the midline, by the structures that pass between the neck and the thorax . On either sides, it is closed by a dense suprapleural membrane Suprapleural Membrane . Tent shaped dense fascial sheet that covers the apex of each lung. An extension of the endothoracic fascia . Extends approximately an inch superior to the superior thoracic aperture . It is attached: • The thoracic cage: . Protects the lungs, heart and large vessels . Provides attachment to the muscles of thorax, upper limb, abdomen & back • The cavity of thorax is divided into: • A median partition, the mediastinum • Laterally placed pleurae & lungs Cutaneous Nerves Anterior wall: . Above the level of sternal angle: Supraclavicular nerves . Below the level of sternal angle: Segmental innervation by anterior and lateral cutaneous branches of the intercostal nerves Posterior wall: . Segmental innervation by posterior rami of the thoracic spinal nerves nerves The Intercostal Space Intercostal Space It is the space between two ribs Since there are 12 ribs on each side, there are 11 intercostal spaces. Each space contains: . Intercostal muscles . Intercostal neurovascular bundle . Lymphatics Intercostal muscles • External Intercostal • Internal Intercostal • Innermost Intercostal Supplied by corresponding intercostal nerves Action: • Tend to pull the ribs nearer to each other . -

1. Anatomical Basis of Thoracic Surgery
BWH 2015 GENERAL SURGERY RESIDENCY PROCEDURAL ANATOMY COURSE 1. ANATOMICAL BASIS OF THORACIC SURGERY Contents Lab objectives ............................................................................................................................................... 2 Knowledge objectives ............................................................................................................................... 2 Skills objectives ......................................................................................................................................... 2 Preparation for lab ....................................................................................................................................... 2 1.1 BASIC PRINCIPLES OF ANATOMICAL ORGANIZATION ............................................................................ 4 1.2 THORACIC CAVITY AND CHEST WALL ..................................................................................................... 9 1.3 PLEURA AND LUNGS ............................................................................................................................. 13 1.4 ORGANIZATION OF THE MEDIASTINUM .............................................................................................. 19 1.5 ANTERIOR mediastinum ....................................................................................................................... 23 Thymus ................................................................................................................................................... -
Notes on the Thorax
Notes on the Thorax Anatomy RHS 241 Lecture 19 Dr. Einas Al-Eisa Osteology of thorax •Ribs • Thoracic vertebrae • Sternum Ribs • True ribs (vertebrosternal ribs): 1st seven or eight ribs • False ribs (vertebrochondral ribs): ribs 8-10 • Floating ribs (free): 11 & 12 • Costosternal joints: ¾1st: cartilagenous ¾2nd –7th: synovial Thoracic vertebrae • Body • Pedicle • Laminae • Vertebral formina • Transverse process • Spinous process • Superior & inferior articular processes Neurovascular bundles • Travel in the costal groove of the ribs (i.e., in the superior portion of the intercostal space) between the internal and innermost intercostals • Physicians passing needles into the thorax insert them just superior to the rib to avoid damaging the bundle Sternum • Manubrium • Jugular notch • Xiphoid process • Sternal angle or Angle of Louis (at the junction of the manubrium & body of sternum): T4-T5 level Surface landmarks • The scapula covers the 2nd to 7th ribs posteriorly (important landmark for defining lung fields) •The 2nd rib joins the sternum at the level of the sternal angle (palpable landmark) Surface anatomy • Suprasternal notch • Clavicle • Sternal angle • Xiphoid process • Sternal attachments for ribs Articulations • Ribs 1, 11, & 12 articulate with their respective vertebrae • Ribs 2-10 articulate with their own vertebra and with the one above • Type of joints? Boundaries of the thoracic inlet • The manubrium anteriorly •1st ribs and costal cartilage laterally •1st thoracic vertebra posteriorly Pectoral region • Pectoralis major: -

Thoracic Trauma I and II
Thoracic Trauma I and II: Matthew W. Beal, DVM Diplomate ACVECC College of Veterinary Medicine; Michigan State University, East Lansing, MI Introduction: Traumatized small animal patients represent a population in which a standardized approach to diagnosis centered on thorough background knowledge of traumatic injuries coupled with a complete physical examination will allow for rapid therapeutic interventions and optimization of patient care. The following paragraphs will detail the pathophysiology, diagnostic methods, and emergency medical treatment for injuries sustained due to both blunt and penetrating thoracic trauma from an anatomically based approach. Thoracic injury occurs most commonly as a result of blunt trauma. Common causes include being hit-by car, falling from a height (high-rise syndrome), big-dog-little-dog interactions, and human-animal interactions. Penetrating injury (projectile induced injury, big-dog-little-dog interactions, and impalement injuries) occurs with less frequency than blunt thoracic injuries, but it must be recognized that both can result in immediately life threatening problems. Trauma Associated Pleural Space Disease: Pneumothorax, Hemothorax, and Diaphragmatic Hernia make up the three acute trauma associated pleural space diseases. Patients with clinically significant trauma associated pleural space diseases will likely display signs of tachypnea, dyspnea, and muffled heart and lung sounds on auscultation of the thorax. Pneumothorax is the accumulation of air in the pleural space between the parietal and visceral pleura. Pneumothorax is classified as “open” when air enters the pleural space from an external wound, or “closed” when air enters the pleural space due to pulmonary or mediastinal injury. Tension pneumothorax occurs when air accumulates within the pleural space via a one-way-valve effect allowing air to enter, but not leave the pleural space.