Chapter 2 Railway Accident and Serious Incident Investigation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Logistics Facility to Be Developed in Hirakata, Osaka Prefecture --Total Floor Space 20,398.12 M2; Whole-Building Lease to OTT Logistics Co., Ltd
August 11, 2014 FOR IMMEDIATE RELEASE Contact Information: ORIX Corporation Corporate Planning Department Tel: +81-3-3435-3121 Fax: +81-3-3435-3154 URL: http://www.orix.co.jp/grp/en/ Logistics Facility in the BCP-suitable Kansai Inland Area Logistics Facility to Be Developed in Hirakata, Osaka Prefecture --Total Floor Space 20,398.12 m2; Whole-Building Lease to OTT Logistics Co., Ltd-- TOKYO, Japan – August 11, 2014 - ORIX Corporation (TSE: 8591; NYSE: IX), a leading integrated financial services group, today announced that it has decided to develop a BTS*1 logistics facility in Hirakata, Osaka Prefecture. The development area for this project is in an industrial park located approximately 3 km from the Hirakata-higashi and Hirakata Gakken interchanges on the Second Keihan Highway, and approximately 1.5 km from Nagao Station on the JR Katamachi Line. The location is suitable for deliveries to the Osaka and Kyoto areas, being located approximately 3 km from National Route 1, a major highway connecting Kyoto and Osaka. Moreover, from the business continuity planning perspective, the Kansai inland area is highly sought-after and considered scarce land resources suitable for logistics facility development. The project includes a whole-building lease to OTT Logistics Co., Ltd. The five-story building (four stories in the warehouse section) will have a gross area of 20,398.12 m2 on a site of 10,629.36 m2. Construction will commence in September 2014, and is scheduled for completion in July 2015. The ORIX Group’s logistics investment business started in 2003, initially focused in the development of BTS facilities. -

West Japan Railway Group Integrated Report 2019 —Report on Our Value for Society—
Continuity Progress Making Our Vision into Reality West Japan Railway Group Integrated Report 2019 —Report on Our Value for Society— West Japan Railway Company Contents 2 On the publication of “JR-West Group Integrated Report 2019” 3 Values held by the JR-West Group Our Starting Point 5 The derailment accident on the Fukuchiyama Line 11 Recovering from heavy rain damage through cooperation and think-and-act initiatives 13 Business activities of JR-West Group 15 The president’s message 17 The value we seek to provide through the non-railway business —Messages from group company Presidents Strategy of 21 Steps toward our vision 21 JR-West Group Medium-Term Management Plan 2022: approach & overview Value Creation 23 Toward long-term sustainable growth for Our Vision 25 Progress on Groupwide strategies—example initiatives 27 Promoting our technology vision 29 Special Three-Way Discussion The challenge of evolving in the railway/transportation field in an era of innovation 33 Fiscal 2019 performance in priority CSR fields and fiscal 2020 plans for priority initiatives 37 Safety 47 Customer satisfaction 51 Coexistence with communities A Foundation 55 Human resources/motivation Supporting 59 Human rights Value Creation 61 Global environment 67 Risk management 71 Corporate governance 73 Special Three-Way Discussion The role of the Board of Directors in achieving sustainable growth and enhancing corporate value 77 Initiatives in each business 81 Consolidated 10-year financial summary Data 83 Financial statements 87 Recognizing and responding to risks and opportunities 88 Data related to human resources and motivation (non-consolidated) Corporate profile (as of March 31, 2019) Scope As a rule, JR-West Group (including some Company name West Japan Railway Company initiatives at the non-consolidated level). -

Wakayama and Sakurai Line
1 / 32 Contents 1. Route information.................................................................................................... 3 1.1 Background information .............................................................................................. 3 1.2 The Route map .............................................................................................................. 4 1.3 ATS Safety system ......................................................................................................... 5 1.4 Route signs and train stop position ........................................................................... 6 1.5 Kitauchi station operation ........................................................................................... 9 2. 103 series EMU ....................................................................................................... 10 2.1 Basic information ........................................................................................................ 10 2.2 External models ........................................................................................................... 11 2.3 The consist ................................................................................................................... 12 2.4 The cab ......................................................................................................................... 13 2.5 Cabin view .................................................................................................................... 16 -

Transport Information Guide Tug of War Shinjo Kenmin Athletic Field 1
Transport Information Guide Sport & Discipline Venue Nara Pref. Shinjo Kenmin Katsuragi City Athletic Field 1 292-3 Shinmachi, Katsuragi City, Nara www.city.katsuragi.nara.jp/index.cfm/17,2969,80,html ※There is an other venue. Please check each venue. Tug of War ・ Kashiba City General Gymnasium ■Recommended route to the venue From Osaka Station (Center Village) to the venue ( OP Original Kansai One Pass usable section WP Original JR Kansai Wide Area Pass usable section) Osaka Oji Yamato-Shinjo Venue Sta. Sta. Sta Traffic Mode Line Depart Arrive Route Time pass Osaka Loop Line / Yamatoji Line Train JR Osaka Sta. Oji Sta. OP WP 42min. for Kamo Wakayama Line Train JR Oji Sta. Yamato-Shinjo Sta. OP WP 24min. for Gojo Shuttle Yamato-Shinjo Sta. Venue 5min. bus Osaka Tennoji Osaka-Abenobashi Sta. Sta. Sta. Shakudo Kintetsu-Shinjo Venue Sta. Sta. Traffic Mode Line Depart Arrive Route Time pass Osaka Loop Line Train JR Osaka Sta. Tennoji Sta. OP WP for Tennoji 16min. ※5-minute walk to Kintetsu Line. Kintetsu Minami-Osaka Line Train Osaka-Abenobashi Sta. Shakudo Sta. OP 30min. Railway for Gose Kintetsu Gose Line Train Shakudo Sta. Kintetsu-Shinjo Sta. OP 5min. Railway for Kintetsu-Gose Shuttle Kintetsu-Shinjo Sta. Venue 5min. bus From Masters Village Nara to the venue Masters Village Nara: "Nara Visitor Center & Inn” ※ 16-minute walk from JR Nara Station, 8-minute walk from Kintetsu Nara Station Nara Visitor Nara Oji Yamato-Shinjo Venue Center & Inn Sta. Sta. Sta Traffic Mode Line Depart Arrive Route Time pass Walking Masters Village Nara Sta. -
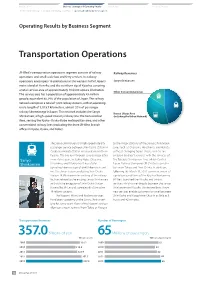
Operating Results by Business Segment — —
Introduction Business Strategy and Operating Results ESG Section Financial Section The President’s Message Medium-Term Management Plan Operating Results by Business Segment — — Operating Results by Business Segment Transportation Operations JR-West’s transportation operations segment consists of railway Railway Revenues operations and small-scale bus and ferry services. Its railway operations encompass 18 prefectures in the western half of Japan’s Sanyo Shinkansen main island of Honshu and the northern tip of Kyushu, covering a total service area of approximately 104,000 square kilometers. Other Conventional Lines The service area has a population of approximately 43 million people, equivalent to 34% of the population of Japan. The railway network comprises a total of 1,222 railway stations, with an operating route length of 5,015.7 kilometers, almost 20% of passenger railway kilometerage in Japan. This network includes the Sanyo Kansai Urban Area Shinkansen, a high-speed intercity railway line; the Kansai Urban (including the Urban Network) Area, serving the Kyoto–Osaka–Kobe metropolitan area; and other conventional railway lines (excluding the three JR-West branch offices in Kyoto, Osaka, and Kobe). The Sanyo Shinkansen is a high-speed intercity to the major stations of the Sanyo Shinkansen passenger service between Shin-Osaka Station in Line, such as Okayama, Hiroshima, and Hakata, Osaka and Hakata Station in Fukuoka in northern without changing trains. These services are Kyushu. The line runs through several major cities enabled by direct services with the services of Sanyo in western Japan, including Kobe, Okayama, the Tokaido Shinkansen Line, which Central Shinkansen Hiroshima, and Kitakyushu. -

Hirakata Logistics Center Completed in Osaka Prefecture
Hirakata Logistics Center Completed in Osaka Prefecture TOKYO, Japan – July 31, 2015 - ORIX Corporation (“ORIX”), a leading integrated financial services group, announced that the construction of its BTS1 logistics facility, "Hirakata Logistics Center (the “Facility”)," located in Hirakata, Osaka Prefecture, completed today. The Facility is located in an industrial park located approximately 3 km from the Hirakata-higashi and Hirakata Gakken interchanges on the Second Keihan Highway, and approximately 1.5 km from Nagao Station on the JR Katamachi Line. The location is suitable for deliveries to the Osaka and Kyoto areas, being located approximately 3 km from National Route 1, a major highway connecting Kyoto and Osaka. The inland area in Kansai, where the Facility resides, is also in high demand for BCP sites. The Facility is a five-story building (four stories in the warehouse section) with the total floor space of 20,398.12 square meters on a site of 10,629.36 square meters. The Facility has been leased to OTT Logistics Co., Ltd. simultaneously when the construction of the building has completed. The ORIX Group‘s logistics investment business started in 2003, initially focused in the development of BTS facilities. From around 2008, utilizing its accumulated expertise, ORIX began shifting the business’ primary focus to the development of multi-tenanted facilities2. To date, ORIX has developed around 1,150,000 m2 of logistics facilities. Going forward, ORIX will provide value added services that leverage its unique group network to differentiate itself, as it continues to operate logistics facility development projects that contribute to meeting market demand. -

Itinerary Japan
Transportation By Train Date Destination From To Remark w/o JR Pass JR Pass Station Track Time Station Track Time TOTAL Monday, 16 Nov 15 Ueno Park Narita Int Airport 09.15 Tokyo 1 10.17 Ltd. Exp Narita Express 8 ¥ 2,820 ¥ ‐ Tokyo 7 10.26 Ueno 6 10.31 JR Joban Line for TSUCHIURA Sightseeing Ueno 12.36 Akihabara 12.39¥ 140 ¥ ‐ JR Yamanote Line for OSAKI Osaka Akihabara 14.20 Tokyo 14.23 JR Keihin‐Tohoku/Negishi Line Rapid for ISOGO Tokyo 17 14.33 Shin‐Osaka 24 17.26 Shinkansen Hikari 517 Shin‐Osaka 16 17.38 Osaka 4 17.42 ¥ 13,940 ¥ ‐ JR Special Rapid Service for BANSHUAKO Osaka 2 17.45 Kyobashi (Osaka) 17.51 JR Kansai Airport Rapid Service for KYOBASHI Kyobashi (Osaka) 17.53 Teradacho 18.04 Osaka Loop Line for TENNOJI Shinsaibashi Shopping Street Teradacho 19.01 Tennoji 14 19.03 ¥ 120 ¥ ‐ Osaka Loop Line for TENNOJI Tennoji 19.09 Shinsaibashi 19.17 ¥ 240 ¥ 240 Osaka City Subway Midosuji Line for SHIN‐OSAKA Rest at Hotel Shinsaibashi 21.05 Tennoji 21.14 ¥ 240 ¥ 240 Osaka City Subway Midosuji Line for TENNOJI Tennoji 11 21.20 Teradacho 21.22 ¥ 120 ¥ ‐ Osaka Loop Line for OSAKA TOTAL ¥ 17,620 ¥ 480 Tuesday, 17 Nov 15 Osaka Castle Teradacho 08.33 Osakajokoen 08.44 ¥ 160 ¥ ‐ Osaka Loop Line for SAKURAJIMA Kiyomizudera Osakajokoen 12.03 Osaka 1 12.12 ¥ 160 ¥ ‐ Osaka Loop Line for OSAKA Drop Luggage at Locker Coin of Osaka Station Osaka 7 12.26 Shin‐Osaka 14 12.30 JR Kyoto Line Local for TAKATSUKI ¥ 2,610 ¥ ‐ Shin‐Osaka 25 12.40 Kyoto 11 12.55 Shinkansen Hikari 468 Kyoto 9 13.07 Tofukuji 13.09 ¥ 140 ¥ ‐ JR Nara Line for JOYO Tofukuji 13.13 Kiyomizu‐gojo 13.16 ¥ 150 ¥ 150 Keihan Main Line Sub‐Exp. -
JICA Experts Study for the Operations and Maintenance Structure Of
Republic of India Mumbai Metro Rail Corporation JICA Experts Study for the Operations and Maintenance Structure of Mumbai Metro Line 3 Project in India Final Report October 2015 Japan International Cooperation Agency (JICA) Japan International Consultants for Transportation Co., Ltd. PADECO Co., Ltd. 4R Metro Development Co., Ltd JR 15-046 Table of Contents Chapter 1 General issues for the management of urban railways .............................. 1 1.1 Introduction ........................................................................................................................ 1 1.2 Management of urban railways ........................................................................................ 4 1.3 Construction of urban railways ...................................................................................... 12 1.4 Governing Structure ........................................................................................................ 17 1.5 Business Model ................................................................................................................. 21 Chapter 2 Present situation in metro projects ............................................................ 23 2.1 General .............................................................................................................................. 23 2.2 Metro projects in the world ............................................................................................. 23 2.3 Summary........................................................................................................................ -

Download the PDF of the Guide to the Surrounding Area
4 te u o R ay sw es pr 2 Ex a im sh ro Hi Mitakidera Ryuo Park Nishi-hiroshima Hiroden-nishi-hiroshima Otagawa River Office Koi Branch Office Ota-gawa Flood Cotrol Channel Kogo-bashi Asahi-bashi Shin-koi-bashi koi-bashi Bridge Hiroshima-nishi-Ohashi Bridge Bridge Bridge Bridge Mitaki JR Kabe Line Yamate-bashi Aki-nagatsuka Bridge Coca-Cola Bottlers Japan Shin-ryuo-bashi Mitaki-bashi Bridge Hiroshima Stadium Bridge Shinjo-bashi Bridge Nishi-kan-on-machi Gion-Ohashi Bridge 450 700 Yokogawa Gion sluice Hiroden- Hirose-bashi640 Bridge Nakahiro ohashi Otagawa River Office gate Temmacho 460 Bridge 183 Oshiba Branch Office 570 Yokogawa Sinbashi 1100 620 Bridge Oshiba-bashi Bridge Temma-gawa River Showa-ohashi 1000 Temma-bashi Bridge 1300 Bridge Minami-Kan-on- Shin-Kannon- 330Midori-ohashi 640 700 Oshiba sluice bashi Bridge Bridge gate 1900 740 bashi Bridge Mifune-bashi Dobashi Tokaichi-machi 1000 Bridge Misasa-bashi 54 Eba-sarayama Park 400 720 660 Sorazaya-bashi 1010 Bridge Ushita Bridge Kita-Ohashi Bridge 1100 480 320 330 Eba-yama Park 750 350 Shin-kohei-bashi Honkawa-bashi Aioi-bashi Bridge The West Peace Bridge 680 Eba Bridge Bridge 490 Nakajima Kanzaki-bashi Bridge 270 Johoku Kohei-bashi Bridge 750 280 Central Park Shin-Hakushima 730 Shin-Sumiyoshi- Peace Memorial Park bashi Bridge 720 Mooiyasu-bashi 700 Funairi-bashi Bridge 720 Bridge Yoshijima-bashi Shin-meiji-bashi Hiroshima Castle 670 Bridge 640 The Atomic Bomb Dome 710 Bridge 700 Peace Bridge Kamiyacho-Higashi 730 Ushita-Ohashi Bridge Hiroshima Prefectural Office Ushita Green Park Shiyakusho-mae -

“JR-West Group Medium-Term Management Plan 2017” Overview of Major Initiatives 1 【Safety】
“JR-West Group Medium-Term Management Plan 2017” Overview of Major Initiatives 1 【Safety】 Legend As of May 8, 2017 Black text: Projects indicated at previous update (May 2, 2016) Red text: Projects added since previous update ※Timing has not yet been determined FY2014.3 FY2015.3 FY2016.3 FY2017.3 FY2018.3 FY2019.3~ Strengthen track facilities When replacing track facilities, we are strengthening facilities by transitioning from standard-length rails to continuous welded rails, (prolongation of rail length replacing wood ties with prestressed concrete ties, and using plastic ties on bridges. Investment in with welding , etc.) maintenance to sustain and Maintain safety and To secure safe, reliable transportation service on the Sanyo Shinkansen, we will evaluate expected future risks that could affect structures and implement enhance the increase durability of Sanyo countermeasures, such as reinforcement measures. functions of Shinkansen structures existing facilities Complete replacement of When replacing facilities, we will strive to improve riding comfort by transitioning to systems utilizing a smooth brake control method Sanyo Shinkansen ATC that is suitable for the characteristics of the rolling stock. system: "New ATC" ▼Spring 2017: Transition to new control method As an addition to existing ATS functions, this system backs up crew members through means such as preventing excessive speed and stop-light violation or preventing incorrect door operation and excessive speed in planned speed reduction zone associated with construction work. We have approved the introduction of this system on On-board oriented train the Sanyo Line (Shiraichi–Iwakuni) in the Hiroshima area. We continue to consider the possibility of installing this system on the Fukuchiyama Line (Amagasaki– control system (ground Sasayamaguchi) and Tokaido/Sanyo Line (Maibara–Kamigori) in the Kansai Urban Area. -

Tokyo National Museum
Ⅱ Outline of the National Institutes for Cultural Heritage The Independent Administrative Institution (IAI), National Institutes for Cultural Heritage, was formed in April 2007 through the merging of the IAI National Museums (Tokyo National Museum, Kyoto National Museum, Nara National Museum, and Kyushu National Museum) and the IAI National Research Institutes for Cultural Properties (Tokyo National Research Institute for Cultural Properties and Nara National Research Institute for Cultural Properties), all of which share the same mission: the conservation and utilization of cultural properties. With the addition of the International Research Centre for Intangible Cultural Heritage in the Asia-Pacific Region, which was established in October 2011, the National Institutes for Cultural Heritage now comprise a total of seven separate institutions. Japan’s cultural properties are the precious assets of the Japanese people. In order to preserve and utilize these properties more effectively and efficiently under unified management, each ofthe seven existing institutions plays the following roles: Tokyo National Museum Kyoto National Museum Nara National Museum As Japan’s foremost museum in the The Kyoto National Museum collects, Nara National Museum collects, pre- humanities field, Tokyo National Mu- preserves, manages, and exhibits serves, manages, and displays cultural seum collects, preserves, manages, cultural properties, while also properties, while also conducting re- and displays cultural properties from conducting research and providing search and providing educational pro- across Japan and other Asian regions, educational programs. The focus is gramming. The focus is Buddhist art while also conducting research and pro- on works from the Heian period to and the cultural properties of Nara. viding educational programs. -

Transport Information Guide Tug of War Kashiba City General
Transport Information Guide Sport & Discipline Venue Nara Pref. Kashiba City Kashiba City General Gymnasium 1437 Hommachi, Kashiba City, Nara http://www.kashiba-general-gym.jp/ ※ There is another venue. Please check each venue. Tug of War ・Shinjo Kenmin Athletic Field 1 ■Recommended route to the venue From Osaka Station (Center Village) to the venue ( OP Original Kansai One Pass usable section WP Original JR Kansai Wide Area Pass usable section) Osaka Oji Kashiba Venue Sta. Sta. Sta. Traffic Mode Line Depart Arrive Route Time pass Osaka Loop Line / Yamatoji Line Train JR Osaka Sta. Oji Sta. OP WP 42min. for Kamo Wakayama Line Train JR Oji Sta. Kashiba Sta. OP WP 9min. for Wakayama Walking Kashiba Sta. Venue 10min. Osaka Tsuruhashi Kintetsu-Shimoda Venue Sta. Sta. Sta. Traffic Mode Line Depart Arrive Route Time pass Osaka Loop Line Train JR Osaka Sta. Tsuruhashi Sta. OP WP 16min. for Kyobashi Kintetsu Kintetsu-Shimoda Kintetsu Osaka Line Train Tsuruhashi Sta. OP 29min. Railway Sta. for Kawachi-Kokubu, Yamato-Yagi Kintetsu-Shimoda Walking Venue 8min. Sta. From Masters Village Nara to the the venue Masters Village Nara: "Nara Visitor Center & Inn” ※ 16-minute walk from JR Nara Station, 8-minute walk from Kintetsu Nara Station Nara Visitor Nara Oji Kashiba Venue Center & Inn Sta. Sta. Sta. Traffic Mode Line Depart Arrive Route Time pass Walking Masters Village Nara Sta. 16min. Yamatoji Line Train JR Nara Sta. Oji Sta. OP WP 16min. for Osaka Wakayama Line Train JR Oji Sta. Kashiba Sta. OP WP 9min. for Takada Walking Kashiba Sta. Venue 10min. Nara Visitor Kintetsu Nara Yamato-Saidaiji Center & Inn Sta.