Carbonic Anhydrases: Role in Ph Control and Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Association Analyses of Known Genetic Variants with Gene
ASSOCIATION ANALYSES OF KNOWN GENETIC VARIANTS WITH GENE EXPRESSION IN BRAIN by Viktoriya Strumba A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy (Bioinformatics) in The University of Michigan 2009 Doctoral Committee: Professor Margit Burmeister, Chair Professor Huda Akil Professor Brian D. Athey Assistant Professor Zhaohui S. Qin Research Statistician Thomas Blackwell To Sam and Valentina Dmitriy and Elizabeth ii ACKNOWLEDGEMENTS I would like to thank my advisor Professor Margit Burmeister, who tirelessly guided me though seemingly impassable corridors of graduate work. Throughout my thesis writing period she provided sound advice, encouragement and inspiration. Leading by example, her enthusiasm and dedication have been instrumental in my path to becoming a better scientist. I also would like to thank my co-advisor Tom Blackwell. His careful prodding always kept me on my toes and looking for answers, which taught me the depth of careful statistical analysis. His diligence and dedication have been irreplaceable in most difficult of projects. I also would like to thank my other committee members: Huda Akil, Brian Athey and Steve Qin as well as David States. You did not make it easy for me, but I thank you for believing and not giving up. Huda’s eloquence in every subject matter she explained have been particularly inspiring, while both Huda’s and Brian’s valuable advice made the completion of this dissertation possible. I would also like to thank all the members of the Burmeister lab, both past and present: Sandra Villafuerte, Kristine Ito, Cindy Schoen, Karen Majczenko, Ellen Schmidt, Randi Burns, Gang Su, Nan Xiang and Ana Progovac. -

Table 2. Significant
Table 2. Significant (Q < 0.05 and |d | > 0.5) transcripts from the meta-analysis Gene Chr Mb Gene Name Affy ProbeSet cDNA_IDs d HAP/LAP d HAP/LAP d d IS Average d Ztest P values Q-value Symbol ID (study #5) 1 2 STS B2m 2 122 beta-2 microglobulin 1452428_a_at AI848245 1.75334941 4 3.2 4 3.2316485 1.07398E-09 5.69E-08 Man2b1 8 84.4 mannosidase 2, alpha B1 1416340_a_at H4049B01 3.75722111 3.87309653 2.1 1.6 2.84852656 5.32443E-07 1.58E-05 1110032A03Rik 9 50.9 RIKEN cDNA 1110032A03 gene 1417211_a_at H4035E05 4 1.66015788 4 1.7 2.82772795 2.94266E-05 0.000527 NA 9 48.5 --- 1456111_at 3.43701477 1.85785922 4 2 2.8237185 9.97969E-08 3.48E-06 Scn4b 9 45.3 Sodium channel, type IV, beta 1434008_at AI844796 3.79536664 1.63774235 3.3 2.3 2.75319499 1.48057E-08 6.21E-07 polypeptide Gadd45gip1 8 84.1 RIKEN cDNA 2310040G17 gene 1417619_at 4 3.38875643 1.4 2 2.69163229 8.84279E-06 0.0001904 BC056474 15 12.1 Mus musculus cDNA clone 1424117_at H3030A06 3.95752801 2.42838452 1.9 2.2 2.62132809 1.3344E-08 5.66E-07 MGC:67360 IMAGE:6823629, complete cds NA 4 153 guanine nucleotide binding protein, 1454696_at -3.46081884 -4 -1.3 -1.6 -2.6026947 8.58458E-05 0.0012617 beta 1 Gnb1 4 153 guanine nucleotide binding protein, 1417432_a_at H3094D02 -3.13334396 -4 -1.6 -1.7 -2.5946297 1.04542E-05 0.0002202 beta 1 Gadd45gip1 8 84.1 RAD23a homolog (S. -

An Investigation Into the Carbonic Anhydrase Isozymes from Zea
This file is part of the following reference: Tems, Ursula (2009) Characterization of the carbonic anhydrase isozymes of zea mays. PhD thesis, James Cook University. Access to this file is available from: http://eprints.jcu.edu.au/8807 Characterization of the Carbonic Anhydrase Isozymes of Zea mays Thesis submitted by Ursula TEMS B.Sc. Hons (JCU) February 2009 for the degree of Doctor of Philosophy in the School of Pharmacy and Molecular Sciences James Cook University Statement of Sources I declare that this thesis is my own work and has not been submitted in any form for another degree or diploma at any university or other institution of tertiary education. Information derived from the published or unpublished work of others has been acknowledged in the text and a list of references is given. Signature Date i Statement of Access I, the undersigned, author of this work, understand that James Cook University will make this thesis available for use within the University Library and, via the Australian Digital Theses network, for use elsewhere. I understand that, as an unpublished work, a thesis has significant protection under the Copyright Act and; I do not wish to place any further restriction on access to this work. Signature Date Declaration I, the undersigned, the author of this work, declare that the electronic copy of this thesis provided to the James Cook University Library is an accurate copy of the print thesis submitted, within the limits of the technology available. Signature Date ii Acknowledgements I would like to express my sincere gratitude to my supervisor Jim Burnell for his enthusiasm, encouragement and guidance. -

Role of Amylase in Ovarian Cancer Mai Mohamed University of South Florida, [email protected]
University of South Florida Scholar Commons Graduate Theses and Dissertations Graduate School July 2017 Role of Amylase in Ovarian Cancer Mai Mohamed University of South Florida, [email protected] Follow this and additional works at: http://scholarcommons.usf.edu/etd Part of the Pathology Commons Scholar Commons Citation Mohamed, Mai, "Role of Amylase in Ovarian Cancer" (2017). Graduate Theses and Dissertations. http://scholarcommons.usf.edu/etd/6907 This Dissertation is brought to you for free and open access by the Graduate School at Scholar Commons. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Scholar Commons. For more information, please contact [email protected]. Role of Amylase in Ovarian Cancer by Mai Mohamed A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy Department of Pathology and Cell Biology Morsani College of Medicine University of South Florida Major Professor: Patricia Kruk, Ph.D. Paula C. Bickford, Ph.D. Meera Nanjundan, Ph.D. Marzenna Wiranowska, Ph.D. Lauri Wright, Ph.D. Date of Approval: June 29, 2017 Keywords: ovarian cancer, amylase, computational analyses, glycocalyx, cellular invasion Copyright © 2017, Mai Mohamed Dedication This dissertation is dedicated to my parents, Ahmed and Fatma, who have always stressed the importance of education, and, throughout my education, have been my strongest source of encouragement and support. They always believed in me and I am eternally grateful to them. I would also like to thank my brothers, Mohamed and Hussien, and my sister, Mariam. I would also like to thank my husband, Ahmed. -

High-Throughput Screening Studies of Inhibition of Human Carbonic Anhydrase II and Bacterial Flagella Antimicrobial Activity
Western Michigan University ScholarWorks at WMU Dissertations Graduate College 5-2010 High-Throughput Screening Studies of Inhibition of Human Carbonic Anhydrase II and Bacterial Flagella Antimicrobial Activity Albert A. Barrese III Western Michigan University Follow this and additional works at: https://scholarworks.wmich.edu/dissertations Part of the Biochemistry, Biophysics, and Structural Biology Commons, and the Biology Commons Recommended Citation Barrese, Albert A. III, "High-Throughput Screening Studies of Inhibition of Human Carbonic Anhydrase II and Bacterial Flagella Antimicrobial Activity" (2010). Dissertations. 500. https://scholarworks.wmich.edu/dissertations/500 This Dissertation-Open Access is brought to you for free and open access by the Graduate College at ScholarWorks at WMU. It has been accepted for inclusion in Dissertations by an authorized administrator of ScholarWorks at WMU. For more information, please contact [email protected]. HIGH-THROUGHPUT SCREENING STUDIES OF INHIBITION OF HUMAN CARBONIC ANHYDRASE II AND BACTERIAL FLAGELLA ANTIMICROBIAL ACTIVITY by Albert A. Barrese III A Dissertation Submitted to the Faculty of The Graduate College in partial fulfillment of the requirements for the Degree of Doctor of Philosophy Department of Biological Sciences Advisor: Brian C. Tripp, Ph.D. Western Michigan University Kalamazoo, Michigan May 2010 UMI Number: 3410393 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. UMT Dissertation Publishing UMI 3410393 Copyright 2010 by ProQuest LLC. -
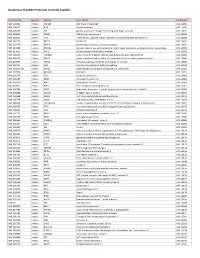
Quantigene Flowrna Probe Sets Currently Available
QuantiGene FlowRNA Probe Sets Currently Available Accession No. Species Symbol Gene Name Catalog No. NM_003452 Human ZNF189 zinc finger protein 189 VA1-10009 NM_000057 Human BLM Bloom syndrome VA1-10010 NM_005269 Human GLI glioma-associated oncogene homolog (zinc finger protein) VA1-10011 NM_002614 Human PDZK1 PDZ domain containing 1 VA1-10015 NM_003225 Human TFF1 Trefoil factor 1 (breast cancer, estrogen-inducible sequence expressed in) VA1-10016 NM_002276 Human KRT19 keratin 19 VA1-10022 NM_002659 Human PLAUR plasminogen activator, urokinase receptor VA1-10025 NM_017669 Human ERCC6L excision repair cross-complementing rodent repair deficiency, complementation group 6-like VA1-10029 NM_017699 Human SIDT1 SID1 transmembrane family, member 1 VA1-10032 NM_000077 Human CDKN2A cyclin-dependent kinase inhibitor 2A (melanoma, p16, inhibits CDK4) VA1-10040 NM_003150 Human STAT3 signal transducer and activator of transcripton 3 (acute-phase response factor) VA1-10046 NM_004707 Human ATG12 ATG12 autophagy related 12 homolog (S. cerevisiae) VA1-10047 NM_000737 Human CGB chorionic gonadotropin, beta polypeptide VA1-10048 NM_001017420 Human ESCO2 establishment of cohesion 1 homolog 2 (S. cerevisiae) VA1-10050 NM_197978 Human HEMGN hemogen VA1-10051 NM_001738 Human CA1 Carbonic anhydrase I VA1-10052 NM_000184 Human HBG2 Hemoglobin, gamma G VA1-10053 NM_005330 Human HBE1 Hemoglobin, epsilon 1 VA1-10054 NR_003367 Human PVT1 Pvt1 oncogene homolog (mouse) VA1-10061 NM_000454 Human SOD1 Superoxide dismutase 1, soluble (amyotrophic lateral sclerosis 1 (adult)) -

Anti-CA1 / Carbonic Anhydrase 1 Antibody (ARG65670)
Product datasheet [email protected] ARG65670 Package: 100 μl, 50 μl anti-CA1 / Carbonic Anhydrase 1 antibody Store at: -20°C Summary Product Description Rabbit Polyclonal antibody recognizes CA1 / Carbonic Anhydrase 1 Tested Reactivity Ms, Rat Tested Application WB Host Rabbit Clonality Polyclonal Isotype IgG Target Name CA1 / Carbonic Anhydrase 1 Antigen Species Human Immunogen Full length fusion protein of Human CA1. Conjugation Un-conjugated Alternate Names Carbonic anhydrase I; EC 4.2.1.1; Carbonate dehydratase I; Carbonic anhydrase B; Car1; HEL-S-11; CA-I; Carbonic anhydrase 1; CAB Application Instructions Application table Application Dilution WB 1:500 - 1:2000 Application Note * The dilutions indicate recommended starting dilutions and the optimal dilutions or concentrations should be determined by the scientist. Positive Control WB: Mouse liver tissue Calculated Mw 29 kDa Properties Form Liquid Purification Affinity purification with immunogen. Buffer PBS (pH 7.3), 0.05% Sodium azide and 50% Glycerol Preservative 0.05% Sodium azide Stabilizer 50% Glycerol Concentration 0.9 mg/ml Storage instruction For continuous use, store undiluted antibody at 2-8°C for up to a week. For long-term storage, aliquot and store at -20°C. Storage in frost free freezers is not recommended. Avoid repeated freeze/thaw cycles. Suggest spin the vial prior to opening. The antibody solution should be gently mixed before use. Note For laboratory research only, not for drug, diagnostic or other use. www.arigobio.com 1/2 Bioinformation Gene Symbol CA1 Gene Full Name carbonic anhydrase I Background Carbonic anhydrases (CAs) are a large family of zinc metalloenzymes that catalyze the reversible hydration of carbon dioxide. -

An Update on the Metabolic Roles of Carbonic Anhydrases in the Model Alga Chlamydomonas Reinhardtii
H OH metabolites OH Review An Update on the Metabolic Roles of Carbonic Anhydrases in the Model Alga Chlamydomonas reinhardtii Ashok Aspatwar 1,* ID , Susanna Haapanen 1 and Seppo Parkkila 1,2 1 Faculty of Medicine and Life Sciences, University of Tampere, FI-33014 Tampere, Finland; [email protected].fi (S.H.); [email protected].fi (S.P.) 2 Fimlab, Ltd., and Tampere University Hospital, FI-33520 Tampere, Finland * Correspondence: [email protected].fi; Tel.: +358-46-596-2117 Received: 11 January 2018; Accepted: 10 March 2018; Published: 13 March 2018 Abstract: Carbonic anhydrases (CAs) are metalloenzymes that are omnipresent in nature. − + CAs catalyze the basic reaction of the reversible hydration of CO2 to HCO3 and H in all living organisms. Photosynthetic organisms contain six evolutionarily different classes of CAs, which are namely: α-CAs, β-CAs, γ-CAs, δ-CAs, ζ-CAs, and θ-CAs. Many of the photosynthetic organisms contain multiple isoforms of each CA family. The model alga Chlamydomonas reinhardtii contains 15 CAs belonging to three different CA gene families. Of these 15 CAs, three belong to the α-CA gene family; nine belong to the β-CA gene family; and three belong to the γ-CA gene family. The multiple copies of the CAs in each gene family may be due to gene duplications within the particular CA gene family. The CAs of Chlamydomonas reinhardtii are localized in different subcellular compartments of this unicellular alga. The presence of a large number of CAs and their diverse subcellular localization within a single cell suggests the importance of these enzymes in the metabolic and biochemical roles they perform in this unicellular alga. -

Neglected Functions of TFCP2/TFCP2L1/UBP1 Transcription Factors May Offer Valuable Insights Into Their Mechanisms of Action
International Journal of Molecular Sciences Review Neglected Functions of TFCP2/TFCP2L1/UBP1 Transcription Factors May Offer Valuable Insights into Their Mechanisms of Action Agnieszka Taracha, Grzegorz Kotarba and Tomasz Wilanowski * Laboratory of Signal Transduction, Nencki Institute of Experimental Biology of Polish Academy of Sciences, 3 Pasteur St., 02-093 Warsaw, Poland; [email protected] (A.T.); [email protected] (G.K.) * Correspondence: [email protected]; Tel.: +48-22-5892-311 Received: 21 August 2018; Accepted: 19 September 2018; Published: 20 September 2018 Abstract: In recent years, the TFCP2 (transcription factor cellular promoter 2)/TFCP2L1 (TFCP2- like 1)/UBP1 (upstream binding protein 1) subfamily of transcription factors has been attracting increasing attention in the scientific community. These factors are very important in cancer, Alzheimer’s disease, and other human conditions, and they can be attractive targets for drug development. However, the interpretation of experimental results is complicated, as in principle, any of these factors could substitute for the lack of another. Thus, studying their hitherto little known functions should enhance our understanding of mechanisms of their functioning, and analogous mechanisms might govern their functioning in medically relevant contexts. For example, there are numerous parallels between placental development and cancer growth; therefore, investigating the roles of TFCP2, TFCP2L1, and UBP1 in the placenta may help us better understand their functioning in cancer, as is evidenced by the studies of various other proteins and pathways. Our review article aims to call the attention of the scientific community to these neglected functions, and encourage further research in this field. -

The Observed Alteration in BCL2 Expression Following Lithium
www.nature.com/scientificreports OPEN The observed alteration in BCL2 expression following lithium treatment is infuenced by the Received: 26 August 2016 Accepted: 26 March 2018 choice of normalization method Published: xx xx xxxx Damri Odeya1,2, Agam Galila1,2 & Toker Lilah3,4 Upregulation of B-cell CLL/lymphoma (BCL)2 expression following lithium treatment is seemingly well established and has been related to the neuroprotective property of the drug. However, while demonstrated by some (but not all) studies based on low-throughput techniques (e.g. qPCR) this efect is not refected in high-throughput studies, such as microarrays and RNAseq. This manuscript presents a systematic review of currently available reports of lithium’s efect on BCL2 expression. To our surprise, we found that the majority of the literature does not support the efect of lithium onBCL 2 transcript or protein levels. Moreover, among the positive reports, several used therapeutically irrelevant lithium doses while others lack statistical power. We also noticed that numerous low-throughput studies normalized the signal using genes/proteins afected by lithium, imposing possible bias. Using wet bench experiments and reanalysis of publicly available microarray data, here we show that the reference gene chosen for normalization critically impacts the outcome of qPCR analyses of lithium’s efect on BCL2 expression. Our fndings suggest that experimental results might be severely afected by the choice of normalizing genes, and emphasize the need to re- evaluate stability of these genes in the context of the specifc experimental conditions. Upregulation of B-cell CLL/lymphoma (BCL)2 transcript following chronic lithium treatment is considered to be well established1. -

Engineered Type 1 Regulatory T Cells Designed for Clinical Use Kill Primary
ARTICLE Acute Myeloid Leukemia Engineered type 1 regulatory T cells designed Ferrata Storti Foundation for clinical use kill primary pediatric acute myeloid leukemia cells Brandon Cieniewicz,1* Molly Javier Uyeda,1,2* Ping (Pauline) Chen,1 Ece Canan Sayitoglu,1 Jeffrey Mao-Hwa Liu,1 Grazia Andolfi,3 Katharine Greenthal,1 Alice Bertaina,1,4 Silvia Gregori,3 Rosa Bacchetta,1,4 Norman James Lacayo,1 Alma-Martina Cepika1,4# and Maria Grazia Roncarolo1,2,4# Haematologica 2021 Volume 106(10):2588-2597 1Department of Pediatrics, Division of Stem Cell Transplantation and Regenerative Medicine, Stanford School of Medicine, Stanford, CA, USA; 2Stanford Institute for Stem Cell Biology and Regenerative Medicine, Stanford School of Medicine, Stanford, CA, USA; 3San Raffaele Telethon Institute for Gene Therapy, Milan, Italy and 4Center for Definitive and Curative Medicine, Stanford School of Medicine, Stanford, CA, USA *BC and MJU contributed equally as co-first authors #AMC and MGR contributed equally as co-senior authors ABSTRACT ype 1 regulatory (Tr1) T cells induced by enforced expression of interleukin-10 (LV-10) are being developed as a novel treatment for Tchemotherapy-resistant myeloid leukemias. In vivo, LV-10 cells do not cause graft-versus-host disease while mediating graft-versus-leukemia effect against adult acute myeloid leukemia (AML). Since pediatric AML (pAML) and adult AML are different on a genetic and epigenetic level, we investigate herein whether LV-10 cells also efficiently kill pAML cells. We show that the majority of primary pAML are killed by LV-10 cells, with different levels of sensitivity to killing. Transcriptionally, pAML sensitive to LV-10 killing expressed a myeloid maturation signature. -

Interventions to Increase Apolipoprotein A-I Transcription in Hepg2 Cells
Interventions to increase apolipoprotein A-I transcription in HepG2 cells Citation for published version (APA): van der Krieken, S. E. (2017). Interventions to increase apolipoprotein A-I transcription in HepG2 cells. Uitgeverij BOXPress. https://doi.org/10.26481/dis.20170330svdk Document status and date: Published: 01/01/2017 DOI: 10.26481/dis.20170330svdk Document Version: Publisher's PDF, also known as Version of record Please check the document version of this publication: • A submitted manuscript is the version of the article upon submission and before peer-review. There can be important differences between the submitted version and the official published version of record. People interested in the research are advised to contact the author for the final version of the publication, or visit the DOI to the publisher's website. • The final author version and the galley proof are versions of the publication after peer review. • The final published version features the final layout of the paper including the volume, issue and page numbers. Link to publication General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal.