Year 3 Quarter 2 Progress Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

IGREJA METODISTA UNIDA Conferência Anual Do Oeste De Angola 32ª Sessão – 11 a 15 De Janeiro De 2017
IGREJA METODISTA UNIDA Conferência Anual do Oeste de Angola 32ª Sessão – 11 a 15 de Janeiro de 2017 PROCEDIMENTOS DIÁRIOS ACTA Nº 1 Quarta-feira, 11 de Janeiro de 2017 CULTO SOLENE DE ABERTURA: A Sessão Solene de Abertura da 32ª Sessão da Conferência Anual decorreu no Pavilhão Gimno-Desportivo de Ndalatando, com início às 9:15 minutos. Foi liturgista o Rev. Marcos Francisco de Almeida- Superintendente do Distrito Eclesiástico de Cuanza-Norte, que acolhe esta Sessão Conferencial, que este ano tem como tema “Povo Metodista: Portas Abertas, Corações Abertos e Mentes Abertas”, baseado em S. Lucas 10:25-37. Entoado o hino em Português 6, foi feita uma chamada de adoração em S. Lucas 10:37, seguindo-se a récita do Credo Apostólico, uma oração feita pelo Rev. Moisés Jungo-Superintendente do Distrito Eclesiástico de Cuanza-Sul bem como a leitura responsiva do Salmo 24. Foram feitas duas orações: uma pela irmã Florinda António, Guia Leiga da Igreja Metodista Unida Central de Luanda e outra pelo Guia Leigo do Distrito Eclesiástico de Cuanza-norte. MOMENTO PROTOCOLAR: O Superintendente do Distrito Eclesiástico de Cuanza- Norte, que acolhe a presente Sessão desejou aos Revmos. Bispos e suas esposas, aos Superintendentes de distrito, delegados clérigos e leigos, boas vindas ao seu Distrito, que acolhe pela segunda vez a Sessão da Conferência Anual nos tempos de paz. De seguida, Sua Revma. Bispo Gaspar João Domingos apresentou Sua Excelência o Governador da Província do Cuanza Norte a quem agradeceu por ter aberto as portas que esta Sessão acontecesse na sua Província, transformando-a, esta semana, na Jerusalém da Igreja Metodista Unida, Conferência Anual do Oeste de Angola. -

Inventário Florestal Nacional, Guia De Campo Para Recolha De Dados
Monitorização e Avaliação de Recursos Florestais Nacionais de Angola Inventário Florestal Nacional Guia de campo para recolha de dados . NFMA Working Paper No 41/P– Rome, Luanda 2009 Monitorização e Avaliação de Recursos Florestais Nacionais As florestas são essenciais para o bem-estar da humanidade. Constitui as fundações para a vida sobre a terra através de funções ecológicas, a regulação do clima e recursos hídricos e servem como habitat para plantas e animais. As florestas também fornecem uma vasta gama de bens essenciais, tais como madeira, comida, forragem, medicamentos e também, oportunidades para lazer, renovação espiritual e outros serviços. Hoje em dia, as florestas sofrem pressões devido ao aumento de procura de produtos e serviços com base na terra, o que resulta frequentemente na degradação ou transformação da floresta em formas insustentáveis de utilização da terra. Quando as florestas são perdidas ou severamente degradadas. A sua capacidade de funcionar como reguladores do ambiente também se perde. O resultado é o aumento de perigo de inundações e erosão, a redução na fertilidade do solo e o desaparecimento de plantas e animais. Como resultado, o fornecimento sustentável de bens e serviços das florestas é posto em perigo. Como resposta do aumento de procura de informações fiáveis sobre os recursos de florestas e árvores tanto ao nível nacional como Internacional l, a FAO iniciou uma actividade para dar apoio à monitorização e avaliação de recursos florestais nationais (MANF). O apoio à MANF inclui uma abordagem harmonizada da MANF, a gestão de informação, sistemas de notificação de dados e o apoio à análise do impacto das políticas no processo nacional de tomada de decisão. -

Mapa Rodoviario Angola
ANGOLA REPÚBLICA DE ANGOLA MINISTÉRIO DAS FINANÇAS FUNDO RODOVIÁRIO Miconje ANGOLA Luali EN 220 Buco Zau Belize Inhuca Massabi EN 220 Necuto Dinge O Chicamba ANG LU O EN 101 EN 100 I R CABINDA Bitchequete Cacongo Zenza de Lucala Malembo Fubo EN 100 EN 201 CABINDA Cabassango Noqui Luvo Pedra do Buela EN 210 Feitiço EN 120 EN 210 Sacandica Lulendo Maquela Sumba ZAIRE Cuimba do Zombo Icoca Soyo Béu EN 160 Cuango Lufico M´BANZA Quimbocolo Canda Cuilo Futa Quiende CONGO EN 140 Quimbele Quielo Camboso EN 210 Mandimba Sacamo Camatambo Quincombe Fronteira EN 120 Damba Quiximba Lucunga Lemboa Buengas Santa Tomboco 31 de Janeiro Quinzau EN 160 RIO BRIDG Cruz M E Quimbianda Uambo EN 100 Bessa Bembe Zenguele UIGE Macocola Macolo Monteiro Cuilo Pombo N´Zeto EN 120 Massau Tchitato Mabaia Mucaba Sanza Uamba EN 223 E EN 223 OG O L EN 140 Quibala Norte RI Songo Pombo Lovua Ambuíla Bungo Alfândega DUNDO EN 220 EN 220 Quinguengue EN 223 Musserra UÍGE Puri EN 180 Canzar Desvio do Cagido Caiongo Quihuhu Cambulo Quipedro EN 120 Negage EN 160 Zala Entre os Rios Ambriz Bela Dange EN 220 Vista Gombe Quixico Aldeia Quisseque Cangola EN 140 Mangando EN 225 EN 100 MuxaluandoViçosa Bindo Massango BENGO Tango MALANGE Camissombo Luia Canacassala Cambamba Bengo EN 165 Caluango Tabi Quicunzo Cabombo Cuilo Quicabo Vista Quiquiemba Camabatela Cuale EN 225 Ramal da Barra Cage Alegre Maua Caungula Camaxilo Capaia Cachimo DANDE do Dande Libongos O RI S. J.das Terreiro EN 225 Barra do BolongongoLuinga Marimba Luremo Quibaxe Matas Cateco Micanda Lucapa Dande Mabubas EN 225 -

United Nations Office for the Coordination of Humanitarian Affairs (Ocha)
UNITED NATIONS OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS (OCHA) HUMANITARIAN SITUATION IN ANGOLA Situation Report Reporting Period: 1 – 15 September 2003 Critical Issues q Fourteen deminers were injured when an anti-tank mine exploded on the Cambaxe – Malanje road in Malanje Municipality. q A meningitis outbreak has been confirmed in Huíla Province and a significant number of cases have been reported in Malanje Province. q Due to the start of the rainy season, humanitarian partners were not able to transport more seeds and tool kits to the interior of Kuanza Sul Province. q A donation of seeds and tools for 8,000 beneficiaries in Lunda Sul was cancelled due to lack of a partner to carry out the distribution. q Most of the seeds and tools for distribution in Moxico Province have yet to arrive. Provincial Update Luanda Province: The Provincial Government transported 2,030 people to Malanje. They are staying in the Katepa transit centre where they are sleeping in the open air and have no access to food, water, sanitation and health assistance. According to provincial authorities, one person died on arrival and no transportation is available for onward travel to areas of origin. Benguela Province: During the reporting period, local authorities closed the Benguela transit centre located in a former military quartering camp and moved the 250 people to the new Capiandalo transit centre approximately five km outside the city centre. An additional 108 demobilised soldiers and their dependents arrived from the former Menga gathering area in Huambo and humanitarian partners report that the people in the new camp are living in substandard conditions. -

Zoneamento Agroclimático Para Cultura Do Café Em Angola
ARISTIDES OSVALDO NGOLO ZONEAMENTO AGROCLIMÁTICO PARA CULTURA DO CAFÉ EM ANGOLA Dissertação apresentada à Universidade Federal de Viçosa, como parte das exigências do Programa de Pós-Graduação em Agroecologia, para obtenção do título de Magister Scientiae. VIÇOSA MINAS GERAIS – BRASIL 2014 Índice Lista de figuras v Lista de tabelas vii Resumo viii Abstract ix 1. Introdução 1 2. Revisão de literatura 4 2.1 Caracterização geral das condições físicas do território de Angola 4 2.1.1 Relevo de Angola 5 2.1.2 Clima de Angola 5 2.1.3 Solos de Angola 7 2.2 Contexto histórico da cafeicultura em Angola 9 2.3 A cultura do cafeeiro 12 2.3.1 Fenologia do cafeeiro 15 2.4 Balanço hídrico climatológico 16 2.5 Precipitação pluviométrica efetiva 18 2.6 Zoneamento agrícola 20 2.7 Aptidões pedológica e agroclimática para o café arábica e robusta 21 2.7.1 Aptidão pedológica para café arábica e robusta 21 2.7.1.1 Características físicas do solo 22 2.7.1.2 Características químicas do solo 23 2.7.2 Aptidões agroclimática para o café arábica e robusta 24 3. Material e Métodos 27 3.1 Dados climáticos 28 3.1.1 Obtenção dos dados de temperatura e precipitação no site do WorldClim 31 3.1.2 Obtenção do Modelo Digital de Elevação 31 3.2 Estimativa da precipitação efetiva 32 3.3 Estimativa da deficiência hídrica 32 3.4 Aptidão Agroclimática 34 3.5 Elaboração do Zoneamento Agroclimático 38 4. Resultados e Discussão 40 4.1 Zoneamento para o café em Angola com base na precipitação efetiva 48 4.2 Zoneamento para o café em Angola com base na precipitação total 53 5. -

(HFA) Population Services International (PSI) RFA-654-16-000004 Cooperative Agreement No.: AID-654-A-17-00003
Health for All (HFA) Population Services International (PSI) RFA-654-16-000004 Cooperative Agreement No.: AID-654-A-17-00003 Quarterly Report 3: April 1st to June 30th, 2017 1 HEALTH FOR ALL In January 2017, the Population Services International-led Consortium was awarded RFA-654- 16-000004 to implement the project Health for All (HFA), from FY17-FY21. HFA’s program goal is to have USAID Angola partnerships transformed to strengthen the effective use of Angola's resources to meet the country’s development needs. HFA includes three health areas: malaria, HIV and family planning. This Quarterly Report refers to activities implemented between April and June 2017 (Q3): Result 1: LLIN Access and Use Increased by at least 30%. Key Results Expected ● Distribution of 2.9 million mosquito nets in 5 provinces ● LLIN related Social Behavior Change Communication strategy updated and adopted by NMCP and HFA ● 4,000 “activitas” or community agents trained in communication during distribution USAID/PMI supports a pillar of the National Malaria Control Program’s (NMCP) strategic plan: LLIN distribution for universal coverage in Angola. NMCP updated its approach to LLIN distribution and now aims to achieve universal coverage through a national distribution campaign to provide LLIN for all provinces within a year. LLIN Distribution HFA led a national Mass Distribution of LLINS (long lasting insecticide treated nets) during FY 17 in the following provinces (phase 1): • Cuanza Sul • Cuanza Norte • Zaire • Malanje • Uige (Quitexe, Cangola, Sanza Pompo, Puri, Buengas and Mucapa municipalities) This quarter was marked by the implementation of LLIN Distribution activities in all municipalities, following the novel distribution strategy adopted by NMCP. -

Boletim Informativo Consulado Geral Da República De Angola | Região Administrativa Especial De Macau | República Popular Da China
No39 16-30 Setembro 2009 Boletim Informativo Consulado Geral da República de Angola | Região Administrativa Especial de Macau | República Popular da China ACTIVIDADE PRESIDENCIAL Chefe de Estado analisa funcionamento da Comissão do Golfo da Guiné LUANDA Chefe de Estado angolano, José Eduardo dos Santos, analisou, O terça-feira (22), em Luanda, com o Secretário-Executivo da Comissão do Golfo da Guiné (CGG), Miguel Trovoada, o funcionamento da organização durante os últimos oito meses. “Foi um relatório daquilo que nós fi zemos e das perspectivas imediatas”, disse Miguel Trovoada à imprensa no fi nal da audiência a si concedida pelo igualmente presidente da CGG. No seu entender, estas perspectivas “passam por uma maior coordenação entre o Secretariado e a Presidência, bem como na preparação dos próximos encontros que irão definir os passos a dar ao longo dos dois anos”. Segundo informou, o organismo deverá reunir em Outubro próximo para abordar aspectos ligados a estabilidade e a segurança, sem no entanto apontar o local, a fi m de se colmatar a fracassada reunião que deveria ter lugar em São Tomé e Príncipe. “O orçamento da organização, estimado em quatro milhões de dólares, quando for pago por todos os estados membros, contribuirá para o normal funcionamento do organismo”, referiu. Angola, enquanto país sede da comissão, referiu, tem concedido apoios fi nanceiros que garantem a sua sobrevivência. Criada em 1999 a CGG é integrada por Angola, Congo Democrático, República do Congo, Nigéria, São Tomé e Príncipe, Gabão, Camarões e Guiné Equatorial. CG/Angolapress ACTIVIDADE PRESIDENCIAL PR recebe garantias da disponibilidade do Banco Espírito Santo LUANDA vamos continuar acrescer e tem tido bons resultados”, disse. -
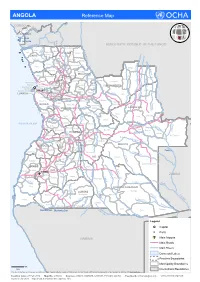
ANGOLA Reference Map
ANGOLA Reference Map CONGO L Belize ua ng Buco Zau o CABINDA Landana Lac Nieba u l Lac Vundu i Cabinda w Congo K DEMOCRATIC REPUBLIC OF THE CONGO o z Maquela do Zombo o p Noqui e Kuimba C Soyo M Mbanza UÍGE Kimbele u -Kongo a n ZAIRE e Damba g g o id Tomboco br Buengas M Milunga I n Songo k a Bembe i C p Mucaba s Sanza Pombo a i a u L Nzeto c u a i L l Chitato b Uige Bungo e h o e d C m Ambuila g e Puri Massango b Negage o MALANGE L Ambriz Kangola o u Nambuangongo b a n Kambulo Kitexe C Ambaca m Marimba g a Kuilo Lukapa h u Kuango i Kalandula C Dande Bolongongo Kaungula e u Sambizanga Dembos Kiculungo Kunda- m Maianga Rangel b Cacuaco Bula-Atumba Banga Kahombo ia-Baze LUNDA NORTE e Kilamba Kiaxi o o Cazenga eng Samba d Ingombota B Ngonguembo Kiuaba n Pango- -Caju a Saurimo Barra Do Cuanza LuanCda u u Golungo-Alto -Nzoji Viana a Kela L Samba Aluquem Lukala Lul o LUANDA nz o Lubalo a Kazengo Kakuso m i Kambambe Malanje h Icolo e Bengo Mukari c a KWANZA-NORTE Xa-Muteba u Kissama Kangandala L Kapenda- L Libolo u BENGO Mussende Kamulemba e L m onga Kambundi- ando b KWANZA-SUL Lu Katembo LUNDA SUL e Kilenda Lukembo Porto Amboim C Kakolo u Amboim Kibala t Mukonda Cu a Dala Luau v t o o Ebo Kirima Konda Ca s Z ATLANTIC OCEAN Waco Kungo Andulo ai Nharea Kamanongue C a Seles hif m um b Sumbe Bailundo Mungo ag e Leua a z Kassongue Kuemba Kameia i C u HUAMBO Kunhinga Luena vo Luakano Lobito Bocoio Londuimbali Katabola Alto Zambeze Moxico Balombo Kachiungo Lun bela gue-B Catum Ekunha Chinguar Kuito Kamakupa ungo a Benguela Chinjenje z Huambo n MOXICO -

Dossier De Habitação Janeiro - Dez 2016
Dossier de Habitação Janeiro - Dez 2016 Grato pela atenção. A Redação O Extracto de notícias é um serviço do Centro de Redação Documentação da DW (CEDOC) situado nas instalações Conselho de Ediçao da DW em Luanda. O Centro foi criado em Janeiro de Allan Cain, João Domingos, Sobriano César Capit-ao e 2001 com o objectivo de facilitar a recolha, Massomba Dominique armazenamento, acesso e disseminação de informação sobre desenvolvimento socio-economico do País. Editado por Development Workshop Angola Através da monitoria dos projectos da DW, estudos, pesquisas e outras formas de recolha de informação, o Endereço Centro armazena uma quantidade considerável de documentos entre relatórios, artigos, mapas e livros. A Rua Rei Katyavala 113, informação é arquivada física e eletronicamente, e está C. P. 3360, Luanda — Angola disponível para consulta para as entidades interessadas. Além da recolha e armazenamento de informação, o Telefone +(244 2) 448371 / 77 / 66 Centro tem a missão da disseminação de informação por vários meios. Um dos produtos principais do Centro é o Email cedoc. dwang@angonet. Org Extracto de notícias. Este Jornal monitora a imprensa nacional e extrai artigos de interesse para os leitores com Com apoio de actividades de interesse no âmbito do desenvolvimento do Development Workshop País. O jornal traz artigos categorizados nos seguintes OXFAM Novib grupos principais. Fundação Bill & Melinda Gates International Development Research Centre 1. Redução da Pobreza e Economia Civil Society Challenge Fund 2. Microfinanças Norwegian & The Netherlands Embassies 3. Mercado Informal European Union 4. OGE investimens públicos e transparência Dislaimer 5. Governação descentralização e cidadania 1. Content 6. -

E2146 V2 Public Disclosure Authorized Public Disclosure Authorized
Angola’s National Health Care Waste Management Plan E2146 V2 Public Disclosure Authorized Public Disclosure Authorized AANNGGOOLLAA’’SS NNAATTIIOONNAALL HHEEAALLTTHH CCAARREE WWAASSTTEE MMAANNAAGGEEMMEENNTT PPLLAANN PPrreeppaarreedduunnddeerr ttthheeHHAAMMSSEETTpprroojjjeeccttt Public Disclosure Authorized UUppddaattteedduunnddeerrrttthheeMMHHSSSS PPrroojjjeeccttt EENNVVIIRROONNMMEENNTTAALL AANNDD SSOOCCIIAALL SSCCRREEEENNIINNGG AANNDD AASSSSEESSSSMMEENNTT FFRRAAMMEEWWOORRKK November 19, 2009 CONSULTANT : Public Disclosure Authorized ENGINEER ADÉRITO DE CASTRO VIDE LUANDA –NOVEMBER 2004 – Updated March 2009. 1/83 Angola’s National Health Care Waste Management Plan INDEX List of Acronyms and Abbreviations List of Tables List of Figures Executive Summary 1. Introduction 2. Country’s Presentation 2.1. Geographical Data and Administrative Division 2.2. Demographic Data and Health Statistics 2.2.1. Population Distribution and Evolution 2.2.2. Health Statistics 2.3. Legal and Political Frame 2.3.1. Health and Environmental Policies 2.3.2. National Health Care System Organization 2.3.3. Health Care Establishments Distribution 3. Health Care Waste Management in Angola: Assessment on the Current Situation 3.1. Existing Practices 3.2. Brief SWOT Analysis 3.2.1. Vector A - Strengths 3.2.2. Vector B - Weaknesses 3.2.3. Vector C - Opportunities 3.2.4. Vector D - Threats 3.2.5. Crossed Analysis 3.2.6. Conclusion 3.3. Estimate of Health Care Waste Generation in Angola 4. Implementing Strategy of the HCWM Plan 4.1. Strategic Vector 1: Reinforce Institutional, Legislative and Regulation frame 4.1.1. Introduction 4.1.2. International Agreements, Legislation and Related Principles 4.1.3. Legal Provisions 4.1.4. Policy Documents and Technical Guidelines 4.1.5. Foreseen Actions 4.2. Strategic Vector 2: Planning and Managing 4.2.1. -

Ssabe Sub Sahara Africa Built
SSABE SUB SAHARA AFRICA BUILT ENVIRONMENT INTERNATIONALLY ACCLAIMED FACILITY From the Desk of Paul S Rogers +27 (0)83 520 7596 E: [email protected] Issue 273- 29, 2012 SSABE CONNECTS YOU with Sub Sahara Africa at no cost, - it is a free service for all built environment suppliers and contractors. No registration, just a get-down-to-basics Internationally Acclaimed service. Just send your eddress and request to [email protected] SSABE PRODUCES - A weekly international tender and news collation of matters relating to the built environment. An easy scrolling ‘.PDF FORMAT NEWSLETTER’ in country alphabetical order divided into the key trade blocs. The articles covered in these weekly updates will provide you with the leads you need to follow up on early warning prospects. Most have names and companies for you to record. Should you target an individual country before a trade visit, scanning the relevant collations will give you a myriad of prospective appointments in business development. TENDERS SSABE TENDER NOTICES – Provides you with the full tender notice of the abridged version in the newsletter at a nominal fee [US$20 / ZAR150] – Just send request and the interested bid reference to [email protected] (A few notices will not be available and ‘Prior Information’ is posted 30 days or more before bid opening) AFRICA: Tender - Fixed Wing STOL Aircraft in Africa Opportunity Type: Goods Express Interest By: Aug 22, 2012 Project Summary - fixed wing STOL aircraft to be used in support of peace-keeping -

Angola Livelihood Zone Report
ANGOLA Livelihood Zones and Descriptions November 2013 ANGOLA Livelihood Zones and Descriptions November 2013 TABLE OF CONTENTS Acknowledgements…………………………………………………………………………................……….…........……...3 Acronyms and Abbreviations……….………………………………………………………………......…………………....4 Introduction………….…………………………………………………………………………………………......………..5 Livelihood Zoning and Description Methodology……..……………………....………………………......…….…………..5 Livelihoods in Rural Angola….………........………………………………………………………….......……....…………..7 Recent Events Affecting Food Security and Livelihoods………………………...………………………..…….....………..9 Coastal Fishing Horticulture and Non-Farm Income Zone (Livelihood Zone 01)…………….………..…....…………...10 Transitional Banana and Pineapple Farming Zone (Livelihood Zone 02)……….……………………….….....…………..14 Southern Livestock Millet and Sorghum Zone (Livelihood Zone 03)………….………………………….....……..……..17 Sub Humid Livestock and Maize (Livelihood Zone 04)…………………………………...………………………..……..20 Mid-Eastern Cassava and Forest (Livelihood Zone 05)………………..……………………………………….……..…..23 Central Highlands Potato and Vegetable (Livelihood Zone 06)..……………………………………………….………..26 Central Hihghlands Maize and Beans (Livelihood Zone 07)..………..…………………………………………….……..29 Transitional Lowland Maize Cassava and Beans (Livelihood Zone 08)......……………………...………………………..32 Tropical Forest Cassava Banana and Coffee (Livelihood Zone 09)……......……………………………………………..35 Savannah Forest and Market Orientated Cassava (Livelihood Zone 10)…….....………………………………………..38 Savannah Forest and Subsistence Cassava