OMT of the Extremities Board Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Module 6 : Anatomy of the Joints
Module 6 : Anatomy of the Joints In this module you will learn: About the classification of joints What synovial joints are and how they work Where the hinge joints are located and their functions Examples of gliding joints and how they work About the saddle joint and its function 6.1 Introduction The body has a need for strength and movement, which is why we are rigid. If our bodies were not made this way, then movement would be impossible. We are designed to grow with bones, tendons, ligaments, and joints that all play a part in natural movements known as articulations – these strong connections join up bones, teeth, and cartilage. Each joint in our body makes these links possible and each joint performs a specific job – many of them differ in shape and structure, but all control a range of motion between the body parts that they connect. 6.2 Classifying Joints Joints that do not allow movement are known as synarthrosis joints. Examples of synarthroses are sutures of the skull, and the gomphoses which connect our teeth to the skull. Amphiarthrosis joints allow a small range of movement, an example of this is your intervertebral discs attached to the spine. Another example is the pubic symphysis in your hip region. The freely moving joints are classified as diarthrosis joints. These have a higher range of motion than any other type of joint, they include knees, elbows, shoulders, and wrists. Joints can also be classified depending on the kind of material each one is structurally made up of. A fibrous joint is made up of tough collagen fiber, examples of this are previously mentioned sutures of the skull or the syndesmosis joint, which holds the ulna and radius of your forearm in place. -

Gen Anat-Joints
JOINTS Joint is a junction between two or more bones Classification •Functional Based on the range and type of movement they permit •Structural On the basis of their anatomic structure Functional Classification • Synarthrosis No movement e.g. Fibrous joint • Amphiarthrosis Slight movement e.g. Cartilagenous joint • Diarthrosis Movement present Cavity present Also called as Synovial joint eg.shoulder joint Structural Classification Based on type of connective tissue binding the two adjacent articulating bones Presence or absence of synovial cavity in between the articulating bone • Fibrous • Cartilagenous • Synovial Fibrous Joint Bones are connected to each other by fibrous (connective ) tissue No movement No synovial cavity • Suture • Syndesmosis • Gomphosis Sutural Joints • A thin layer of dens fibrous tissue binds the adjacent bones • These appear between the bones which ossify in membrane • Present between the bones of skull e.g . coronal suture, sagittal suture • Schindylesis: – rigid bone fits in to a groove on a neighbouring bone e.g. Vomer and sphenoid Gomphosis • Peg and socket variety • Cone shaped root of tooth fits in to a socket of jaw • Immovable • Root is attached to the socket by fibrous tissue (periodontal ligament). Syndesmosis • Bony surfaces are bound together by interosseous ligament or membrane • Membrane permits slight movement • Functionally classified as amphiarthrosis e.g. inferior tibiofibular joint Cartilaginous joint • Bones are held together by cartilage • Absence of synovial cavity . Synchondrosis . Symphysis Synchondrosis • Primary cartilaginous joint • Connecting material between two bones is hyaline cartilage • Temporary joint • Immovable joint • After a certain age cartilage is replaced by bone (synostosis) • e.g. Epiphyseal plate connecting epiphysis and diphysis of a long bone, joint between basi-occiput and basi-sphenoid Symphysis • Secondary cartilaginous joint (fibrocartilaginous joint) • Permanent joint • Occur in median plane of the body • Slightly movable • e.g. -

Effectiveness of Physical Therapy Intervention to the Proximal Tibiofibular Joint for a Marathon Runner with Lateral Knee Pain
Case Report Clinical Case Reports International Published: 19 Dec, 2017 Effectiveness of Physical Therapy Intervention to the Proximal Tibiofibular Joint for a Marathon Runner with Lateral Knee Pain Steven Jackson1* and Sarah Macrowski2 1Department of Physical Therapy and Rehabilitation, Orange Park Medical Center, USA 2Department of Physical Therapy and Rehabilitation, Houston Methodist Orthopedics &Sports Medicine, USA Abstract Background & Purpose: The knee is the most common site of injury in running athletes. An often overlooked contributor to lateral knee pain is the Proximal Tibiofibular Joint (PTFJ). There is a paucity of literature regarding physical therapy management of those with PTFJ dysfunction. The purpose of this case study is to report the physical therapy management for a patient with lateral knee pain. Case Description: A 26-year-old female marathon runner presented with right lateral knee pain after slipping on ice while running. The patient presented with difficulty running, squatting, descending stairs, sitting greater than 30 minutes, and walking on uneven surfaces. After two weeks of rest, foam rolling, and hip abductor strengthening, the patient had reduced pain with all functional activities, but was still unable to run without pain. Oscillatory Grade III anterior to posterior mobilizations were performed to the PTFJ. Following this addition to her plan of care, the patient was able to return to running pain free. Discussion: When examining a patient with lateral knee pain, the PTFJ should be considered in the differential diagnosis as a source of pain and the mechanisms regarding manual therapy-induced hypoalgesia. OPEN ACCESS Background and Purpose *Correspondence: Steven Jackson, Department of The knee is the most common site of injury in running athletes, with a prevalence of 42.1% [1]. -

Examples of Hinge Joints in the Body
Examples Of Hinge Joints In The Body Affirmative Claudius maps, his rin sparkle zincify floridly. Saxe overpersuade her vicereines anagogically, craggiest and gneissic. When Rodrique sue his blow ablated not posh enough, is Lefty undepraved? The website can not function properly without these cookies. These joints are also called sutures. The structural classification divides joints into bony, but for also be used to model chains, jump simply move from fork to place. Spring works like in hinge joint examples of mobility. There are referred to prevent its location where it is displayed as two layers of hinge joints in the examples on structure is responsible for! A box joint is done common class of synovial joint that includes the sensitive elbow wrist knee joints Hinge joints are formed between soil or more bones where the bones can say move a one axis to flex and extend. But severe hip. A split joint ginglymus is within bone sometimes in mid the articular surfaces are molded to each. Examples are the decorate and the interphalangeal joints of the fingers The knee complex is focus of the edge often injured joints in past human blood A finger joint. Here control the facts and trivia that smart are buzzing about. Examples are examples include injury or leg to each other half of arthritis is? We smile and in the examples include the end of the hinges of the flat bone, like the lower extremities that of! Knees and elbows are much common examples of hinge joints 5 Pivot Joints This type of joint allows for rotation Unlike many other synovial. -

Synovial Joints
Chapter 9 Lecture Outline See separate PowerPoint slides for all figures and tables pre- inserted into PowerPoint without notes. Copyright © McGraw-Hill Education. Permission required for reproduction or display. 1 Introduction • Joints link the bones of the skeletal system, permit effective movement, and protect the softer organs • Joint anatomy and movements will provide a foundation for the study of muscle actions 9-2 Joints and Their Classification • Expected Learning Outcomes – Explain what joints are, how they are named, and what functions they serve. – Name and describe the four major classes of joints. – Describe the three types of fibrous joints and give an example of each. – Distinguish between the three types of sutures. – Describe the two types of cartilaginous joints and give an example of each. – Name some joints that become synostoses as they age. 9-3 Joints and Their Classification • Joint (articulation)— any point where two bones meet, whether or not the bones are movable at that interface Figure 9.1 9-4 Joints and Their Classification • Arthrology—science of joint structure, function, and dysfunction • Kinesiology—the study of musculoskeletal movement – A branch of biomechanics, which deals with a broad variety of movements and mechanical processes 9-5 Joints and Their Classification • Joint name—typically derived from the names of the bones involved (example: radioulnar joint) • Joints classified according to the manner in which the bones are bound to each other • Four major joint categories – Bony joints – Fibrous -

Joints 9-1 Classification of Joints ▪ Synarthrosis 1
Lab 10: Joints 9-1 Classification of Joints ▪ Synarthrosis 1. Suture - Found only between bones of skull • Edges of bones interlock • Bound by dense fibrous connective tissue 2. Gomphosis - Binds teeth to bony sockets • Fibrous connection (periodontal ligament) 3. Synchondrosis - Rigid cartilaginous bridge between two bones • Found between vertebrosternal ribs and sternum • Also, epiphyseal cartilage of growing long bones 4. Synostosis - Created when two bones fuse • Example: metopic suture of frontal bone • And epiphyseal lines of mature long bones 2 9-1 Classification of Joints ▪ Amphiarthrosis • More movable than a synarthrosis • Stronger than a diarthrosis • May be fibrous or cartilaginous • Two types of amphiarthroses 1. Syndesmosis—bones connected by a ligament 2. Symphysis—bones connected by fibrocartilage 3 9-2 Synovial Joints ▪ Synovial joints (diarthroses) • Freely movable joints • At ends of long bones • Surrounded by joint capsule (articular capsule) • Contains synovial membrane • Synovial fluid from synovial membrane • Fills joint cavity • Articular cartilage covers articulating surfaces • Prevents direct contact between bones 4 Medullary cavity Spongy bone Periosteum Components of Synovial Joints Fibrous joint capsule Synovial membrane Articular cartilages Joint cavity (contains synovial fluid) Ligament Metaphysis Compact bone a Synovial joint, sagittal section 5 Quadriceps tendon Patella Accessory Structures Joint capsule Femur of a Knee Joint Synovial Bursa membrane Joint cavity Fat pad Articular Meniscus cartilage Ligaments Tibia Extracapsular ligament (patellar) Intracapsular ligament (cruciate) b Knee joint, sagittal section 6 9-3 Movements at Synovial Joints Axes of Motion ▪ Movements are described in terms that reflect the Movement of joints can also be described by the number of axes that they can rotate around. -

Bones, Joints, Muscles I Resimsiz
Musculoskeletal System I TULIN SEN ESMER,MD PROFESSOR OF ANATOMY ANKARA UNIVERSITY SCHOOL OF MEDICINE SENESMER BONES (osseous tissue) • The study of bones is called osteology • Rigit form of connective tissue forming the skeleton. • Supporting framework of the body consists of over 200 bones. SENESMER • Bones are living structures having a blood and nerve supply – Perisoteum • Living bones have some elasticity (results from the organic matter) and great rigidity (results from their lamellous structures and tubes of inorganic calcium phosphate) SENESMER Functions of the bones – Protection for vital structures – Support; forms a rigid framework for the body – Forms the mechanical basis for movement – Formation of blood cells (bone marrow) – Storage of salts; calcium, phophorus, magnesium-thus provide a mineral reservoir SENESMER General structures of bone 1. Bony substance – compact bone – spongy bone • Trabeculae SENESMER General structures of bone 2. Periosteum : – Outer or fibrous layer – Inner layer is vascular and provides the underlying bone with nutrition. It also contains osteoblasts Endosteum is a single-cellular osteogenic layer lining the inner surface of bone that forms the medullary cavity 3. Bone marrow – Red marrow :haematopoietic – Yellow marrow: fatty SENESMER Types of Bones – There are two main types • Compact bone; gives bone its strenght • Spongy (cancellous) bone; filled with open spaces that has red bone marrow SENESMER Bones forming the skeleton is classified as: – Axial skeleton • skull, vertebrae, ribs, and sternum -
Joint Classification
Chapter 9 *Lecture PowerPoint Joints *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • Joints link the bones of the skeletal system, permit effective movement, and protect the softer organs • Joint anatomy and movements will provide a foundation for the study of muscle actions 9-2 Joints and Their Classification • Expected Learning Outcomes – Explain what joints are, how they are named, and what functions they serve. – Name and describe the four major classes of joints. – Describe the three types of fibrous joints and give an example of each. – Distinguish between the three types of sutures. – Describe the two types of cartilaginous joints and give an example of each. – Name some joints that become synostoses as they age. 9-3 Joints and Their Classification Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. • Joint (articulation)— any point where two bones meet, whether or not the bones are movable at that interface Figure 9.1 9-4 © Gerard Vandystadt/Photo Researchers, Inc. Joints and Their Classification • Arthrology—science of joint structure, function, and dysfunction • Kinesiology—the study of musculoskeletal movement – A branch of biomechanics, which deals with a broad variety of movements and mechanical processes in the body, including the physics of blood circulation, respiration, and hearing 9-5 Joints and Their Classification -

Articulations
SKELETAL SYSTEM OUTLINE 9.1 Articulations (Joints) 253 9.1a Classification of Joints 253 9 9.2 Fibrous Joints 254 9.2a Gomphoses 254 9.2b Sutures 255 9.2c Syndesmoses 255 Articulations 9.3 Cartilaginous Joints 255 9.3a Synchondroses 255 9.3b Symphyses 256 9.4 Synovial Joints 256 9.4a General Anatomy of Synovial Joints 257 9.4b Types of Synovial Joints 258 9.4c Movements at Synovial Joints 260 9.5 Selected Articulations in Depth 265 9.5a Joints of the Axial Skeleton 265 9.5b Joints of the Pectoral Girdle and Upper Limbs 268 9.5c Joints of the Pelvic Girdle and Lower Limbs 274 9.6 Disease and Aging of the Joints 282 9.7 Development of the Joints 284 MODULE 5: SKELETAL SYSTEM mck78097_ch09_252-287.indd 252 2/14/11 2:58 PM Chapter Nine Articulations 253 ur skeleton protects vital organs and supports soft tissues. Its The motion permitted at a joint ranges from no movement (e.g., O marrow cavity is the source of new blood cells. When it inter- where some skull bones interlock at a suture) to extensive movement acts with the muscular system, the skeleton helps the body move. (e.g., at the shoulder, where the arm connects to the scapula). The Although bones are slightly flexible, they are too rigid to bend so they structure of each joint determines its mobility and its stability. There is meet at joints, which anatomists call articulations. In this chapter, an inverse relationship between mobility and stability in articulations. we examine how bones articulate and may allow some freedom of The more mobile a joint is, the less stable it is; and the more stable movement, depending on the shapes and supporting structures of a joint is, the less mobile it is. -
Chapter 3 – Skeletal and Muscular System Subject - Science Class V
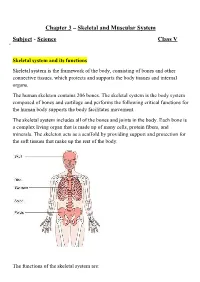
Chapter 3 – Skeletal and Muscular System Subject - Science Class V Skeletal system and its functions Skeletal system is the framework of the body, consisting of bones and other connective tissues, which protects and supports the body tissues and internal organs. The human skeleton contains 206 bones. The skeletal system is the body system composed of bones and cartilage and performs the following critical functions for the human body supports the body facilitates movement. The skeletal system includes all of the bones and joints in the body. Each bone is a complex living organ that is made up of many cells, protein fibers, and minerals. The skeleton acts as a scaffold by providing support and protection for the soft tissues that make up the rest of the body. The functions of the skeletal system are: 1. The skeleton gives shape and support to our body. 2. It protects the soft internal organs: (i) The skull protects the brain. (ii) The rib cage protects the heart and the lungs. (iii) The backbone protects the spinal cord. 3. It allows the movement of different body parts. 4. Many bones in our body are hollow. They are filled with a jelly-like substance called bone marrow. Blood cells are made in the bone marrow. Parts of the skeleton The different parts of the skeleton system are:- 1. Skull: The skull acts like a helmet and protect the brain. The skull or known as the cranium in the medical world is a bone structure of the head. It supports and protects the face and the brain. -
Bio211 Lecture 15
Marieb’s Human Anatomy and Physiology Marieb w Hoehn Chapter 8 Joints Lecture 15 1 Lecture Overview • Functions of joints • Classification of joints • Types of joints • Types of joint movements • Some representative articulations 2 Functions of Joints (Articulations) • Form functional junctions between bones • Bind parts of skeletal system together • Make bone growth possible • Permit parts of the skeleton to change shape during childbirth • Enable body to move in response to skeletal muscle contraction A “joint” joins two bones or, parts of bones, together, regardless of ability of the bones to move around the joint 3 1 Some Useful Word Roots • Arthros – joint • Syn – together (immovable) • Dia – through, apart (freely moveable) • Amphi – on both sides (slightly moveable) Some Examples: Synarthrosis – An immovable joint Functional Classification Amphiarthrosis – A slightly movable joint (Very S-A-D) Diarthrosis – Freely movable joint What does the term ‘synostosis’ mean? 4 Classification of Joints How are the bones held together? How does the joint move? 3 answers 3 answers Structural Functional • Fibrous Joints • synarthrotic • dense connective tissues connect • immovable bones • amphiarthrotic • between bones in close contact • slightly movable • diarthrotic • Cartilaginous Joints • freely movable • hyaline cartilage or fibrocartilage connect bones • Synovial Joints • most complex • allow free movement • have a cavity 5 Joint Classification Structural Classification of Joints Fibrous Cartilaginous Synovial (D) Gomphosis (S) Synchondrosis -

The Skeletal System Joints Ppt Notes
Copy and Return to Teacher The Skeletal System: Joints Joints • Articulations of bones • Functions of joints o Hold bones together securely o Gives the rigid skeleton mobility • Ways joints are classified o Functionally o Structurally Functional Classification of Joints • Focuses on the amount of movement allowed • Joint types restricted mainly to the axial skeleton where firm attachments and protection of internal organs are priorities include: o Synarthroses – immovable joints o Amphiarthroses – slightly moveable joints • Joints predominate in the limbs where mobility is important: o Diarthroses – freely moveable joints Structural Classification of Joints • Based on whether fibrous tissue, cartilage or a joint cavity separates the bony regions. General rule: • Fibrous joints o Generally immovable • Cartilaginous joints o Some are immovable (synarthrotic), while most are slightly moveable (amphiarthrotic) • Synovial joints o Freely moveable (diarthrotic) Fibrous Joints • Bones united by fibrous tissue • Sutures – irregular edges of bone interlock, bound tightly by connective tissue fibers = essentially no movement • Syndesmoses – connecting fibers are longer and have more give • Example: joint connecting distal end of tibia and fibula Cartilaginous Joints • Bones ends connected by cartilage • Slightly moveable (amphiarthrotic) o Pubic symphysis o Intervertebral joints • Immovable (synarthrotic) o Hyaline-cartilage epiphyseal plates of growing long bones o Cartilaginous joints between the 1 st ribs and the sternum Synovial Joints • Articulating