The Lateral Ligament Is Attached to the Styloid Process of the Radius and to the Scaphoid Bone
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4Th SESSION 1
2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4th SESSION 1: Carpal Ligament 1 Stable Central Column Theory of Carpal Mechanics Michael Sandow FRACS Wakefield Orthopaedic Clinic Adelaide, Australia Background: The carpus is a complicated and functionally challenged mechanical system and advancements in the understanding have been compromised by the recognition that there is no standard carpal mechanical system and no typical wrist. This paper cover component of a larger project that seeks to develop a kinetic model of wrist mechanics to allow reverse analysis of the specific biomechanical controls or rule of a specific patient's carpus, and then use those to create a forward mathematical model to reproduce the unique individual's anatomical motion based on the extracted rules. Objectives and Methods: Based on previous observations, the carpus essentially moves with only 2 degrees of freedom - pitch (flexion / extension) and yaw (radial deviation / ulnar deviation), while largely preventing roll (pronation / supination). The object of this paper is therefore to present the background and justification to support the rules based motion (RBM) concept states that the motion of a mechanical system, such as the wrist, is the net interplay of 4 rules - morphology, constraint, interaction and load. The Stable Central Column Theory (SCCT) of wrist mechanics applies the concept of RBM to the carpus, and by using a reverse engineering computational analysis model, identified a consistent pattern of isometric constraints, creating a "Two-Gear Four-Bar" linkage. This study assessed the motion of the carpus using a 3D dynamic visualization model, and the hypothesis was that the pattern and direction of motion of the proximal row, and the distal row with respect the immediately cephalad carpal bones or radius would be very similar in all directions of wrist motion. -
Lecture Notes on Human Anatomy. Part One, Fourth Edition. PUB DATE Sep 89 NOTE 79P.; for Related Documents, See SE 051 219-221
DOCUMENT RESUME ED 315 320 SE 051 218 AUTHOR Conrey, Kathleen TITLE Lecture Notes on Human Anatomy. Part One, Fourth Edition. PUB DATE Sep 89 NOTE 79p.; For related documents, see SE 051 219-221. Black and white illustrations will not reproduce clearly. AVAILABLE FROM Aramaki Design and Publications, 12077 Jefferson Blvd., Culver City, CA 90506 ($7.75). PUB TYPE Guides - Classroom Use - Materials (For Learner) (051) EDRS PRICE MF01 Plus Postage. PC Not Available from EDRS. DESCRIPTORS *Anatomy; *Biological Sciences; *College Science; Higher Education; *Human Body; *Lecture Method; Science Education; Secondary Education; Secondary School Science; Teaching Guides; Teaching Methods ABSTRACT During the process of studying the specific course content of human anatomy, students are being educated to expand their vocabulary, deal successfully with complex tasks, anduse a specific way of thinking. This is the first volume in a set of notes which are designed to accompany a lecture series in human anatomy. This volume Includes discussions of anatomical planes and positions, body cavities, and architecture; studies of the skeleton including bones and joints; studies of the musculature of the body; and studiesof the nervous system including the central, autonomic, motor and sensory systems. (CW) *****1.**k07********Y*******t1.****+***********,****A*******r****** % Reproductions supplied by EDRS are the best that can be made from the original document. **************************************************************A**t***** "PERMISSION TO REPRODUCE -

38.3 Joints and Skeletal Movement.Pdf
1198 Chapter 38 | The Musculoskeletal System Decalcification of Bones Question: What effect does the removal of calcium and collagen have on bone structure? Background: Conduct a literature search on the role of calcium and collagen in maintaining bone structure. Conduct a literature search on diseases in which bone structure is compromised. Hypothesis: Develop a hypothesis that states predictions of the flexibility, strength, and mass of bones that have had the calcium and collagen components removed. Develop a hypothesis regarding the attempt to add calcium back to decalcified bones. Test the hypothesis: Test the prediction by removing calcium from chicken bones by placing them in a jar of vinegar for seven days. Test the hypothesis regarding adding calcium back to decalcified bone by placing the decalcified chicken bones into a jar of water with calcium supplements added. Test the prediction by denaturing the collagen from the bones by baking them at 250°C for three hours. Analyze the data: Create a table showing the changes in bone flexibility, strength, and mass in the three different environments. Report the results: Under which conditions was the bone most flexible? Under which conditions was the bone the strongest? Draw a conclusion: Did the results support or refute the hypothesis? How do the results observed in this experiment correspond to diseases that destroy bone tissue? 38.3 | Joints and Skeletal Movement By the end of this section, you will be able to do the following: • Classify the different types of joints on the basis of structure • Explain the role of joints in skeletal movement The point at which two or more bones meet is called a joint, or articulation. -

REVIEW ARTICLE Osteoarthritis of the Wrist
REVIEW ARTICLE Osteoarthritis of the Wrist Krista E. Weiss, Craig M. Rodner, MD From Harvard College, Cambridge, MA and Department of Orthopaedic Surgery, University of Connecticut Health Center, Farmington, CT. Osteoarthritis of the wrist is one of the most common conditions encountered by hand surgeons. It may result from a nonunited or malunited fracture of the scaphoid or distal radius; disruption of the intercarpal, radiocarpal, radioulnar, or ulnocarpal ligaments; avascular necrosis of the carpus; or a developmental abnormality. Whatever the cause, subsequent abnormal joint loading produces a spectrum of symptoms, from mild swelling to considerable pain and limitations of motion as the involved joints degenerate. A meticulous clinical and radiographic evaluation is required so that the pain-generating articulation(s) can be identi- fied and eliminated. This article reviews common causes of wrist osteoarthritis and their surgical treatment alternatives. (J Hand Surg 2007;32A:725–746. Copyright © 2007 by the American Society for Surgery of the Hand.) Key words: Wrist, osteoarthritis, arthrodesis, carpectomy, SLAC. here are several different causes, both idio- of events is analogous to SLAC wrist and has pathic and traumatic, of wrist osteoarthritis. been termed scaphoid nonunion advanced collapse Untreated cases of idiopathic carpal avascular (SNAC). Wrist osteoarthritis can also occur second- T 1 2 necrosis, as in Kienböck’s or Preiser’s disease, may ary to an intra-articular fracture of the distal radius or result in radiocarpal arthritis. Congenital wrist abnor- ulna or from an extra-articular fracture resulting in malities, such as Madelung’s deformity,3,4 can lead malunion and abnormal joint loading. -

A Rare Combination of Two Uncommon Fractures of the Carpal Bones
12 Maart 1960 S.A. TYDSKRIF VIR GE 'EESKUNDE 221 whether a low tracheotomy would have produced better 5. There must be no evidence of any pulmonary com figures. I performed a low tracheotomy on the first bulbo plication indicating broncbial obstruction and atelectasis. spinal case to be treated by Lassen's method in the 1956 The difficulty in detubation which ometimes arises in Cape Town polio epidemic and I must confess the tendency infants \ ho have had a tracheotomy for any length of time of the tube to' slip down the right bronchus required constant is a familiar problem. In the first in tance a laryngo opyand watching. The right-angled tube designed by Crampton bronchoscopy hould be carried out to a certain whether Smith eliminates this hazard, however, and with it I think there is any tenosis or whether granulations are present in this objection to a below-isthmus tracheotomy falls away. the trachea. When such granulations have been encountered If tracheotomy is being performed with a view to inter they have, in my experience, in ariably been found to be mittent-positive-pressure respiration it is necessary to excise a prolapsing into the trachea from the margins of the toma window from the anterior tracheal wall. This should be oval and not arising within the trachea itself. I have found that the in shape with its greatest diameter in the axis of the trachea. most effective way of dealing with these is to remove them If the tracheotomy is for an obstructive lesion or for tracheo under endotracheal anaesthesia with aHartman's granulation-. -
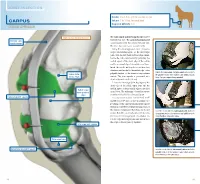
Carpus Volume: 7 to 10 Ml for Each Joint Degree of Difficulty: 1/3 Dorsal Approach
JOINT INJECTION needle: 1 to 1.5 in. (2.5 to 3.8 cm), 20 ga Carpus volume: 7 to 10 ml for each joint Degree of difficulty: 1/3 Dorsal approach right carpus, dorsomedial view The radiocarpal and intercarpal joints can be extensor carpi entered with ease. The carpometacarpal joint radialis tendon communicates with the intercarpal joint and, therefore, does not require separate entry. Using the dorsal approach, enter the radio- carpal (antebrachiocarpal) or the intercarpal joints with the limb held and the carpus flexed. Locate the radiocarpal joint by palpating the medial aspect of the distal edge of the radius and the proximal edge of the radial carpal bone. Insert the needle midway between these two structures and medial to the medial edge of the palpate the radiocarpal and intercarpal joints medial to palpable tendon of the extensor carpi radialis radius (distal the palpable tendon of the extensor carpi radialis muscle. medial edge) muscle. The joint capsule is penetrated at a Note: The right carpus is being palpated. depth of about 0.5 inch (1.3 cm). Locate the intercarpal joint by palpating the distal edge of the radial carpal bone and the medial aspect of the proximal edge of the third radial carpal bone (proximal carpal bone. The technique of needle insertion edge) is similar to that for the radiocarpal joint. radiocarpal joint capsule It is important to point out that Ford et al47 and Moyer et al48 showed that the palmar out- pouchings of the carpometacarpal joint capsule extend into the fibers of the proximal portion of the suspensory ligament. -

Osteoblastoma of the Trapezoid Bone and Triquetral Bone: Report of Two Cases
CASE REPORT Acta Orthop Traumatol Turc 2013;47(5):376-378 doi:10.3944/AOTT.2013.3081 Osteoblastoma of the trapezoid bone and triquetral bone: report of two cases ‹brahim KAYA1, Burak BOYNUK2, Caner GÜNERBÜYÜK3, Ak›n U⁄RAfi4 1Department of Orthopedics and Traumatology, Haseki Training and Research Hospital, ‹stanbul, Turkey; 2Department of Orthopedics and Traumatology, Bak›rköy Ac›badem Hospital, ‹stanbul, Turkey; 3Department of Orthopedics and Traumatology, 29 May›s Hospital, ‹stanbul, Turkey; 4Department of Orthopedics and Traumatology, ‹stanbul Medipol University, School of Medicine, ‹stanbul, Turkey Osteoblastoma is a benign local aggressive tumor mostly localized in the vertebra or long bones. Carpal location and recurrence are extremely rare. Treatment options include either curettage or wide en bloc resection which causes functional disability in the hand and wrist and should be reserved only for recurrence. We present a case of recurrent trapezoid osteoblastoma previously treated with curet- tage of the trapezoid bone and a case of primary triquetral osteoblastoma. Key words: Curettage; osteoblastoma; trapezoid bone; triquetral bone. Osteoblastoma is a benign primary bone tumor first pain increased at night and had a good response to non- described as “giant osteoid osteoma” by Dahlin and steroidal analgesic drugs. Radiographs, computerized Johnson in 1954.[1] Later, in 1956, Lichtenstein and Jaffe tomography and magnetic resonance imaging (MRI) named this tumor “osteoblastoma” in two different arti- revealed findings resembling avascular necrosis of the cles.[2] It is an uncommon benign but locally aggressive trapezoid bone, periosteal reaction at the second tumor, most commonly located in the vertebral column metacarpal and generalized edema in the dorsal com- or metaphysis of long bones. -

Readingsample
Color Atlas of Human Anatomy Vol. 1: Locomotor System Bearbeitet von Werner Platzer 6. durchges. Auflage 2008. Buch. ca. 480 S. ISBN 978 3 13 533306 9 Zu Inhaltsverzeichnis schnell und portofrei erhältlich bei Die Online-Fachbuchhandlung beck-shop.de ist spezialisiert auf Fachbücher, insbesondere Recht, Steuern und Wirtschaft. Im Sortiment finden Sie alle Medien (Bücher, Zeitschriften, CDs, eBooks, etc.) aller Verlage. Ergänzt wird das Programm durch Services wie Neuerscheinungsdienst oder Zusammenstellungen von Büchern zu Sonderpreisen. Der Shop führt mehr als 8 Millionen Produkte. 130 Upper Limb: Bones, Ligaments, Joints Radiocarpal and Midcarpal Joints Ligaments in the Region of the Wrist (A–E) (A–E) Four groups of ligaments can be distin- The radiocarpal or wrist joint is an ellip- guished: soid joint formed on one side by the radius (1) and the articular disk (2) and on the Ligaments which unite the forearm bones with other by the proximal row of carpal bones.Not the carpal bones (violet). These include the all the carpal bones of the proximal row are ulnar collateral ligament (8), the radial col- in continual contact with the socket- lateral ligament (9), the palmar radiocarpal shaped articular facet of the radius and the ligament (10), the dorsal radiocarpal liga- disk. The triquetrum (3), only makes close ment (11), and the palmar ulnocarpal liga- contact with the disk during ulnar abduc- ment (12). tion and loses contact on radial abduction. Ligaments which unite the carpal bones with The capsule of the wrist joint is lax, dorsally one another,orintercarpal ligaments (red). These comprise the radiate carpal ligament Upper Limb relatively thin, and is reinforced by numer- ous ligaments. -

Bones and Joints of the Upper Limb: Forearm and Hand
Unit 4: Bones and joints of the upper limb: forearm and hand Chapter 6 (Upper limb) GENERAL OBJECTIVES: - recognize, name and correctly orient forearm and hand bones - understand movements in elbow, wrist and hand joints SPECIFIC OBJECTIVES: Bones of the forearm and hand Identify the bony features on each part of the following bones: RADIUS - Upper End - Shaft - Lower End ULNA - Upper End - Shaft - Lower End Deduce (from the shape of the articular surfaces) the movements at (i) the elbow joint and (ii) the radioulnar joints. Indicate the bony attachments of the major ligaments which help to maintain the stability of these joints (while allowing their mobility). Identify the following bones CARPALS - Proximal Row - Distal Row METACARPALS PHALANGES Identify the attachments of the Flexor Retinaculum and define the "Carpal Tunnel". Deduce (from the shape of the articular surfaces) the movements at (i) the wrist joint (ii) the carpometacarpal joint of the thumb (iii) metacarpophalangeal joints (iv) interphalangeal joints Indicate the bony attachments of the major ligaments which help to maintain the stability of these joints (while allowing their mobility). Joints of the forearm and hand Elbow Joint Articular Surfaces (Humeroulnar & Humeroradial) Fibrous Capsule & Joint Cavity Synovial Membrane Collateral Ligaments ( Medial & Lateral) Special Structures: Olecranon Bursa Other Bursae, Pads of Fat Movements at the Elbow Joint: Flexion/Extension Stability Carrying Angle Radioulnar Joints Proximal Radioulnar Joint Annular Ligament Distal Radioulnar -

Carpal Fractures
CURRENT CONCEPTS Carpal Fractures Nina Suh, MD, Eugene T. Ek, MBBS, PhD, Scott W. Wolfe, MD CME INFORMATION AND DISCLOSURES The Review Section of JHS will contain at least 3 clinically relevant articles selected by the Provider Information can be found at http://www.assh.org/Pages/ContactUs.aspx. editor to be offered for CME in each issue. For CME credit, the participant must read the Technical Requirements for the Online Examination can be found at http://jhandsurg. articles in print or online and correctly answer all related questions through an online org/cme/home. examination. The questions on the test are designed to make the reader think and will occasionally require the reader to go back and scrutinize the article for details. Privacy Policy can be found at http://www.assh.org/pages/ASSHPrivacyPolicy.aspx. The JHS CME Activity fee of $30.00 includes the exam questions/answers only and does not ASSH Disclosure Policy: As a provider accredited by the ACCME, the ASSH must ensure fi include access to the JHS articles referenced. balance, independence, objectivity, and scienti c rigor in all its activities. Disclosures for this Article Statement of Need: This CME activity was developed by the JHS review section editors and review article authors as a convenient education tool to help increase or affirm Editors reader’s knowledge. The overall goal of the activity is for participants to evaluate the Ghazi M. Rayan, MD, has no relevant conflicts of interest to disclose. appropriateness of clinical data and apply it to their practice and the provision of patient Authors care. -

Gen Anat-Joints
JOINTS Joint is a junction between two or more bones Classification •Functional Based on the range and type of movement they permit •Structural On the basis of their anatomic structure Functional Classification • Synarthrosis No movement e.g. Fibrous joint • Amphiarthrosis Slight movement e.g. Cartilagenous joint • Diarthrosis Movement present Cavity present Also called as Synovial joint eg.shoulder joint Structural Classification Based on type of connective tissue binding the two adjacent articulating bones Presence or absence of synovial cavity in between the articulating bone • Fibrous • Cartilagenous • Synovial Fibrous Joint Bones are connected to each other by fibrous (connective ) tissue No movement No synovial cavity • Suture • Syndesmosis • Gomphosis Sutural Joints • A thin layer of dens fibrous tissue binds the adjacent bones • These appear between the bones which ossify in membrane • Present between the bones of skull e.g . coronal suture, sagittal suture • Schindylesis: – rigid bone fits in to a groove on a neighbouring bone e.g. Vomer and sphenoid Gomphosis • Peg and socket variety • Cone shaped root of tooth fits in to a socket of jaw • Immovable • Root is attached to the socket by fibrous tissue (periodontal ligament). Syndesmosis • Bony surfaces are bound together by interosseous ligament or membrane • Membrane permits slight movement • Functionally classified as amphiarthrosis e.g. inferior tibiofibular joint Cartilaginous joint • Bones are held together by cartilage • Absence of synovial cavity . Synchondrosis . Symphysis Synchondrosis • Primary cartilaginous joint • Connecting material between two bones is hyaline cartilage • Temporary joint • Immovable joint • After a certain age cartilage is replaced by bone (synostosis) • e.g. Epiphyseal plate connecting epiphysis and diphysis of a long bone, joint between basi-occiput and basi-sphenoid Symphysis • Secondary cartilaginous joint (fibrocartilaginous joint) • Permanent joint • Occur in median plane of the body • Slightly movable • e.g. -

Clinical Orthopedics Advanced Research Journal Case Report Teodonno F, Et Al
1 VolumeVolume 2019; 2018; Issue Issue 01 Clinical Orthopedics Advanced Research Journal Case Report Teodonno F, et al. Clin Ortho Adv Res J: COARJ-100003. Trans-Scaphoid Perilunate Dislocation with Fractured Triquetral Bone in A Pediatric Patient: A 10-Month Follow Up of a Case Report Teodonno F*, Macera A, Crespo Lastras P, Cervero Suárez FJ, Suárez Rueda C and Márquez Ámbite J Department of Orthopedic Surgery and Traumatology, Infanta Elena Hospital, Valdemoro, Madrid, Spain *Corresponding author: Francesca Teodonno, Department of Orthopedic Surgery and Traumatology, Infanta Elena Hospital, Valde- moro, Madrid, Spain, Tel: +34918948410; Email: [email protected] Citation: Francesca Teodonno, et al. (2019) Trans-Scaphoid Perilunate Dislocation with Fractured Triquetral Bone in A Pediatric Pa- tient: A 10-Month Follow Up of a Case Report. Clin Ortho Adv Res J: COARJ-100003. Received date: 28 October, 2019; Accepted date: 04 November, 2019; Published date: 15 November, 2019 Abstract Transcarpal fractures and dislocations in pediatric patients are seldomly reported in literature. Trans-scaphoid dislocations rep- resent only the 1,4% of all scaphoid fractures in the pediatric population.We present the case of 12-year-old boy that, after a fall on the outstretched hand from a motorbike, sustains a trans-scaphoid perilunate dislocation with non displaced fractures of the scaphoid and triquetrum bones, and was treated conservativelythrough closed reduction for the dislocation and immobilization with a closed cast. At final follow up of 10 months, the fractures healed well with a full return of good wrist function. This unusual injury is described so that it may be better acknowledged in the future.