Bones and Joints of the Upper Limb: Forearm and Hand
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4Th SESSION 1
2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4th SESSION 1: Carpal Ligament 1 Stable Central Column Theory of Carpal Mechanics Michael Sandow FRACS Wakefield Orthopaedic Clinic Adelaide, Australia Background: The carpus is a complicated and functionally challenged mechanical system and advancements in the understanding have been compromised by the recognition that there is no standard carpal mechanical system and no typical wrist. This paper cover component of a larger project that seeks to develop a kinetic model of wrist mechanics to allow reverse analysis of the specific biomechanical controls or rule of a specific patient's carpus, and then use those to create a forward mathematical model to reproduce the unique individual's anatomical motion based on the extracted rules. Objectives and Methods: Based on previous observations, the carpus essentially moves with only 2 degrees of freedom - pitch (flexion / extension) and yaw (radial deviation / ulnar deviation), while largely preventing roll (pronation / supination). The object of this paper is therefore to present the background and justification to support the rules based motion (RBM) concept states that the motion of a mechanical system, such as the wrist, is the net interplay of 4 rules - morphology, constraint, interaction and load. The Stable Central Column Theory (SCCT) of wrist mechanics applies the concept of RBM to the carpus, and by using a reverse engineering computational analysis model, identified a consistent pattern of isometric constraints, creating a "Two-Gear Four-Bar" linkage. This study assessed the motion of the carpus using a 3D dynamic visualization model, and the hypothesis was that the pattern and direction of motion of the proximal row, and the distal row with respect the immediately cephalad carpal bones or radius would be very similar in all directions of wrist motion. -

An Analytical Study on the Finger Flexion Cascade in General Population of Various Occupations
Research Article Orthop Rheumatol Open Access J Volume 1 Issue 1 - August 2015 Copyright © All rights are reserved by Jibu George varghese An Analytical Study on the Finger Flexion Cascade in General Population of Various Occupations K. Asha1, Jibu George Varghese1, V. Srinivasan1 and Kannabiran Bhojan2 1Sri Ramachandra University, India 2RVS College Of Physiotherapy, India Submission: September 10, 2015; Published: October 06, 2015 *Corresponding author: Jibu George varghese, Assistant Professor, Faculty of Physiotherapy, Sri Ramachandra University, Coimbatore, India, Email: Abstract Background and Purpose: Finger flexion cascade (FFC) is a natural phenomenon that is observed in the hand at complete rest. It is the posture/alignment of fingers with some flexion at all the joints of digits, beginning with less flexion at the index finger, progressing to more flexion towards the little finger. The FFC may vary in individuals of different occupations as occupational activities performed over a prolonged period may have an influence on the finger flexion ROM thereby influencing the normal FFC. Understanding the variations may serve as a valuable tool to manage rehabilitation following hand injuries, which may include improving the finger flexion joint ROM suited to the need of the individual. The purpose of this study was to observe, measure and document the FFC in individuals belonging to different occupations and to analyzeMethods: whether a significant variation may be seen within the occupations and between the occupations. One hundred twenty five healthy individuals with an age ranging between 20 to 60 years who met the inclusion criteria participated in the study. Occupations included were electricians, maintenance workers and desk workers. -

REVIEW ARTICLE Osteoarthritis of the Wrist
REVIEW ARTICLE Osteoarthritis of the Wrist Krista E. Weiss, Craig M. Rodner, MD From Harvard College, Cambridge, MA and Department of Orthopaedic Surgery, University of Connecticut Health Center, Farmington, CT. Osteoarthritis of the wrist is one of the most common conditions encountered by hand surgeons. It may result from a nonunited or malunited fracture of the scaphoid or distal radius; disruption of the intercarpal, radiocarpal, radioulnar, or ulnocarpal ligaments; avascular necrosis of the carpus; or a developmental abnormality. Whatever the cause, subsequent abnormal joint loading produces a spectrum of symptoms, from mild swelling to considerable pain and limitations of motion as the involved joints degenerate. A meticulous clinical and radiographic evaluation is required so that the pain-generating articulation(s) can be identi- fied and eliminated. This article reviews common causes of wrist osteoarthritis and their surgical treatment alternatives. (J Hand Surg 2007;32A:725–746. Copyright © 2007 by the American Society for Surgery of the Hand.) Key words: Wrist, osteoarthritis, arthrodesis, carpectomy, SLAC. here are several different causes, both idio- of events is analogous to SLAC wrist and has pathic and traumatic, of wrist osteoarthritis. been termed scaphoid nonunion advanced collapse Untreated cases of idiopathic carpal avascular (SNAC). Wrist osteoarthritis can also occur second- T 1 2 necrosis, as in Kienböck’s or Preiser’s disease, may ary to an intra-articular fracture of the distal radius or result in radiocarpal arthritis. Congenital wrist abnor- ulna or from an extra-articular fracture resulting in malities, such as Madelung’s deformity,3,4 can lead malunion and abnormal joint loading. -
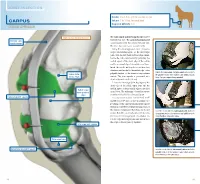
Carpus Volume: 7 to 10 Ml for Each Joint Degree of Difficulty: 1/3 Dorsal Approach
JOINT INJECTION needle: 1 to 1.5 in. (2.5 to 3.8 cm), 20 ga Carpus volume: 7 to 10 ml for each joint Degree of difficulty: 1/3 Dorsal approach right carpus, dorsomedial view The radiocarpal and intercarpal joints can be extensor carpi entered with ease. The carpometacarpal joint radialis tendon communicates with the intercarpal joint and, therefore, does not require separate entry. Using the dorsal approach, enter the radio- carpal (antebrachiocarpal) or the intercarpal joints with the limb held and the carpus flexed. Locate the radiocarpal joint by palpating the medial aspect of the distal edge of the radius and the proximal edge of the radial carpal bone. Insert the needle midway between these two structures and medial to the medial edge of the palpate the radiocarpal and intercarpal joints medial to palpable tendon of the extensor carpi radialis radius (distal the palpable tendon of the extensor carpi radialis muscle. medial edge) muscle. The joint capsule is penetrated at a Note: The right carpus is being palpated. depth of about 0.5 inch (1.3 cm). Locate the intercarpal joint by palpating the distal edge of the radial carpal bone and the medial aspect of the proximal edge of the third radial carpal bone (proximal carpal bone. The technique of needle insertion edge) is similar to that for the radiocarpal joint. radiocarpal joint capsule It is important to point out that Ford et al47 and Moyer et al48 showed that the palmar out- pouchings of the carpometacarpal joint capsule extend into the fibers of the proximal portion of the suspensory ligament. -

Readingsample
Color Atlas of Human Anatomy Vol. 1: Locomotor System Bearbeitet von Werner Platzer 6. durchges. Auflage 2008. Buch. ca. 480 S. ISBN 978 3 13 533306 9 Zu Inhaltsverzeichnis schnell und portofrei erhältlich bei Die Online-Fachbuchhandlung beck-shop.de ist spezialisiert auf Fachbücher, insbesondere Recht, Steuern und Wirtschaft. Im Sortiment finden Sie alle Medien (Bücher, Zeitschriften, CDs, eBooks, etc.) aller Verlage. Ergänzt wird das Programm durch Services wie Neuerscheinungsdienst oder Zusammenstellungen von Büchern zu Sonderpreisen. Der Shop führt mehr als 8 Millionen Produkte. 130 Upper Limb: Bones, Ligaments, Joints Radiocarpal and Midcarpal Joints Ligaments in the Region of the Wrist (A–E) (A–E) Four groups of ligaments can be distin- The radiocarpal or wrist joint is an ellip- guished: soid joint formed on one side by the radius (1) and the articular disk (2) and on the Ligaments which unite the forearm bones with other by the proximal row of carpal bones.Not the carpal bones (violet). These include the all the carpal bones of the proximal row are ulnar collateral ligament (8), the radial col- in continual contact with the socket- lateral ligament (9), the palmar radiocarpal shaped articular facet of the radius and the ligament (10), the dorsal radiocarpal liga- disk. The triquetrum (3), only makes close ment (11), and the palmar ulnocarpal liga- contact with the disk during ulnar abduc- ment (12). tion and loses contact on radial abduction. Ligaments which unite the carpal bones with The capsule of the wrist joint is lax, dorsally one another,orintercarpal ligaments (red). These comprise the radiate carpal ligament Upper Limb relatively thin, and is reinforced by numer- ous ligaments. -

Wrist Complex
WRIST COMPLEX DR DIGVIJAY SHARMA ASSISTANT PROFESSOR DEPARTMENT OF PHYSIOTHERAPY C.S.J.M. UNIVERSITY KANPUR It consist of 2 compound joints- Radiocarpal joint Midcarpal joint STRUCTURE- RADIOCARPAL JOINTS- This joint is formed by radius and radioulnar disc proximally and by the scaphoid, lunate and triquetral distally. The proximal joint surface is composed of I. Lateral radial facet which articulate with scaphoid. II. Medial Radial facet articulates with lunate III. The triangular fibro cartilage complex that articulate with triquetrum predominantly and lunate with up to some extent . When the wrist is in neutral position ulna does not participate as the part of the radiocarpal joint Other than an attachment site for the TFCC(triangular fibro cartilage complex). MIDCARPAL JOINT It is the articulation between a scaphoid, lunate and triquetrum proximally and distal carpal row composed of the trapezium, trapezoid , capitate and hamate. The mid carpal joint surfaces are complex with an overall reciprocally concavo- convex configuration. Functionally the distal carpal row moves as an almost fix unit. The capitate and hamate are most strongly bound together, So only small amount of play is possible between them. The union of distal carpal also results in nearly equal distribution of load across - A scaphoid – trapezium- trapezoid, Scaphoid-capitate, lunate- capitate , the triquetrum- hamate articulations. Together the bones of the distal carpal row contribute 20 of freedom of wrist complex with varying amounts of radial/ulnar deviation and flexion/extension credited to the joint . LIGAMENTS- The ligaments of the wrist complex are divided into- I. Extrinsic ligaments II. Intrinsic ligaments The extrinsic ligaments connect the carpals to the radius or ulna proximally and to the metacarpals distally. -

ABSTRACT Background: a Normal Finger Flexion Cascade (FFC) Is Formed by the Fingers of the Hand When the Hand in a Relaxed Position
Int J Physiother. Vol 7(2), 59-68, April (2020) ISSN: 2348 - 8336 ORIGINAL ARTICLE GENDER ORIENTED VARIATIONS IN THE FINGER FLEXION CASCADE IN NORMAL INDIVIDUALS *¹Jibu George Varghese, M.P.T., CMP., COMPT., MCTA. ²Vidhya Venugopal, M.Sc., Ph.D ³V. Srinivasan, M.S., M.Ch. 4G. A. Geetha Hari Priya, M.P.T IJPHY ABSTRACT Background: A normal Finger Flexion Cascade (FFC) is formed by the fingers of the hand when the hand in a relaxed position. Usually, the fingers of the hand assume a flexed position; gender may influence the normative values of the resting hand due to differences in the anatomical structure of hand and frequency of usage of joints of hand in their respective occupation and habitual activities of daily living. Hence the study aims to find the difference in the FFC between men and women in power grip and nonpower grip occupational activities. Methods: A cross-sectional study was conducted in a mixed population of five hundred active individuals aged between 25 and 40 years belonging to various occupations of industrial work and individuals working with software companies. Individuals who fulfilled the inclusion criteria participated in the study. After completing a questionnaire based on occupation, the subjects were grouped into power grip users and nonpower grip users. The range of motion of the joints of all the fingers, namely, metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints of both dominant hand and nondominant hand was measured using universal finger goniometer, and the composite finger flexion was recorded using a geometric ruler. The results were analyzed, and Un-paired T-test was used to compare the FFC between the power grip and the nonpower grip group. -

Biomimetic Design and Development of a Prosthetic Hand: Prototype 1.0
15th National Conference on Machines and Mechanisms NaCoMM2011-97 Biomimetic Design and Development of a Prosthetic Hand: Prototype 1.0 Nayan M. Kakoty, Shyamanta M. Hazarika Abstract This paper reports the biomimetic design and development of a prototype of extreme upper limb prosthesis. The motivation for developing a new prosthetic hand is provided by the fact that low functionality and low controllability are the most important reasons why amputees do not use their prosthetic hands. In addi- tion, although multifingered hand prosthesis has appeared in the market, the cost is exorbitantly high and out of reach of common people, which is particularly true for developing countries like India. This paper presents an anthropomor- phic design of a prosthetic hand with 15 degrees of freedom using underactuated mechanism. The bioinspired control is through electromyogram signals based on support vector machine for classification of six grasps involved in 70% of daily living activities. Keywords: Biomimetic, Prosthetic hand, Electromyogram, Grasps 1 Introduction Dexterous artificial hand design and manipulation is an active research topic. A very interesting practical application is the field of upper limb prosthetics. Number of lab- oratory prototypes and commercial versions of upper limb prosthesis have been avail- able. However, electromyogram (EMG) based control is still rudimentary, being lim- ited to a few hand postures; and control is non-intuitive, in the sense that the user is required to learn to associate muscle remnants actions to unrelated posture of the prosthesis. Neuro-bionic hands address some of these issues. However, commercially launched variants (such as i-Limb from Touch Bionics [1]) are exorbitantly priced. -
Prezentace Aplikace Powerpoint
Bones, ligament, joints of the upper and lower limb Pelvis Sternoclavicular joint Articular disc Anterior sternoclavicular ligament Posterior sternoclavicular ligament Costoclavicular ligament Interclavicular ligament Acromioclavicular joint Acromioclavicular ligament (Articular disc) Coracoclavicular ligament Trapezoid ligament Conoid ligament Glenohumeral joint; Shoulder joint Glenoid labrum Glenohumeral ligaments Coracohumeral ligament Transverse humeral ligament Rotatory cuff Coraco-acromial ligament Superior transverse scapular ligament Elbow joint Humero-ulnar joint Humeroradial joint Proximal radio- ulnar joint Ulnar collateral ligament Radial collateral ligament Anular ligament of radius Radio-ulnar syndesmosis Interosseous membrane of forearm Oblique cord Distal radio-ulnar joint Articular disc Sacciform recess Joints of hand Wrist joint Ulnar collateral ligament of wrist joint Radial collateral ligament of wrist joint Carpal joints; Intercarpal joints Midcarpal joint Radiate carpal ligament Interosseus intercarpal ligaments Pisiform joint Pisohamate ligament Pisometacarpal ligament Carpal tunnel Carpometacarpal joints Dorsal carpometacarpal ligaments Palmar carpometacarpal ligaments Carpometacarpal joint of thumb Intermetacarpal joints Dorsal metacarpal ligaments Palmar metacarpal ligaments Interosseous metacarpal ligaments Interosseous metacarpal spaces Joints of hand Wrist joint Ulnar collateral ligament of wrist joint Radial collateral ligament of wrist joint Carpal joints; Intercarpal joints Midcarpal joint Radiate carpal -

Bilateral Spontaneous Bony Ankylosis of the Elbow Following Burn: a Case Report and Review of the Literature
Case Report Journal of Orthopaedic Case Reports 2018 September-October : 8(5):Page 43-46 Bilateral Spontaneous Bony Ankylosis of the Elbow Following Burn: A Case Report and Review of the Literature Raju Vaishya¹, Amit Kumar Singh¹, Amit Kumar Agarwal¹, Vipul Vijay¹ Learning Point of the Article: The possibility of spontaneous bony fusion in deep burn injuries around the joint should be kept in mind so that effective preventive measures can be taken. Abstract Introduction: Ankylosis of a joint could be intra-articular or extra-articular. Intra-articular ankylosis may be fibrous or bony. Soft tissue contracture and heterotopic ossification area common finding in patients with a deep burn around the joints. Intra-articular bony ankylosis after burn is uncommon, but a possible complication and we present a rare case with bilateral elbow involvement. Case Report: A 35-year-old female presented to us with contracture of both the elbows. She had a history of severe accidental thermal burn involving mainly the front of both the upper limbs 6months back. She developed burn contracture of both elbows. X-rays of both elbows showed bony fusion. Conclusion: Spontaneous bony fusion occurs in various pathologies, some are well known, but some are rare and unusual. Development of soft tissue contracture in deep burn is quite typical, followed by extra-articular ankylosis, but true spontaneous bony fusion can also occur. The possibility of spontaneous bony fusion in deep burn injuries around the joint should be kept in mind by both plastic surgeons and orthopedic surgeons. Keywords: Burn contracture, elbow, bony ankylosis, ossification, joints. -

(DRUJ) Midcarpal Joint Carpometa
12/20/2016 Radiocarpal Joint Mobilization of the Wrist 2017 EATA Student Conference Mary L. Mundrane-Zweiacher MPT, ATC, CHT [email protected] Radiocarpal Joint Ligaments Distal Radioulnar Joint (DRUJ) Midcarpal Joint Carpometacarpal Joint 1 12/20/2016 First CMC Joint The Extrinsic Hand Muscles: The Extrinsic Hand Muscles: Volar Aspect Volar Aspect • Palmaris longus • Flexor carpi radialis • Flexor Digitorum • Flexor carpi ulnaris Profundus (FDP) • Flexor Pollicis Longus • Flexor Digitorum • Flexor Digitorum Superficialis (FDS) Profundus (FDP) • Flexor Digitorum Superficialis (FDS) 2 12/20/2016 FDS FDP The Extrinsic Hand Muscles: Visible Extensor Mechanism Dorsal Aspect • Extensor Pollicis Longus (EPL) • Extensor Pollicis Brevis (EPB) • Abductor Pollicis Longus (APL) • Extensor indicis • Extensor Digitorum Communis (EDC) The Extrinsic Hand Muscles: The Intrinsic Hand Muscles Dorsal Aspect • Extensor carpi radialis • Lumbricales longus ( ECRL) • Dorsal Interossei • Extensor carpi radialis • Palmar (Volar) brevis (ECRB) Interossei • Extensor carpi ulnaris •Thenar Muscles • Extensor digiti minimi • Hypothenar Muscles • Adductor Pollicis 3 12/20/2016 The Intrinsic Hand Muscles The Intrinsic Hand Muscles • Lumbricales • Lumbricales • Dorsal Interossei • Dorsal Interossei • Palmar (Volar) • Palmar (Volar) Interossei Interossei • Thenar Muscles •Thenar Muscles • Hypothenar Muscles • Hypothenar Muscles • Adductor Pollicis • Adductor Pollicis Volar Plate Pulley Systems of the Hand The Lymphatic System Myofascial/Skin • It is the only system that can remove large • The dorsum of the hand is very different molecule substances such as excess plasma than the palm proteins, hormones, fat cells, and waste products from the interstitium that you see in chronic • The palmar fascia has longitudinal, edema. The lymphatics are tubes which are in the transverse, and vertical fibers dermis layer of the skin; they rely on changes in • The vertical fibers run superficially to interstitial pressure to open and close stabilize the thick palmar skin (pressures>60mmHg will collapse the tubes). -

Physical Examination of the Wrist: Useful Provocative Maneuvers
CURRENT CONCEPTS Physical Examination of the Wrist: Useful Provocative Maneuvers William B. Kleinman, MD Chronic wrist pain resulting from partial interosseous ligament injury remains a diagnostic dilemma for many hand and orthopedic surgeons. Overuse of costly diagnostic studies including magnetic resonance imaging, computed tomography scans, and bone scans can be further frustrating to the clinician because of their inconsistent specificity and reliability in these cases. Physical diagnosis is an effective (and underused) means of establishing a working diagnosis of partial ligament injury to the wrist. Carefully performed provocative maneuvers can be used by the clinician to reproduce the precise character of a patient’s problem, reliably establish a working diagnosis, and initiate a plan of treatment. Using precise physical examination techniques, the examiner introduces energy into the wrist in a manner that puts load on specific support ligaments of the carpus, leading to an accurate diagnosis. This article provides a broad spectrum of physical diagnostic tools to help the surgeon develop a working diagnosis of partial wrist ligament injuries in the face of chronic wrist pain and normal x-rays. (J Hand Surg Am. 2015;-(-):-e-. Copyright Ó 2015 by the American Society for Surgery of the Hand. All rights reserved.) Key words Carpus (wrist), physical examination, ligament injuries, provocative maneuvers, anatomy. VER THE PAST HALF-CENTURY, a plethora of PATHOMECHANICS OF CARPAL LIGAMENT clinical and laboratory research has been pub- INJURY O lished on the kinesiology and biomechanics of The complex nature of carpal mechanics can be simpli- the wrist joint. Gross and micro cadaver dissections fied by considering the distal carpal row (trapezium, have elucidated details of wrist anatomy; sophisticated trapezoid, capitate, and hamate) as securely attached to imaging studies have clearly defined mechanisms of the medial 4 metacarpals through short, tight, intrinsic carpal motion; and mechanical studies under load-to- ligaments.