Carpal Fractures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Osteoid Osteoma of the Trapezoid Bone
'-DIDUL)1DMG0D]KDU Case Report Osteoid Osteoma of the Trapezoid Bone Dawood Jafari MD1)DULG1DMG0D]KDU0'1 Abstract Osteoid osteoma is a benign, bone-forming tumor that rarely involves the carpal bones. We report a case of osteoid osteoma of the trap- H]RLGFDUSDOERQHZLWKH[WHQVLRQWRWKHDGMDFHQWVHFRQGPHWDFDUSDOERQH&KURQLFZULVWSDLQDQGORFDOWHQGHUQHVVZHUHWKHPDMRUFOLQLFDO signs and symptoms. In chronic wrist pain osteoid osteoma and the possibility of extension to the adjacent bones should be considered. Keywords: &DUSDOERQHPHWDFDUSDORVWHRLGRVWHRPDWUDSH]RLG Cite the article as: Jafari D, Najd Mazhar F. Osteoid Osteoma of the Trapezoid Bone. Arch Iran Med. 2012; 15(12): 777 – 779. Introduction RSV\WKURXJKDGRUVDODSSURDFK:HXVHGDVPDOOGULOOELWDQG¿QH osteotome to remove the involved area, which included the adjacent steoid osteoma is a benign bone tumor that rarely localizes articular surface of the trapezoid. The biopsy specimen had a highly to the carpal bones.1,2 Wrist pain usually is the main com- vascular reddish nidus embedded in normal bone (Figure 5). We no- O plaint and because it rarely involves the carpal bone, diag- ticed that the articular surface of the second metacarpal was eroded nosis is often delayed. It has been reported in the scaphoid and lu- and softened (Figure 6). Following curettage, we sent the specimen nate areas; however, the trapezoid is an exceedingly rare location from the base of the second metacarpal in a separate container for for osteoid osteoma. Bifocal involvement of adjacent carpal bones pathologic analysis. The results of the histologic examinations of has been reported previously but to the best of our knowledge ex- both biopsy specimens indicated osteoid osteoma (Figure 7). Since tension of osteoid osteoma through the joint to adjacent bone has we had only one nidus at the CT scan and involvement of both trap- not been mentioned in the literature. -

A Rare Combination of Two Uncommon Fractures of the Carpal Bones
12 Maart 1960 S.A. TYDSKRIF VIR GE 'EESKUNDE 221 whether a low tracheotomy would have produced better 5. There must be no evidence of any pulmonary com figures. I performed a low tracheotomy on the first bulbo plication indicating broncbial obstruction and atelectasis. spinal case to be treated by Lassen's method in the 1956 The difficulty in detubation which ometimes arises in Cape Town polio epidemic and I must confess the tendency infants \ ho have had a tracheotomy for any length of time of the tube to' slip down the right bronchus required constant is a familiar problem. In the first in tance a laryngo opyand watching. The right-angled tube designed by Crampton bronchoscopy hould be carried out to a certain whether Smith eliminates this hazard, however, and with it I think there is any tenosis or whether granulations are present in this objection to a below-isthmus tracheotomy falls away. the trachea. When such granulations have been encountered If tracheotomy is being performed with a view to inter they have, in my experience, in ariably been found to be mittent-positive-pressure respiration it is necessary to excise a prolapsing into the trachea from the margins of the toma window from the anterior tracheal wall. This should be oval and not arising within the trachea itself. I have found that the in shape with its greatest diameter in the axis of the trachea. most effective way of dealing with these is to remove them If the tracheotomy is for an obstructive lesion or for tracheo under endotracheal anaesthesia with aHartman's granulation-. -

Osteoblastoma of the Trapezoid Bone and Triquetral Bone: Report of Two Cases
CASE REPORT Acta Orthop Traumatol Turc 2013;47(5):376-378 doi:10.3944/AOTT.2013.3081 Osteoblastoma of the trapezoid bone and triquetral bone: report of two cases ‹brahim KAYA1, Burak BOYNUK2, Caner GÜNERBÜYÜK3, Ak›n U⁄RAfi4 1Department of Orthopedics and Traumatology, Haseki Training and Research Hospital, ‹stanbul, Turkey; 2Department of Orthopedics and Traumatology, Bak›rköy Ac›badem Hospital, ‹stanbul, Turkey; 3Department of Orthopedics and Traumatology, 29 May›s Hospital, ‹stanbul, Turkey; 4Department of Orthopedics and Traumatology, ‹stanbul Medipol University, School of Medicine, ‹stanbul, Turkey Osteoblastoma is a benign local aggressive tumor mostly localized in the vertebra or long bones. Carpal location and recurrence are extremely rare. Treatment options include either curettage or wide en bloc resection which causes functional disability in the hand and wrist and should be reserved only for recurrence. We present a case of recurrent trapezoid osteoblastoma previously treated with curet- tage of the trapezoid bone and a case of primary triquetral osteoblastoma. Key words: Curettage; osteoblastoma; trapezoid bone; triquetral bone. Osteoblastoma is a benign primary bone tumor first pain increased at night and had a good response to non- described as “giant osteoid osteoma” by Dahlin and steroidal analgesic drugs. Radiographs, computerized Johnson in 1954.[1] Later, in 1956, Lichtenstein and Jaffe tomography and magnetic resonance imaging (MRI) named this tumor “osteoblastoma” in two different arti- revealed findings resembling avascular necrosis of the cles.[2] It is an uncommon benign but locally aggressive trapezoid bone, periosteal reaction at the second tumor, most commonly located in the vertebral column metacarpal and generalized edema in the dorsal com- or metaphysis of long bones. -

The Structure and Movement of Clarinet Playing D.M.A
The Structure and Movement of Clarinet Playing D.M.A. DOCUMENT Presented in Partial Fulfilment of the Requirements for the Degree Doctor of Musical Arts in the Graduate School of The Ohio State University By Sheri Lynn Rolf, M.D. Graduate Program in Music The Ohio State University 2018 D.M.A. Document Committee: Dr. Caroline A. Hartig, Chair Dr. David Hedgecoth Professor Katherine Borst Jones Dr. Scott McCoy Copyrighted by Sheri Lynn Rolf, M.D. 2018 Abstract The clarinet is a complex instrument that blends wood, metal, and air to create some of the world’s most beautiful sounds. Its most intricate component, however, is the human who is playing it. While the clarinet has 24 tone holes and 17 or 18 keys, the human body has 205 bones, around 700 muscles, and nearly 45 miles of nerves. A seemingly endless number of exercises and etudes are available to improve technique, but almost no one comments on how to best use the body in order to utilize these studies to maximum effect while preventing injury. The purpose of this study is to elucidate the interactions of the clarinet with the body of the person playing it. Emphasis will be placed upon the musculoskeletal system, recognizing that playing the clarinet is an activity that ultimately involves the entire body. Aspects of the skeletal system as they relate to playing the clarinet will be described, beginning with the axial skeleton. The extremities and their musculoskeletal relationships to the clarinet will then be discussed. The muscles responsible for the fine coordinated movements required for successful performance on the clarinet will be described. -

Hand Surgery: a Guide for Medical Students
Hand Surgery: A Guide for Medical Students Trevor Carroll and Margaret Jain MD Table of Contents Trigger Finger 3 Carpal Tunnel Syndrome 13 Basal Joint Arthritis 23 Ganglion Cyst 36 Scaphoid Fracture 43 Cubital Tunnel Syndrome 54 Low Ulnar Nerve Injury 64 Trigger Finger (stenosing tenosynovitis) • Anatomy and Mechanism of Injury • Risk Factors • Symptoms • Physical Exam • Classification • Treatments Trigger Finger: Anatomy and MOI (Thompson and Netter, p191) • The flexor tendons run within the synovial tendinous sheath in the finger • During flexion, the tendons contract, running underneath the pulley system • Overtime, the flexor tendons and/or the A1 pulley can get inflamed during finger flexion. • Occassionally, the flexor tendons and/or the A1 pulley abnormally thicken. This decreases the normal space between these structures necessary for the tendon to smoothly glide • In more severe cases, patients can have their fingers momentarily or permanently locked in flexion usually at the PIP joint (Trigger Finger‐OrthoInfo ) Trigger Finger: Risk Factors • Age: 40‐60 • Female > Male • Repetitive tasks may be related – Computers, machinery • Gout • Rheumatoid arthritis • Diabetes (poor prognostic sign) • Carpal tunnel syndrome (often concurrently) Trigger Finger: Subjective • C/O focal distal palm pain • Pain can radiate proximally in the palm and distally in finger • C/O finger locking, clicking, sticking—often worse during sleep or in the early morning • Sometimes “snapping” during flexion • Can improve throughout the day Trigger Finger: -

Scapholunate Ligament Tear
Scapholunate Ligament Tear Note: These exercises are only to be performed with physician approval. Wrist & Forearm Active ROM Exercises 1 . Wrist Flexion & Extension 2. Wrist Ulnar and Radial Deviation With forearm supported on table and wrist over With hand flat on table, slide hand side. the edge, lift hand up with fingers resting in a Repeat 8 – 10 times, 3 – 4 times per day. fist, and then relax hand down with fingers open. Repeat 8 – 10 times, 3 – 4 times per day. 3 . Forearm Supination and Pronation Keeping elbow bent and close to your side, to side, rotate your hand to turn palm up, and then palm down. It is helpful to use a light hammer or light weighted dowel to perform this exercise Repeat 8 – 10 times, 3 – 4 times per day. 1 Passive Wrist Stretches Use uninvolved hand to gently bend involved wrist downward. Hold a comfortable stretch about 15 seconds. Repeat 8–10 times, 3–4 times per day. Use uninvolved hand to gently bend involved wrist towards the ceiling. Hold a comfortable stretch about 15 seconds. Repeat 8–10 times, 3–4 times per day. Place both hands together in a ‘meditation-like’ position. If you are having a hard time keeping the base of the palms connected, place a card or thin object between both palms and attempt to hold together. Slowly start to increase wrist flexion (wrist bending) by lowering both wrists while maintaining the palms together. The fingers and thumbs should be resting against each other. Hold a comfortable stretch about 15 seconds. -

Capitate-Trapezoid Synostosis: Analysis of an Early Bronze Age Case and Review of the Literature P
Folia Morphol. Vol. 76, No. 2, pp. 149–156 DOI: 10.5603/FM.a2016.0068 R E V I E W A R T I C L E Copyright © 2017 Via Medica ISSN 0015–5659 www.fm.viamedica.pl Capitate-trapezoid synostosis: analysis of an Early Bronze Age case and review of the literature P. Saccheri1, G. Sabbadini2, E. Crivellato1, A. Canci3, F. Toso4, L. Travan1 1Department of Experimental and Clinical Medicine, Section of Anatomy, University of Udine, Italy 2Department of Medical, Surgical and Health Sciences, University of Trieste, Italy 3Department of History and Preservation of the Cultural Heritage, University of Udine, Italy 4Department of Diagnostic Imaging, University Hospital of Udine, Italy [Received: 22 July 2016; Accepted: 2 September 2016] Background: Carpal synostoses are congenital defects characterised by com- plete or incomplete coalition of two or more carpal bones. Although most of these defects are discovered only incidentally, sometimes they become clinically manifest. Among the different types of carpal coalition, the synostosis between capitate and trapezoid bones is quite rare, with only sparse data available in the literature. The aim of this report was to describe a case of capitate-trapezoid synostosis (CTS) observed in an ancient human skeleton, as well as to scrutinise the pertinent literature in order to assess for the characteristics of this type of defect, including its potential relevance to clinical practice. Materials and methods: We studied the skeletal remains of an Early Bronze Age male warrior affected by incomplete CTS. Macroscopic and radiological examina- tion of the defect was carried out. We also performed a comprehensive PubMed search in the Medline and other specialty literature databases to retrieve and analyse data relevant to the subject under consideration. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -
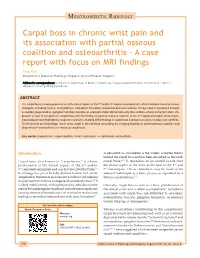
Carpal Boss in Chronic Wrist Pain and Its Association with Partial Osseous
MUSCULOSKELETAL RADIOLOGY Carpal boss in chronic wrist pain and its association with partial osseous coalition and osteoarthritis ‑ A case report with focus on MRI findings Feng Poh Department of Diagnostic Radiology, Singapore General Hospital, Singapore Address for correspondence: Dr. Feng Poh, Department of Diagnostic Radiology, Singapore General Hospital, Outram Road ‑ 168 751, Singapore. E‑mail: [email protected] ABSTRACT The carpal boss is a bony prominence at the dorsal aspect of the 2nd and/or 3rd carpometacarpal joint, which has been linked to various etiologies, including trauma, os styloideum, osteophyte formation, and partial osseous coalition. It may result in symptoms through secondary degeneration, ganglion formation, bursitis, or extensor tendon abnormalities by altered biomechanics of wrist motion. We present a case of symptomatic carpal boss with the finding of a partial osseous coalition at the 2nd carpometacarpal (metacarpal– trapezoid) joint and highlight the magnetic resonance imaging (MRI) findings of carpal boss impingement and secondary osteoarthritis. To the best of our knowledge, there is no report in the literature describing the imaging findings of partial osseous coalition and degenerative osteoarthritis in relation to carpal boss. Key words: Carpal boss; carpal coalition; chronic wrist pain; os styloideum; osteoarthritis Introduction A persistent os styloideum is the widely accepted theory behind the carpal boss and has been described as the ninth Carpal boss, also known as “carpe bossu,” is a bony carpal bone.[4,5] It represents an un‑united ossicle over prominence at the dorsal aspect of the 2nd and/or the dorsal aspect of the wrist at the base of the 2nd and 3rd carpometacarpal joint and was first described by Fiolle.[1] 3rd metacarpals. -

Clinical Orthopedics Advanced Research Journal Case Report Teodonno F, Et Al
1 VolumeVolume 2019; 2018; Issue Issue 01 Clinical Orthopedics Advanced Research Journal Case Report Teodonno F, et al. Clin Ortho Adv Res J: COARJ-100003. Trans-Scaphoid Perilunate Dislocation with Fractured Triquetral Bone in A Pediatric Patient: A 10-Month Follow Up of a Case Report Teodonno F*, Macera A, Crespo Lastras P, Cervero Suárez FJ, Suárez Rueda C and Márquez Ámbite J Department of Orthopedic Surgery and Traumatology, Infanta Elena Hospital, Valdemoro, Madrid, Spain *Corresponding author: Francesca Teodonno, Department of Orthopedic Surgery and Traumatology, Infanta Elena Hospital, Valde- moro, Madrid, Spain, Tel: +34918948410; Email: [email protected] Citation: Francesca Teodonno, et al. (2019) Trans-Scaphoid Perilunate Dislocation with Fractured Triquetral Bone in A Pediatric Pa- tient: A 10-Month Follow Up of a Case Report. Clin Ortho Adv Res J: COARJ-100003. Received date: 28 October, 2019; Accepted date: 04 November, 2019; Published date: 15 November, 2019 Abstract Transcarpal fractures and dislocations in pediatric patients are seldomly reported in literature. Trans-scaphoid dislocations rep- resent only the 1,4% of all scaphoid fractures in the pediatric population.We present the case of 12-year-old boy that, after a fall on the outstretched hand from a motorbike, sustains a trans-scaphoid perilunate dislocation with non displaced fractures of the scaphoid and triquetrum bones, and was treated conservativelythrough closed reduction for the dislocation and immobilization with a closed cast. At final follow up of 10 months, the fractures healed well with a full return of good wrist function. This unusual injury is described so that it may be better acknowledged in the future. -
Comprehensive Anatomy and Physiology for ICD-10-CM and ICD-10-PCS Coding Contents
2016 Optum Learning: Comprehensive Anatomy and Physiology for ICD-10-CM and ICD-10-PCS Coding Contents Introduction ................................................................................................................1 Welcome to Comprehensive Anatomy and Physiology for ICD-10-CM and ICD-10-PCS Coding .....................................................................1 Summary ....................................................................................................11 Chapter 1. Introduction to the Human Body ........................................................13 Anatomy Overview .....................................................................................13 Figure 1.1: Tissue ...................................................................................14 Figure 1.2: Anatomical Position .............................................................17 Figure 1.3: Body Planes ..........................................................................19 Figure 1.4: Motion .................................................................................20 Summary ....................................................................................................21 Knowledge Assessment Questions ..............................................................22 Chapter 2. ICD-10-CM: Integumentary System ....................................................25 Anatomic Overview ....................................................................................25 Figure 2.1: Skin .....................................................................................25