And Inquests Into a Wildfire and the Deaths of Five Firefighters at Linton on 2 December 1998
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
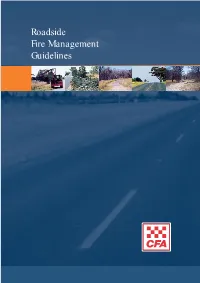
Roadside Fire Management Guidelines Contents CONTENTS
Roadside Fire Management Guidelines contents CONTENTS PART A: INTRODUCTION 2 LEGISLATION 2 ROADSIDE MANAGEMENT PLANNING 3 MUNICIPAL FIRE PREVENTION PLANNING 3 PART B: ROADSIDE FIRE MANAGEMENT 5 OBJECTIVES OF ROADSIDE FIRE MANAGEMENT 5 Objective 1: Prevent Fires on Roadsides 8 Objective 2: Contain Roadside Fires 12 Objective 3: Manage Safety of Road Users 20 Objective 4: Provide Control Lines 24 Objective 5: Recovery From Roadside Fires 27 PART C: ROADSIDE RISK ASSESSMENT PROCESS 29 THE RISK ASSESSMENT PROCESS 29 SUMMARY OF RISK ASSESSMENT PROCESS 29 SELECTING TREATMENT OPTIONS 30 Roadside Reserve Categories 31 ROADSIDE RISK ASSESSMENT WORKSHEET 32 PART D: APPENDICES 34 Appendix 1: CFA Regions 34 Appendix 2: Glossary of Terms 35 REFERENCES 37 ACKNOWLEDGEMENTS These guidelines have been developed by the Country Fire Authority Victoria (CFA), after consultation with the Rural and Urban Fire Brigades Associations, Department of Natural Resources and Environment (DNRE), VicRoads and the Municipal Association of Victoria (MAV). Roadside Fire Management Guidelines 1 PART A part a INTRODUCTION Traditionally, roadsides have been used extensively for the implementation of fire prevention programs. With changes in land and resource management and a shift to risk based emergency management, there is a need to review fire prevention on roadsides to keep pace INTRODUCTION with community expectations and ensure a consistent approach to fire management. LEGISLATION Conservation values of national significance are protected under the Commonwealth’s Environment -

FIREGROUND RESPONSE 3 Volume II: Fire Preparation, Response and Recovery
FIREGROUND RESPONSE 3 Volume II: Fire Preparation, Response and Recovery 3 FIreground response In the lead-up to 7 February 2009 firefighters took precautionary measures, and when a response was required it was rapid and apt. The preparations of many brigades were exemplary. Some localities pre-positioned firefighting resources in readiness and others responded to nearby districts to support firefighting efforts. The Commission heard evidence of responsive and resourceful activity from firefighters on the day, and it commends their efforts. Many operational systems worked well, particularly considering the weather conditions. There were, however, some areas—such as timely fireground warnings to firefighters and appointing safety officers to incident management teams—where systemic problems emerged. Communications also fell short and this affected the safety of some fire crews caught unexpectedly when the wind changed. Aerial firefighting preparations and dispatch systems did not always provide the required response and need review to make them more responsive. Essential requirements such as access to water and electricity also caused problems. Successful response to a fire relies on a blend of personnel, resources and processes. These include systems for rapid fire detection, deployment of appropriate equipment and personnel to assist suppression, accurate and timely intelligence about fires and weather conditions, and good communication. In addition, robust systems are required to support firefighters on the ground and ensure their safety. Timely and precise information from the firefront is also critical to enable accurate warnings for the community. Given its terms of reference, the Commission focused on Victorian fire management systems, agencies and structures, while recognising that in many cases these are not unique to Victoria. -
Additional Presentation Abstracts Abstracts for the 2010 Human Dimensions of Wildland Fire Conference Proceedings
ADDITIONAL PRESENTATION ABSTRACTS ABSTRACTS FOR THE 2010 HUMAN DIMENSIONS OF WILDLAND FIRE CONFERENCE PROCEEDINGS 1.0 PLENARY SESSIONS 1.1 Australian Response to the Black Saturday Fires: What is and isn’t Changing? Presenters Naomi Brown, Australasian Fire Authorities Council Alan Rhodes, Country Fire Authority Abstract The wildfires of 7 February 2009 in Victoria, Australia, management have been under intense scrutiny and that killed 173 people and destroyed more than 2,000 have been the focus of public debate. The presentation homes shocked the world. The government quickly will provide an overview of the fires, the Royal established a Royal Commission, the highest form of Commission findings, and the implications that flow inquiry possible in Australia, to investigate all aspects from these events. The presentation will also include of the disaster. Both the fires and the proceedings reflection on some fundamental issues that have arisen, of the Royal Commission have significantly altered such as the community’s role in responding to the risk public perceptions of the wildfire risk and how of wildfire and whether agencies and the community agencies need to respond. Key issues such as the can share responsibility for dealing with the risk. “stay or go” approach, warning systems, and incident Proceedings of the Second Conference on the Human Dimensions of Wildland Fire GTR-NRS-P-84 113 1.2 When the Incident doesn’t End: Life in the Grinder (The Experiences of a State Agency Tasked with Managing Multiple Long-Duration Incidents and the Impact on its Personnel) Presenter Mark D. Stanford, Fire Operations Chief, Texas Forest Service Abstract From 2005 through 2009, Texas Forest Service (TFS) for more than 65 percent of the 5-year period. -

CFA Annual Report 2019-20 8 Lakeside Drive, Burwood East Vic 3149 Telephone (03) 9262 8444 Cfa.Vic.Gov.Au
Annual Report 2019–20 All material in this publication is provided under a Creative Commons Attribution 4.0 international licence with the exception of any images, photographs or branding, including CFA and government logos. In some cases a third party may hold copyright in material in this publication and their permission may be required to use the material. See creativecommons.org/licenses/by/4.0. Material obtained from this publication is to be attributed as: © State of Victoria (Country Fire Authority) 2020. Cover photo: Epping Fire Brigade’s Asim Siddiqui 2 Country Fire Authority Annual Report 2019–20 Foreword ........................................................................................................................................................4 Chair’s foreword ....................................................................................................................................................4 From the CEO/Chief Officer ...............................................................................................................................6 CFA Victoria ................................................................................................................................................8 Who we are.............................................................................................................................................................8 CFA’s response to the coronavirus ..................................................................................................................9 -

Reporting Fire in Australia's Forests and Vegetation
Reporting fire in Australia’s forests and vegetation D.J. Walsh, K.E. Rumba, J., Hoare, M. Parsons and R. Thackway April 2007 © Commonwealth of Australia 2007 This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without prior written permission from the Commonwealth. Requests and inquiries concerning reproduction and rights should be addressed to the Commonwealth Copyright Administration, Attorney General’s Department, Robert Garran Offices, National Circuit, Barton ACT 2600 or posted at http://www.ag.gov.au/cca. The Australian Government acting through the Bureau of Rural Sciences has exercised due care and skill in the preparation and compilation of the information and data set out in this publication. Notwithstanding, the Bureau of Rural Sciences, its employees and advisers disclaim all liability, including liability for negligence, for any loss, damage, injury, expense or cost incurred by any person as a result of accessing, using or relying upon any of the information or data set out in this publication to the maximum extent permitted by law. Postal address: Bureau of Rural Sciences GPO Box 858 Canberra, ACT 2601 Copies available from: BRS Publication Sales GPO Box 858 Canberra ACT 2601 Ph: 1800 020 157 Fax: 02 6272 2330 Email: [email protected] Internet: http://www.brs.gov.au Preferred citation: Walsh, D.J., Rumba, K.E., Hoare, J., Parsons, M., and Thackway R. 2006. Reporting Fire in Australia’s Forests and Vegetation. Bureau of Rural Sciences, Canberra. Acknowledgements The first draft of this report was prepared in 2001. -

Tourism Business Fire Ready Kit Introduction
Tourism Business Fire Ready Kit Introduction You may think that a bush or grass fire will never affect your business, and we hope you are right. However, the fact is, Victoria is one of the most fire-prone areas in the world and bushfires occur every summer. If a bushfire starts near your business, you How will a written bushfire plan and your employees may be under pressure help your business? to ensure the safety of yourselves and others. A written plan can: Understanding your risks and responsibilities, and planning what you will do now will help • Save lives by helping you to stay focused you respond in the best possible way. and respond in the best possible way when you’re under pressure. This resource kit has been developed to help • Help to protect your investments and get you understand your local risks, prepare your your business back up and running more business and your employees, identify your quickly after the threat of fire has passed. triggers to act, understand how to inform customers and undertake planning. • Minimise the loss of profits. • Ensure your employees’ needs are accounted for in your planning. “ We did have an emergency bushfire plan in place – one that you think you’re never • Ensure you comply with the Victorian going to use. But, on the day, it actually Occupational Health and Safety Act 2004. worked exceptionally well. • Reduce the anxiety that people may feel on high-risk bushfire days. We found that the procedures we put in place made it easier for us all to know what • Remind you what you need to do every year to do, and certainly in dealing with our to prepare your property, your employees guests as well. -

CFA Annual Report 2001-02
® Annual Report 2002 AnnualReport 2002 CFA Annual Report 2002 CFA Annual Report 2002 Contents Vision and objectives 1 This annual report has been prepared in accordance with the History 5 Financial Management Act 1994 and the Directions of the Minister for Finance. It: CFA profile 6 •provides a record of events, performance, volunteer and career CFA at a glance 7 staff activities; Chairman’s report 8 •reports against CFA’s annual plan 2001/02; Financial summary 10 •informs the Government and public about CFA’s services and Summary of key achievements 15 organisational development during the financial year; Achievements against 2001/02 annual plan 17 • acknowledges the support of CFA people; and Year in review 37 • demonstrates how CFA’s vision and the expected community CFA operational regions 42 outcomes for Victoria are being delivered. Area performance 43 Corporate governance 55 Further copies of this annual report may be obtained from CFA, PO Box 701, Mt Waverley, Vic 3149. Telephone: 03-9262 8444. Board members 60 Facsimile: 03-9264 6200. A CD-ROM copy is also available with CFA organisation and senior management 64 printable pages. Medals and awards 65 Auditor-General’s report 70 Glossary 71 Cover photography: Sally Prideaux Top Photo: New recruit - training exercise at Fiskville. Bottom Photo: Volunteers from Cranbourne, Warneet-Blind Bight and Mt Martha Fire Brigades. Training exercise at CFA’s South Eastern Training Ground CFA Annual Report 2002 CFA Annual Report 2002 Our purpose 1 To provide a cost effective fire and emergency service for the people of Victoria. CFA Annual Report 2002 CFA Annual Report 2002 Our vision 2 With our people, volunteers and career firefighters alike, we will strive to create a safe community through best practice and continuous improvement. -
CFA Annual Report 2000-01
Country Fire Authority Annual Report 2001 ™ Contents CFA profile 1 CFA at a glance 1 History 2 Achievement of our Vision and Mission 3 Chairman’s report 4 Authority members 6 CFA organisation and senior management 7 Corporate governance 8 Chief Executive Officer’s report 11 Achievements against 2000/01 Annual Plan 13 Financial summary 19 Operations 22 Community safety 27 CFA people 30 CFA operational regions 36 CFA Area performance 37 Medals awarded 48 Financial statements and appendices 49 Glossary inside back cover This annual report has been prepared in accordance with the Financial Management Act 1994 and the Directions of the Minister for Finance. It: • provides a record of events, performance, volunteer and career staff activities • reports against CFA’s Annual Plan 2000/01 • informs the Government and public about CFA’s services and organisational development during the financial year • acknowledges the support of CFA people • demonstrates how CFA’s vision and the expected community outcomes for Victoria are being delivered. Further copies of this annual report may be obtained from CFA, PO Box 701, Mt Waverley, Vic 3149. Telephone: 03-9262 8444. Facsimile: 03-9264 6200. A copy is also available on CFA’s website: www.cfa.vic.gov.au. CFA profile The Authority is constituted under the Country Fire Authority Act 1958. CFA operates within CFA at a glance … the State Government portfolio of the Minister (as at 30 June 2001) for Police and Emergency Services. As a community service organisation, CFA’s people Brigades Incident management operate as an integrated team of volunteers Brigades 1,228 Total number of incidents 34,908 and career staff, supported by central and Groups 143 Total number of brigade turnouts 61,560 regional infrastructure. -

Challenges to Response Operations of the 2009 Black Saturday Bushfires
Challenges to response operations of the 2009 black Saturday bushfires Dr Richard Oloruntoba [email protected] Newcastle Business School, Faculty of Business & Law, University of Newcastle 1 University Drive, Callaghan, NSW 2308, Australia Abstract The paper summarises operational issues contributing to high mortality during the “Black Saturday” bushfire disaster of 7th February 2009; and highlights emergency and disaster operations management implications. The paper is an outcome of research undertaken as part of a larger PhD project that utilised document and content analysis supplemented with face to face interviews with senior incident commanders. The research found that: poor information and communication, unusual fire behaviour and ambiguous evacuation policy were key challenges in emergency and disaster response operations. Further research into early warning risk communication, situation awareness and evacuation policy and logistics to reduce mortality is required. Keywords: disaster operations; humanitarian operations; humanitarian logistics Introduction Disasters threaten societies everywhere in the world. While there is great variety in the way disaster operations and management is organized in different countries and different parts of the same nation, operational difficulties contributing to mortality and loss often appear to be similar across large scale disaster and emergency response operations. This paper summarises the key challenges to the Victoria State emergency and disaster response operations during the “Black Saturday” bushfires of February 7th, 2009 in Australia in which 173 persons perished (Victoria Bushfires Royal Commission of Enquiry 2009). The rest of the paper is structured as follows: the next section provides a brief overview of key bushfire and emergency operations literature. This is followed by a summary of the history of bushfires in the state of Victoria in Australia. -

Country Fire Authority Regulations 2014
Regulatory Impact Statement Country Fire Authority Regulations 2014 August2014 Prepared forthe Department of Justice by Jaguar Consulting Pty Ltd www.jaguarconsulting.com.au 1 Summary The Country Fire Authority Regulations 2004 (existing regulations) are due to sunset on 26 January 2015. The proposed Country Fire Authority Regulations 2014 (proposed regulations) will replace the existing regulations with limited amendments. Broadly speaking, the content of the existing and proposed regulations can be divided into two parts. Firstly, the regulations cover a wide range of administrative matters in connection with the operation of the Country Fire Authority (CFA or 'the Authority'). Secondly, the regulations prescribe requirements for the fire danger period; also authorising the CFA to charge the prescribed fee for emergency attendances, and to determine and charge fees in connection with services it provides, which fall outside its core fire prevention and suppression functions. Specifically, the regulations broadly contain: 1. Matters relating to the internal management of CFA employees and members These matters include the registration and functioning of brigades including forestry industry brigades; a range of disciplinary processes, such as the establishment of disciplinary offences and penalties, processes for hearings in relation to alleged offences and appeals against findings. They also include provisions for compensation of volunteers for personal injury and/or property losses incurred while undertaking service as a member of the CFA. 2. Matters relating to fire prevention and suppression functions and the ability to charge fees for CFA services These matters include prescribing fire danger period requirements and the issuing of fire prevention notices, while regulations also authorise fees to be charged for the provision of services, including for fire protection, property protection and loss mitigation, road accident rescue and emergency attendances. -

7Th February 2009, Black Saturday Since Then
FSBSC Submission 1596 7th February 2009, Black Saturday Days before Black Saturday A heatwave struck south-eastern Australia in the weeks before 7 February 2009, building on two months of hot, dry conditions. Melbourne endured three days above 43 degrees and the temperature peaked on 30 January at 45.1 degrees, one of the hottest days ever recorded in the city. These temperatures combined with extremely low levels of humidity to create tinder-dry conditions in the Victorian bush. On 6 February, Premier John Brumby issued a public warning that the next day was expected to be the ‘worst day [for fire conditions] in the history of the state’. Black Saturday On the morning of 7 February northwesterly winds in excess of 100 kilometres per hour scoured the state, bringing hot, dry air from Central Australia. The storm helped create almost perfect fire conditions and when the winds brought down powerlines around 11.30am in the Kinglake/Whittlesea area, the resulting sparks ignited the Kilmore East fire. As the day progressed, the size and intensity of the fire increased. In the evening a cool change from the south-west lowered temperatures but raised wind speeds again to more than 100 kilometres per hour. Spot fires, ignited by embers blown ahead of the main blaze, were reported up to 35 kilometres from the fire front. Other fires began across the state in Horsham, Beechworth, Bendigo and Marysville. By evening almost 400 individual fires were burning and Victoria Police had announced the first fatalities. The weeks after The following day, 8 February, the Kilmore East fire and the Murrindindi Mill fire around Marysville merged to create the massive Kinglake fire complex. -

Dear Assistant Clerk Committees INQUIRY INTO the FIREFIGHTERS' PRESUMPTIVE RIGHTS COMPENSATION and FIRE SERVICES L
FSBSC Submission 1595 Dear Assistant Clerk Committees INQUIRY INTO THE FIREFIGHTERS’ PRESUMPTIVE RIGHTS COMPENSATION AND FIRE SERVICES LEGISLATION AMENDMENT (REFORM) BILL 2017 My name is Kenneth (Ken) Houston and I have been with the Country Fire Authority since 1999. I first joined as a Volunteer and then joined as a Career Firefighter in 2001 and maintained my volunteer membership until 2005/2006. Whilst as a Volunteer at Plenty CFA I was trained as a Heavy Rescue Driver/Operator and had responded to many various types of callouts for entrapments as far away as Kinglake West to free critically ill patients from motor vehicles. These incidents first highlighted to me the glaring gaps in response to Motor Vehicle Accidents outside the Metropolitan Fire Brigade area and as such had delayed injured people to be treated at a hospital within the referred to the “Golden Hour”. (The Golden Hour is determined by medical trauma units as giving the increased likelihood of survival). After graduating from CFA Fiskville in May 2001 I was appointed to Springvale Fire Station and was soon transferred to Dandenong Fire Station to be utilised for my Heavy rescue skills for their Heavy Rescue. Since then I have achieved the following; Chief Officer Commendation 2002‐ for reviving a servilely burnt female removed from her burning home and treating her from the scene to Dandenong Hospital with Ambulance crews. Leading Firefighter Promotion 2005 Fire Officer Promotion 2009 Senior Station Officer 2013 Operations Officer Level 2 Qualification 2015. During my time as a Leading Firefighter at Dandenong, Hoppers Crossing and Greenvale I have responded to numerous House Fires, Motor Vehicle accidents, Hazmat Incidents and even a Mc Donald’s Restaurant Fire 2 up (1 Fire Officer & 1 Leading Firefighter or even at as a LFF Dandenong with 1 Firefighter) 1 of 3 FSBSC Submission 1595 Meeting with CFA Chief Officer My Platoon and I were fortunate enough to have a visit from Chief Officer Euan Ferguson back in April, 2015.