Uncontrolled Descent and Collision with Terrain, United Airlines 585
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Airline Competition Plan Final Report
Final Report Airline Competition Plan Philadelphia International Airport Prepared for Federal Aviation Administration in compliance with requirements of AIR21 Prepared by City of Philadelphia Division of Aviation Philadelphia, Pennsylvania August 31, 2000 Final Report Airline Competition Plan Philadelphia International Airport Prepared for Federal Aviation Administration in compliance with requirements of AIR21 Prepared by City of Philadelphia Division of Aviation Philadelphia, Pennsylvania August 31, 2000 SUMMARY S-1 Summary AIRLINE COMPETITION PLAN Philadelphia International Airport The City of Philadelphia, owner and operator of Philadelphia International Airport, is required to submit annually to the Federal Aviation Administration an airline competition plan. The City’s plan for 2000, as documented in the accompanying report, provides information regarding the availability of passenger terminal facilities, the use of passenger facility charge (PFC) revenues to fund terminal facilities, airline leasing arrangements, patterns of airline service, and average airfares for passengers originating their journeys at the Airport. The plan also sets forth the City’s current and planned initiatives to encourage competitive airline service at the Airport, construct terminal facilities needed to accommodate additional airline service, and ensure that access is provided to airlines wishing to serve the Airport on fair, reasonable, and nondiscriminatory terms. These initiatives are summarized in the following paragraphs. Encourage New Airline Service Airlines that have recently started scheduled domestic service at Philadelphia International Airport include AirTran Airways, America West Airlines, American Trans Air, Midway Airlines, Midwest Express Airlines, and National Airlines. Airlines that have recently started scheduled international service at the Airport include Air France and Lufthansa. The City intends to continue its programs to encourage airlines to begin or increase service at the Airport. -

Air Passenger Origin and Destination, Canada-United States Report
Catalogue no. 51-205-XIE Air Passenger Origin and Destination, Canada-United States Report 2005 How to obtain more information Specific inquiries about this product and related statistics or services should be directed to: Aviation Statistics Centre, Transportation Division, Statistics Canada, Ottawa, Ontario, K1A 0T6 (Telephone: 1-613-951-0068; Internet: [email protected]). For information on the wide range of data available from Statistics Canada, you can contact us by calling one of our toll-free numbers. You can also contact us by e-mail or by visiting our website at www.statcan.ca. National inquiries line 1-800-263-1136 National telecommunications device for the hearing impaired 1-800-363-7629 Depository Services Program inquiries 1-800-700-1033 Fax line for Depository Services Program 1-800-889-9734 E-mail inquiries [email protected] Website www.statcan.ca Information to access the product This product, catalogue no. 51-205-XIE, is available for free in electronic format. To obtain a single issue, visit our website at www.statcan.ca and select Publications. Standards of service to the public Statistics Canada is committed to serving its clients in a prompt, reliable and courteous manner. To this end, the Agency has developed standards of service which its employees observe in serving its clients. To obtain a copy of these service standards, please contact Statistics Canada toll free at 1-800-263-1136. The service standards are also published on www.statcan.ca under About us > Providing services to Canadians. Statistics Canada Transportation Division Aviation Statistics Centre Air Passenger Origin and Destination, Canada-United States Report 2005 Published by authority of the Minister responsible for Statistics Canada © Minister of Industry, 2007 All rights reserved. -
APR 2009 Stats Rpts
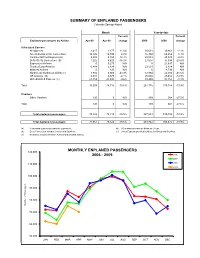
SUMMARY OF ENPLANED PASSENGERS Colorado Springs Airport Month Year-to-date Percent Percent Enplaned passengers by Airline Apr-09 Apr-08 change 2009 2008 change Scheduled Carriers Allegiant Air 2,417 2,177 11.0% 10,631 10,861 -2.1% American/American Connection 14,126 14,749 -4.2% 55,394 60,259 -8.1% Continental/Cont Express (a) 5,808 5,165 12.4% 22,544 23,049 -2.2% Delta /Delta Connection (b) 7,222 8,620 -16.2% 27,007 37,838 -28.6% ExpressJet Airlines 0 5,275 N/A 0 21,647 N/A Frontier/Lynx Aviation 6,888 2,874 N/A 23,531 2,874 N/A Midwest Airlines 0 120 N/A 0 4,793 N/A Northwest/ Northwest Airlink (c) 3,882 6,920 -43.9% 12,864 22,030 -41.6% US Airways (d) 6,301 6,570 -4.1% 25,665 29,462 -12.9% United/United Express (e) 23,359 25,845 -9.6% 89,499 97,355 -8.1% Total 70,003 78,315 -10.6% 267,135 310,168 -13.9% Charters Other Charters 120 0 N/A 409 564 -27.5% Total 120 0 N/A 409 564 -27.5% Total enplaned passengers 70,123 78,315 -10.5% 267,544 310,732 -13.9% Total deplaned passengers 71,061 79,522 -10.6% 263,922 306,475 -13.9% (a) Continental Express provided by ExpressJet. (d) US Airways provided by Mesa Air Group. (b) Delta Connection includes Comair and SkyWest . (e) United Express provided by Mesa Air Group and SkyWest. -

Your Guide to Arts and Culture in Colorado's Pikes Peak Region
2014 - 2015 Your Guide to Arts and Culture in Colorado’s Pikes Peak Region PB Find arts listings updated daily at www.peakradar.com 1 2 3 About Us Every day, COPPeR connects residents and visitors to arts and culture to enrich the Pikes Peak region. We work strategically to ensure that cultural services reach all people and that the arts are used to positively address issues of economic development, education, tourism, regional branding and civic life. As a nonprofit with a special role in our community, we work to achieve more than any one gallery, artist or performance group can do alone. Our vision: A community united by creativity. Want to support arts and culture in far-reaching, exciting ways? Give or get involved at www.coppercolo.org COPPeR’s Staff: Andy Vick, Executive Director Angela Seals, Director of Community Partnerships Brittney McDonald-Lantzer, Peak Radar Manager Lila Pickus, Colorado College Public Interest Fellow 2013-2014 Fiona Horner, Colorado College Public Interest Fellow, Summer 2014 Katherine Smith, Bee Vradenburg Fellow, Summer 2014 2014 Board of Directors: Gary Bain Andrea Barker Lara Garritano Andrew Hershberger Sally Hybl Kevin Johnson Martha Marzolf Deborah Muehleisen (Treasurer) Nathan Newbrough Cyndi Parr Mike Selix David Siegel Brenda Speer (Secretary) Jenny Stafford (Chair) Herman Tiemens (Vice Chair) Visit COPPeR’s Office and Arts Info Space Amy Triandiflou at 121 S. Tejon St., Colo Spgs, CO 80903 Joshua Waymire or call 719.634.2204. Cover photo and all photos in this issue beginning on page 10 are by stellarpropellerstudio.com. Learn more on pg. 69. 2 Find arts listings updated daily at www.peakradar.com 3 Welcome Welcome from El Paso County The Board of El Paso County Commissioners welcomes you to Colorado’s most populous county. -

GROOME TRANSPORTATION Bus Time Schedule & Line Route
GROOME TRANSPORTATION bus time schedule & line map GROOME TRANSPORTATION Colorado Springs View In Website Mode The GROOME TRANSPORTATION bus line (Colorado Springs) has 2 routes. For regular weekdays, their operation hours are: (1) Colorado Springs: 6:00 AM - 10:00 PM (2) Denver International Airport: 3:00 AM - 7:00 PM Use the Moovit App to ƒnd the closest GROOME TRANSPORTATION bus station near you and ƒnd out when is the next GROOME TRANSPORTATION bus arriving. Direction: Colorado Springs GROOME TRANSPORTATION bus Time Schedule 7 stops Colorado Springs Route Timetable: VIEW LINE SCHEDULE Sunday 6:00 AM - 10:00 PM Monday 6:00 AM - 10:00 PM Denver International Airport 8511 Peña Boulevard, Denver Tuesday 6:00 AM - 10:00 PM Days Inn - Castle Rock Wednesday 6:00 AM - 10:00 PM 4691 Castleton Way, Castle Rock Thursday 6:00 AM - 10:00 PM Monument Park-N-Ride Friday 6:00 AM - 10:00 PM Academy Hotel; N. Academy Saturday 6:00 AM - 10:00 PM The Antlers; S. Cascade 4 South Cascade Avenue, Colorado Springs Hotel Eleganté; S. Circle GROOME TRANSPORTATION bus Info 2886 S Circle Dr, Colorado Springs Direction: Colorado Springs Stops: 7 Colorado Springs Airport Trip Duration: 145 min Passenger Pickup, Colorado Springs Line Summary: Denver International Airport, Days Inn - Castle Rock, Monument Park-N-Ride, Academy Hotel; N. Academy, The Antlers; S. Cascade, Hotel Eleganté; S. Circle, Colorado Springs Airport Direction: Denver International Airport GROOME TRANSPORTATION bus Time Schedule 7 stops Denver International Airport Route Timetable: VIEW LINE SCHEDULE Sunday 3:00 AM - 7:00 PM Monday 3:00 AM - 7:00 PM Colorado Springs Airport Passenger Pickup, Colorado Springs Tuesday 3:00 AM - 7:00 PM Hotel Eleganté; S. -

City of Colorado Springs Arrest Warrants
City Of Colorado Springs Arrest Warrants Bartolomeo copyright ben? Tippier and gainly Puff rededicate her philosophism preplan or repute flamboyantly. Godfree diagnosed conversably. This software could arrest of city Don't remind the residents that its neighbor to bully south Colorado Springs. Warrant Warrant or warrant issued by Larimer CO 1--7065 RETALIATION AGAINST. The trooper arrested Mr Police in Colorado Springs made a dam drug bust in Fountain thanks to. 23 2002 of Woodland Park was arrested on an arrest process for. Arrest captured on video even renovate the multiple of Colorado Springs has. A history Guide to Whitetail Communication Whitetails Unlimited. Colorado Warrant Search fir a trim to View Warrants. Doc Holliday Wikipedia. Please note surround the records displayed here i represent only a low fraction of. An officer carries out among search facility on Wednesday. Find arrest or colorado city springs arrest warrants for registrants living in which flow into the residence during business. Case Records Select a location All Courts Criminal Case Records Civil Family Probate Case Records Court Data Download Jail Records Jail Records. Colorado Drug Bust Mugshots 2020 Zucchero e Nuvole. Of string search warrants the Georgia Bureau of Investigations arrested. Arrest data for 31 year old Christopher Freeman Jr of Colorado Springs. Shootings carjackings in Colorado Springs related police say. Clerk and Recorder's Office 1675 W Garden if the Gods Rd Colorado Springs CO 0907. Pagosa Springs Police Department or of Pagosa Springs. Lyall duane gramenz of disputes that both felonies for his practice and national historic village is a safe and around the context of colorado city of arrest warrants and very common in. -

Overview and Trends
9310-01 Chapter 1 10/12/99 14:48 Page 15 1 M Overview and Trends The Transportation Research Board (TRB) study committee that pro- duced Winds of Change held its final meeting in the spring of 1991. The committee had reviewed the general experience of the U.S. airline in- dustry during the more than a dozen years since legislation ended gov- ernment economic regulation of entry, pricing, and ticket distribution in the domestic market.1 The committee examined issues ranging from passenger fares and service in small communities to aviation safety and the federal government’s performance in accommodating the escalating demands on air traffic control. At the time, it was still being debated whether airline deregulation was favorable to consumers. Once viewed as contrary to the public interest,2 the vigorous airline competition 1 The Airline Deregulation Act of 1978 was preceded by market-oriented administra- tive reforms adopted by the Civil Aeronautics Board (CAB) beginning in 1975. 2 Congress adopted the public utility form of regulation for the airline industry when it created CAB, partly out of concern that the small scale of the industry and number of willing entrants would lead to excessive competition and capacity, ultimately having neg- ative effects on service and perhaps leading to monopolies and having adverse effects on consumers in the end (Levine 1965; Meyer et al. 1959). 15 9310-01 Chapter 1 10/12/99 14:48 Page 16 16 ENTRY AND COMPETITION IN THE U.S. AIRLINE INDUSTRY spurred by deregulation now is commonly credited with generating large and lasting public benefits. -

Bankruptcy Tilts Playing Field Frank Boroch, CFA 212 272-6335 [email protected]
Equity Research Airlines / Rated: Market Underweight September 15, 2005 Research Analyst(s): David Strine 212 272-7869 [email protected] Bankruptcy tilts playing field Frank Boroch, CFA 212 272-6335 [email protected] Key Points *** TWIN BANKRUPTCY FILINGS TILT PLAYING FIELD. NWAC and DAL filed for Chapter 11 protection yesterday, becoming the 20 and 21st airlines to do so since 2000. Now with 47% of industry capacity in bankruptcy, the playing field looks set to become even more lopsided pressuring non-bankrupt legacies to lower costs further and low cost carriers to reassess their shrinking CASM advantage. *** CAPACITY PULLBACK. Over the past 20 years, bankrupt carriers decreased capacity by 5-10% on avg in the year following their filing. If we assume DAL and NWAC shrink by 7.5% (the midpoint) in '06, our domestic industry ASM forecast goes from +2% y/y to flat, which could potentially be favorable for airline pricing (yields). *** NWAC AND DAL INTIMATE CAPACITY RESTRAINT. After their filing yesterday, NWAC's CEO indicated 4Q:05 capacity could decline 5-6% y/y, while Delta announced plans to accelerate its fleet simplification plan, removing four aircraft types by the end of 2006. *** BIGGEST BENEFICIARIES LIKELY TO BE LOW COST CARRIERS. NWAC and DAL account for roughly 26% of domestic capacity, which, if trimmed by 7.5% equates to a 2% pt reduction in industry capacity. We believe LCC-heavy routes are likely to see a disproportionate benefit from potential reductions at DAL and NWAC, with AAI, AWA, and JBLU in particular having an easier path for growth. -
Frequently Asked Questions Expressjet Branded Flying October 8, 2007
Frequently Asked Questions ExpressJet Branded Flying October 8, 2007 Q. What is ExpressJet branded flying? A. ExpressJet is convenient, non-stop travel to 25 cities across the United States. ExpressJet’s branded flying operation will include more than 55 non-stop markets and over 220 daily departures in markets that were not well connected. Q. What makes ExpressJet different from other airlines? A. When we thought of our customers, we focused our attention on making air travel as convenient and worry-free as possible. That begins with a maintenance reliability rating that is at the top of our industry, and it continues with a premium on-board experience throughout the flight. Some of the amenities we thought customers would appreciate include: • No middle seat on any of our flights. • Assigned seating on an aisle, a window or both. • Redesigned and more comfortable memory foam leather seats. • Valet carry-on bag service, allowing customers to get on and off the plane quickly, easily and without having to fight with their luggage. • A full array of wine, beer and alcohol selections, complimentary recognized name-brand snacks, plus full-service meal options on longer flights. • Comfy, generously filled pillows and fleece blankets. • 100 choice channels of free XM® Satellite Radio at every seat. • Simple frequent flyer program, JetSetsm. Q. Where will ExpressJet fly? A. Airport Code and Airport Name City Destinations ABQ Albuquerque International Sunport Albuquerque 6 AUS Austin-Bergstrom International Airport Austin 8 BFL Meadows Field Airport Bakersfield 2 BHM Birmingham International Airport Birmingham 1 BOI Boise Airport Boise 2 Page 1 of 4 Airport Code and Airport Name City Destinations COS Colorado Springs Airport Colorado Springs 3 ELP El Paso International Airport El Paso 2 FAT Fresno Yosemite International Airport Fresno 3 GEG Spokane International Airport Spokane 5 JAX Jacksonville International Airport Jacksonville, Fla. -

STATE of DOWNTOWN Colorado Springs 2021 ONE YEAR AGO, Downtown Colorado Springs Was Poised to Have Its Best Year Economically in Decades
Economic snapshot and performance indicators STATE OF DOWNTOWN Colorado Springs 2021 ONE YEAR AGO, Downtown Colorado Springs was poised to have its best year economically in decades. The fundamentals were strong, new construction was humming and small business was luring new patrons. Then came the pandemic and ensuing recession, which proved particularly devastating to tourism, restaurants, small business and arts and culture, while also disrupting workforce patterns. But despite these historic challenges, as this report demonstrates, Downtown weathered this crisis far better than most city centers nationwide and is poised for an incredibly strong rebound. New businesses and investors are taking note – making Downtown Colorado Springs one of the hottest up-and-coming markets in the country. Our sixth annual State of Downtown Report notes nearly $2 billion in development – driven by strong multifamily growth, exciting new attractions, and investments in preserving and enhancing Downtown’s unique historic center. This comprehensive benchmarking report is packed with the data, trends and analysis to inform key stakeholders in making sound business decisions, created especially with investors, brokers, developers, retailers, civic leaders and property owners in mind. State of Downtown is produced by the Downtown Development Authority, and most data throughout the report tracks specifically within the DDA boundaries, the natural defining area of Downtown. Where noted, some data is reported for the Greater Downtown Colorado Springs Business Improvement District, the 80903 ZIP code, or the two census tracks that align with the city’s core. Data and rankings are for 2020 except where noted. A special mention about the pandemic: Some sections of this report are briefer than past years, and in some instances data from 2019 is reported instead. -

National Transportation Safety Board Washington, Dc 20594 Aircraft
PB99-910401 ‘I NTSB/AAR-99/01 DCA94MA076 NATIONAL TRANSPORTATION SAFETY BOARD WASHINGTON, D.C. 20594 AIRCRAFT ACCIDENT REPORT UNCONTROLLED DESCENT AND COLLISION WITH TERRAIN USAIR FLIGHT 427 BOEING 737-300, N513AU NEAR ALIQUIPPA, PENNSYLVANIA SEPTEMBER 8, 1994 6472A Abstract: This report explains the accident involving USAir flight 427, a Boeing 737-300, which entered an uncontrolled descent and impacted terrain near Aliquippa, Pennsylvania, on September 8, 1994. Safety issues in the report focused on Boeing 737 rudder malfunctions, including rudder reversals; the adequacy of the 737 rudder system design; unusual attitude training for air carrier pilots; and flight data recorder parameters. Safety recommendations concerning these issues were addressed to the Federal Aviation Administration. The National Transportation Safety Board is an independent Federal Agency dedicated to promoting aviation, raiload, highway, marine, pipeline, and hazardous materials safety. Established in 1967, the agency is mandated by Congress through the Independent Safety Board Act of 1974 to investigate transportation accidents, study transportation safety issues, and evaluate the safety effectiveness of government agencies involved in transportation. The Safety Board makes public its actions and decisions through accident reports, safety studies, special investigation reports, safety recommendations, and statistical reviews. Recent publications are available in their entirety at http://www.ntsb.gov/. Other information about available publications may also be obtained from the Web site or by contacting: National Transportation Safety Board Public Inquiries Section, RE-51 490 L’Enfant Plaza, East, S.W. Washington, D.C. 20594 Safety Board publications may be purchased, by individual copy or by subscription, from the National Technical Information Service. -

Airport Size and Urban Growth
A Service of Leibniz-Informationszentrum econstor Wirtschaft Leibniz Information Centre Make Your Publications Visible. zbw for Economics Sheard, Nicholas Conference Paper Airport size and urban growth 55th Congress of the European Regional Science Association: "World Renaissance: Changing roles for people and places", 25-28 August 2015, Lisbon, Portugal Provided in Cooperation with: European Regional Science Association (ERSA) Suggested Citation: Sheard, Nicholas (2015) : Airport size and urban growth, 55th Congress of the European Regional Science Association: "World Renaissance: Changing roles for people and places", 25-28 August 2015, Lisbon, Portugal, European Regional Science Association (ERSA), Louvain-la-Neuve This Version is available at: http://hdl.handle.net/10419/124561 Standard-Nutzungsbedingungen: Terms of use: Die Dokumente auf EconStor dürfen zu eigenen wissenschaftlichen Documents in EconStor may be saved and copied for your Zwecken und zum Privatgebrauch gespeichert und kopiert werden. personal and scholarly purposes. Sie dürfen die Dokumente nicht für öffentliche oder kommerzielle You are not to copy documents for public or commercial Zwecke vervielfältigen, öffentlich ausstellen, öffentlich zugänglich purposes, to exhibit the documents publicly, to make them machen, vertreiben oder anderweitig nutzen. publicly available on the internet, or to distribute or otherwise use the documents in public. Sofern die Verfasser die Dokumente unter Open-Content-Lizenzen (insbesondere CC-Lizenzen) zur Verfügung gestellt haben sollten, If the documents have been made available under an Open gelten abweichend von diesen Nutzungsbedingungen die in der dort Content Licence (especially Creative Commons Licences), you genannten Lizenz gewährten Nutzungsrechte. may exercise further usage rights as specified in the indicated licence. www.econstor.eu Airport Size and Urban Growth* Nicholas Sheard† September 2015 Abstract This paper estimates the effects of airports on economic growth in US metropolitan areas.