Neurological Syndromes of Brucellosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
SCIATICA Sciatica Describes Nerve Pain in the Leg That Is Caused by Irritation And/Or Compression of the Sciatic Nerve
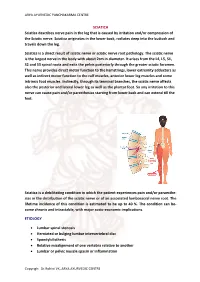
ARYA AYURVEDIC PANCHAKARMA CENTRE SCIATICA Sciatica describes nerve pain in the leg that is caused by irritation and/or compression of the Sciatic nerve. Sciatica originates in the lower back, radiates deep into the buttock and travels down the leg. Sciatica is a direct result of sciatic nerve or sciatic nerve root pathology. The sciatic nerve is the largest nerve in the body with about 2cm in diameter. It arises from the L4, L5, S1, S2 and S3 spinal roots and exits the pelvis posteriorly through the greater sciatic foramen. This nerve provides direct motor function to the hamstrings, lower extremity adductors as well as indirect motor function to the calf muscles, anterior lower leg muscles and some intrinsic foot muscles. Indirectly, through its terminal branches, the sciatic nerve affects also the posterior and lateral lower leg as well as the plantar foot. So any irritation to this nerve can cause pain and/or paresthesias starting from lower back and can extend till the feet. Sciatica is a debilitating condition in which the patient experiences pain and/or paraesthe- sias in the distribution of the sciatic nerve or of an associated lumbosacral nerve root. The lifetime incidence of this condition is estimated to be up to 40 %. The condition can be- come chronic and intractable, with major socio-economic implications. ETIOLOGY • Lumbar spinal stenosis • Herniated or bulging lumbar intervertebral disc • Spondylolisthesis • Relative misalignment of one vertebra relative to another • Lumbar or pelvic muscle spasm or inflammation Copyrigh: Dr.Rohini VK, ARYA AYURVEDIC CENTRE ARYA AYURVEDIC PANCHAKARMA CENTRE • Spinal or Paraspinal masses included malignancy, epidural haematoma or epidural abscess • Lumbar degenerative disc disease • Sacroiliac joint dysfunction EPIDEMIOLOGY GENDER: There appears to be no gender predominance. -

Radiculopathy Vs. Spinal Stenosis: Evocative Electrodiagnosis Identifies the Main Pain Generator
Functional Electromyography Loren M. Fishman · Allen N. Wilkins Functional Electromyography Provocative Maneuvers in Electrodiagnosis 123 Loren M. Fishman, MD Allen N. Wilkins, MD College of Physicians & Surgeons Manhattan Physical Medicine Columbia University and Rehabilitation New York, NY 10028, USA New York, NY 10013, USA [email protected] ISBN 978-1-60761-019-9 e-ISBN 978-1-60761-020-5 DOI 10.1007/978-1-60761-020-5 Springer New York Dordrecht Heidelberg London Library of Congress Control Number: 2010935087 © Springer Science+Business Media, LLC 2011 All rights reserved. This work may not be translated or copied in whole or in part without the written permission of the publisher (Springer Science+Business Media, LLC, 233 Spring Street, New York, NY 10013, USA), except for brief excerpts in connection with reviews or scholarly analysis. Use in connection with any form of information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed is forbidden. The use in this publication of trade names, trademarks, service marks, and similar terms, even if they are not identified as such, is not to be taken as an expression of opinion as to whether or not they are subject to proprietary rights. While the advice and information in this book are believed to be true and accurate at the date of going to press, neither the authors nor the editors nor the publisher can accept any legal responsibility for any errors or omissions that may be made. The publisher makes no warranty, express or implied, with respect to the material contained herein. -

Missouri Hospitalist Missouri Society
MISSOURI HOSPITALIST MISSOURI SOCIETY HOSPITALIST Publisher: Issue 22 October 22, 2009 Division of General IM University of Missouri Hospitalist Update Columbia, Missouri Dealing with Hypertensive Urgencies Syed Ahsan, MD Editor: Robert Folzenlogen MD INTRODUCTION Patients presenting with severe hypertension can often be alarming for house officers and family members. Systolic blood pressures > 180 mm Hg, with or without a diastolic blood pressure >120, have been known to progress to hypertensive emer- Inside this issue: gencies. The majority of complications are related to end organ damage; this may include encephalopa- thy, blurred vision, chest pain, unstable angina, Hospitalist Update acute myocardial infarction and acute renal insuffi- ciency, with or without proteinuria. In the absence of these acute signs, the control of hypertensive urgency remains paramount but is not considered an emergency. Case of the Month The etiology of severe, asymptomatic hypertension is extremely important in defin- ing treatment strategies. The majority of these patients have a prolonged history of uncontrolled hypertension secondary to poor compliance or inadequate treatment From the Journals regimens. Guidelines are not entirely specific in the management of hypertensive ur- gency. ID Corner TREATMENT STRATEGY Based on the current literature, the following approach is recommended: Calendar 1. Confirm that the blood pressure is elevated. The reading should be re- peated in both upper extremities; the physician should ensure that the appropriate cuff size is used and that the readings are consistent. Comments 2. Goal for blood pressure reduction: the ideal goal is to reduce the systolic blood pressure by 20-25% and this should be done over a period of hours to days. -

Adult Onset Still's Disease Accompanied by Acute Respiratory Distress Syndrome: a Case Report
EXPERIMENTAL AND THERAPEUTIC MEDICINE 12: 1817-1821, 2015 Adult onset Still's disease accompanied by acute respiratory distress syndrome: A case report XIAO-TU XI1, MAO‑JIE WANG2, RUN‑YUE HUANG2 and BANG‑HAN DING1 1Emergency Department; 2Rheumatology Department, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine (Guangdong Provincial Hospital of Chinese Medicine), Guangzhou, Guangdong 510006, P.R. China Received July 17, 2015; Accepted May 20, 2016 DOI: 10.3892/etm.2016.3512 Abstract. Adult onset Still's disease (AOSD) is a systemic vascular permeability and a loss of aerated lung tissue (8). inflammatory disorder characterized by rash, leukocytosis, ARDS occurs in 7.2‑38.9/100,000 individuals (9,10), and has fever and arthralgia/arthritis. The most common pulmo- a mortality rate of ~40% (11). Patient mortality varies based nary manifestations associated with AOSD are pulmonary on numerous factors, including age, etiology of the lung injury infiltrates and pleural effusion. The present study describes and non‑pulmonary organ dysfunction. The most common a 40‑year‑old male with AOSD who developed fever, sore risk factors for ARDS are pneumonia, sepsis, aspiration and throat and shortness of breath. Difficulty breathing promptly trauma (11). Multiple predisposing risk factors, in addition to developed, and the patient was diagnosed with acute respira- some secondary factors such as alcohol abuse and obesity, also tory distress syndrome (ARDS). The patient did not respond increase the risk (4). In addition to patient support provided by to antibiotics, including imipenem, vancomycin, fluconazole, improving oxygen delivery to the tissues and preventing multi- moxifloxacin, penicillin, doxycycline and meropenem, but was organ system failure, early recognition and correction of the sensitive to glucocorticoid treatment, including methylpred- underlying cause is important in ARDS treatment. -

Piriformis Syndrome: the Literal “Pain in My Butt” Chelsea Smith, PTA
Piriformis Syndrome: the literal “pain in my butt” Chelsea Smith, PTA Aside from the monotony of day-to-day pains and annoyances, piriformis syndrome is the literal “pain in my butt” that may not go away with sending the kids to grandmas and often takes the form of sciatica. Many individuals with pain in the buttock that radiates down the leg are experiencing a form of sciatica caused by irritation of the spinal nerves in or near the lumbar spine (1). Other times though, the nerve irritation is not in the spine but further down the leg due to a pesky muscle called the piriformis, hence “piriformis syndrome”. The piriformis muscle is a flat, pyramidal-shaped muscle that originates from the front surface of the sacrum and the joint capsule of the sacroiliac joint (SI joint) and is located deep in the gluteal tissue (2). The piriformis travels through the greater sciatic foramen and attaches to the upper surface of the greater trochanter (or top of the hip bone) while the sciatic nerve runs under (and sometimes through) the piriformis muscle as it exits the pelvis. Due to this close proximity between the piriformis muscle and the sciatic nerve, if there is excessive tension (tightness), spasm, or inflammation of the piriformis muscle this can cause irritation to the sciatic nerve leading to symptoms of sciatica (pain down the leg) (1). Activities like sitting on hard surfaces, crouching down, walking or running for long distances, and climbing stairs can all increase symptoms (2) with the most common symptom being tenderness along the piriformis muscle (deep in the gluteal region) upon palpation. -

Malaria History
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site. Copyright 2006, The Johns Hopkins University and David Sullivan. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed. Malariology Overview History, Lifecycle, Epidemiology, Pathology, and Control David Sullivan, MD Malaria History • 2700 BCE: The Nei Ching (Chinese Canon of Medicine) discussed malaria symptoms and the relationship between fevers and enlarged spleens. • 1550 BCE: The Ebers Papyrus mentions fevers, rigors, splenomegaly, and oil from Balantines tree as mosquito repellent. • 6th century BCE: Cuneiform tablets mention deadly malaria-like fevers affecting Mesopotamia. • Hippocrates from studies in Egypt was first to make connection between nearness of stagnant bodies of water and occurrence of fevers in local population. • Romans also associated marshes with fever and pioneered efforts to drain swamps. • Italian: “aria cattiva” = bad air; “mal aria” = bad air. • French: “paludisme” = rooted in swamp. Cure Before Etiology: Mid 17th Century - Three Theories • PC Garnham relates that following: An earthquake caused destruction in Loxa in which many cinchona trees collapsed and fell into small lake or pond and water became very bitter as to be almost undrinkable. Yet an Indian so thirsty with a violent fever quenched his thirst with this cinchona bark contaminated water and was better in a day or two. -

Piriformis Syndrome Is Overdiagnosed 11 Robert A
American Association of Neuromuscular & Electrodiagnostic Medicine AANEM CROSSFIRE: CONTROVERSIES IN NEUROMUSCULAR AND ELECTRODIAGNOSTIC MEDICINE Loren M. Fishman, MD, B.Phil Robert A.Werner, MD, MS Scott J. Primack, DO Willam S. Pease, MD Ernest W. Johnson, MD Lawrence R. Robinson, MD 2005 AANEM COURSE F AANEM 52ND Annual Scientific Meeting Monterey, California CROSSFIRE: Controversies in Neuromuscular and Electrodiagnostic Medicine Loren M. Fishman, MD, B.Phil Robert A.Werner, MD, MS Scott J. Primack, DO Willam S. Pease, MD Ernest W. Johnson, MD Lawrence R. Robinson, MD 2005 COURSE F AANEM 52nd Annual Scientific Meeting Monterey, California AANEM Copyright © September 2005 American Association of Neuromuscular & Electrodiagnostic Medicine 421 First Avenue SW, Suite 300 East Rochester, MN 55902 PRINTED BY JOHNSON PRINTING COMPANY, INC. ii CROSSFIRE: Controversies in Neuromuscular and Electrodiagnostic Medicine Faculty Loren M. Fishman, MD, B.Phil Scott J. Primack, DO Assistant Clinical Professor Co-director Department of Physical Medicine and Rehabilitation Colorado Rehabilitation and Occupational Medicine Columbia College of Physicians and Surgeons Denver, Colorado New York City, New York Dr. Primack completed his residency at the Rehabilitation Institute of Dr. Fishman is a specialist in low back pain and sciatica, electrodiagnosis, Chicago in 1992. He then spent 6 months with Dr. Larry Mack at the functional assessment, and cognitive rehabilitation. Over the last 20 years, University of Washington. Dr. Mack, in conjunction with the Shoulder he has lectured frequently and contributed over 55 publications. His most and Elbow Service at the University of Washington, performed some of the recent work, Relief is in the Stretch: End Back Pain Through Yoga, and the original research utilizing musculoskeletal ultrasound in order to diagnose earlier book, Back Talk, both written with Carol Ardman, were published shoulder pathology. -
A Systematic Review and Meta-Analysis on Chloroquine And
www.nature.com/scientificreports OPEN A systematic review and meta‑analysis on chloroquine and hydroxychloroquine as monotherapy or combined with azithromycin in COVID‑19 treatment Ramy Mohamed Ghazy1, Abdallah Almaghraby2*, Ramy Shaaban3, Ahmed Kamal4, Hatem Beshir5,6, Amr Moursi7, Ahmed Ramadan8 & Sarah Hamed N. Taha9 Many recent studies have investigated the role of either Chloroquine (CQ) or Hydroxychloroquine (HCQ) alone or in combination with azithromycin (AZM) in the management of the emerging coronavirus. This systematic review and meta‑analysis of either published or preprint observational studies or randomized control trials (RCT) aimed to assess mortality rate, duration of hospital stay, need for mechanical ventilation (MV), virologic cure rate (VQR), time to a negative viral polymerase chain reaction (PCR), radiological progression, experiencing drug side efects, and clinical worsening. A search of the online database through June 2020 was performed and examined the reference lists of pertinent articles for in‑vivo studies only. Pooled relative risks (RRs), standard mean diferences of 95% confdence intervals (CIs) were calculated with the random‑efects model. Mortality was not diferent between the standard care (SC) and HCQ groups (RR = 0.99, 95% CI 0.61–1.59, I2 = 82%), meta‑regression analysis proved that mortality was signifcantly diferent across the studies from diferent countries. However, mortality among the HCQ + AZM was signifcantly higher than among the SC (RR = 1.8, 95% CI 1.19–2.27, I2 = 70%). The duration of hospital stay in days was shorter in the SC in comparison with the HCQ group (standard mean diference = 0.57, 95% CI 0.20–0.94, I2 = 92%), or the HCQ + AZM (standard mean diference = 0.77, 95% CI 0.46–1.08, I2 = 81). -

Sciatica and Chronic Pain
Sciatica and Chronic Pain Past, Present and Future Robert W. Baloh 123 Sciatica and Chronic Pain Robert W. Baloh Sciatica and Chronic Pain Past, Present and Future Robert W. Baloh, MD Department of Neurology University of California, Los Angeles Los Angeles, CA, USA ISBN 978-3-319-93903-2 ISBN 978-3-319-93904-9 (eBook) https://doi.org/10.1007/978-3-319-93904-9 Library of Congress Control Number: 2018952076 © Springer International Publishing AG, part of Springer Nature 2019 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors, and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. -

Surgery for Lumbar Radiculopathy/ Sciatica Final Evidence Report
Surgery for Lumbar Radiculopathy/ Sciatica Final evidence report April 13, 2018 Health Technology Assessment Program (HTA) Washington State Health Care Authority PO Box 42712 Olympia, WA 98504-2712 (360) 725-5126 www.hca.wa.gov/hta [email protected] Prepared by: RTI International–University of North Carolina Evidence-based Practice Center Research Triangle Park, NC 27709 www.rti.org This evidence report is based on research conducted by the RTI-UNC Evidence-based Practice Center through a contract between RTI International and the State of Washington Health Care Authority (HCA). The findings and conclusions in this document are those of the authors, who are responsible for its contents. The findings and conclusions do not represent the views of the Washington HCA and no statement in this report should be construed as an official position of Washington HCA. The information in this report is intended to help the State of Washington’s independent Health Technology Clinical Committee make well-informed coverage determinations. This report is not intended to be a substitute for the application of clinical judgment. Anyone who makes decisions concerning the provision of clinical care should consider this report in the same way as any medical reference and in conjunction with all other pertinent information (i.e., in the context of available resources and circumstances presented by individual patients). This document is in the public domain and may be used and reprinted without permission except those copyrighted materials that are clearly noted in the document. Further reproduction of those copyrighted materials is prohibited without the specific permission of copyright holders. -

Lumbosacral Plexus Entrapment Syndrome. Part One: a Common Yet Little-Known Cause of Chronic Pelvic and Lower Extremity Pain
3-A Running head: ANAESTHESIA, PAIN & INTENSIVE CARE www.apicareonline.com ORIGINAL ARTICLE Lumbosacral plexus entrapment syndrome. Part one: A common yet little-known cause of chronic pelvic and lower extremity pain Kjetil Larsen, CES, George C. Chang Chien, D O2 ABSTRACT Corrective exercise specialist, Training & Rehabilitation, Oslo Lumbosacral plexus entrapment syndrome (LPES) is a little-known but common cause Norway of chronic lumbopelvic and lower extremity pain. The lumbar plexus, including the 2 Director of pain management, lumbosacral tunks emerge through the fibers of the psoas major, and the proximal Ventura County Medical Center, sciatic nerve beneath the piriformis muscles. Severe weakness of these muscles may Ventura, CA 93003, USA. lead to entrapment plexopathy, resulting in diffuse and non-specific pain patterns Correspondence: Kjetil Larsen, CES, Corrective throughout the lumbopelvic complex and lower extremities (LPLE), easily mimicking Exercise Specialist, Training & other diagnoses and is therefore likely to mislead the interpreting clinician. It is a Rehabilitation, Oslo Norway; pathology very similar to that of thoracic outlet syndrome, but for the lower body. This Kjetil@trainingandrehabilitation. two part manuscript series was written in an attempt to demonstrate the existence, com; pathophysiology, diagnostic protocol as well as interventional strategy for LPES, and Tel.: +47 975 45 192 its efficacy. Received: 23 November 2018, Reviewed & Accepted: 28 Key words: Pelvic girdle; Pain, Pelvic girdle; Lumbosacral plexus entrapment syndrome; February 2019 Piriformis syndrome; Nerve entrapment; Double-crush; Pain, Chronic; Fibromyalgia Citation: Larsen K, Chien GCC. Lumbosacral plexus entrapment syndrome. Part one: A common yet little-known cause of chronic pelvic and lower extremity pain. -

Overview of Fever of Unknown Origin in Adult and Paediatric Patients L
Overview of fever of unknown origin in adult and paediatric patients L. Attard1, M. Tadolini1, D.U. De Rose2, M. Cattalini2 1Infectious Diseases Unit, Department ABSTRACT been proposed, including removing the of Medical and Surgical Sciences, Alma Fever of unknown origin (FUO) can requirement for in-hospital evaluation Mater Studiorum University of Bologna; be caused by a wide group of dis- due to an increased sophistication of 2Paediatric Clinic, University of Brescia eases, and can include both benign outpatient evaluation. Expansion of the and ASST Spedali Civili di Brescia, Italy. and serious conditions. Since the first definition has also been suggested to Luciano Attard, MD definition of FUO in the early 1960s, include sub-categories of FUO. In par- Marina Tadolini, MD Domenico Umberto De Rose, MD several updates to the definition, di- ticular, in 1991 Durak and Street re-de- Marco Cattalini, MD agnostic and therapeutic approaches fined FUO into four categories: classic Please address correspondence to: have been proposed. This review out- FUO; nosocomial FUO; neutropenic Marina Tadolini, MD, lines a case report of an elderly Ital- FUO; and human immunodeficiency Via Massarenti 11, ian male patient with high fever and virus (HIV)-associated FUO, and pro- 40138 Bologna, Italy. migrating arthralgia who underwent posed three outpatient visits and re- E-mail: [email protected] many procedures and treatments before lated investigations as an alternative to Received on November 27, 2017, accepted a final diagnosis of Adult-onset Still’s “1 week of hospitalisation” (5). on December, 7, 2017. disease was achieved. This case report In 1997, Arnow and Flaherty updated Clin Exp Rheumatol 2018; 36 (Suppl.