Effect of Norian® Crs® Fast Set™ Putty on in Vivo Osseous Repair Using a Critical Size Defect in the Rattus Norvegicus Calvarium
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Paper 2: the Woollen Cloth Industry in the Lim Valley © Richard Bull & Lyme Regis Museum Revised with Extra Images July 2015
Industrial Lyme - Paper 2: The Woollen Cloth Industry in the Lim Valley © Richard Bull & Lyme Regis Museum Revised with extra images July 2015 Like all research, this is on-going. If you know more, or are descended from any of the families involved, please get in touch with the author via Lyme Regis Museum. Summary Woollen cloth has been made in the Lim Valley from at least medieval times, but this paper is more about the factories in Lyme Regis and Uplyme that made high-quality West of England coat cloths. The factories in Lyme were bankrupt in 1847, leaving the Uplyme factory to soldier on against Yorkshire competition until it was destroyed by fire in 1866, whilst being modernised. In Lyme the factories were started up again in the 1850s to make silk thread and hemp twine, but only for a short period; these are the subjects of other papers in this series. This paper contains: the background to the trade, the history of the factories and a walking trail to see the mills. Cloth making – the essential process in a nutshell Sheep fleeces are packed on the farm into big canvas bags called woolsacks. At the factory the fleeces are scoured (washed) to remove lanolin (wool- grease), dirt and adhering vegetable material. Then the fleeces are scribbled (torn up into pieces), combed and carded to produce rovings, long strips of wool ready for spinning. Washed and combed fleece being fed into a carding machine at Coldharbour Mill, Uffculme, Devon Industrial Lyme Paper 2 – The Woollen Cloth Industry © R Bull & Lyme Regis Museum 1 Spinning means to draw out and twist - and by this process the scales of the individual wool fibres lock together to produce a thread known as a single. -

Week 3 the Woollen & Worsted Industries to 1780
Week 3 Dr Frances Richardson frances.richardson@conted. The woollen & ox.ac.uk https://open.conted.ox.ac.uk /series/manufactures- worsted industries industrial-revolution to 1780 Week 2 takeaways • Proto-industrialization theories give us some useful concepts for studying specific pre-factory manufacturing industries • More a framework than a predictive model • Artisan systems did not necessarily develop into putting-out systems • Proto-industry contained the seeds of its own demise • Although factory industrialization often grew out of proto-industry in the same area, some areas de-industrialized and industry spread to new areas • Other factors needed to explain changes, including marketing, industrial relations, and local politics Week 3 outline • Processes in woollen and worsted hand manufacture • Outline history – changing fashions, home demand and exports Wool comber • Organization of the industry in the West Country, Norwich and Yorkshire • How organisation and marketing affected success • How well different regions responded to changing fashion and demand Woollen cloth • Used carded, short-staple wool • Traditional from medieval period, predominated in Tudor exports • Types of cloth - broadcloth, kersey (lighter, less heavily fulled) • Export cloth high and medium quality – limited demand growth • Wool was sorted, willeyed, carded, spun, woven, fulled, finished – could involve raising nap, shearing, pressing, dyeing Broadcloth suit, 1705, VAM Worsted • Used combed, long-staple wool Lincoln longwool sheep • More suited to the Saxony -
Textiles Under Mughals
Chapter V Textiles under Mughals- The advent of the Mughal dynasty gave an undeniable boost to production of the up-market textile, as to other craft. Textiles are singled out for mentioned by Abul Fazl, the minister and biographer of Akbar (1556-1605), in his Ain-i-Akbari, compile in the 1590‟s as a subject in which the emperor took particular interest. Akbar favoured woollen garment – the chosen wear of Sufis (Muslim mystics) – „from his indifference to everything that is worldly‟ in preference to the richer stuffs. His penchant for wool is also indicated by the steps he took to improve shawl manufacture; especially in the relation to dyes and width of fabric.1 Ain-i- Akbari goes into fascinating details on the manner of classifying garments in the imperial wardrobe (toshkhana). The textiles were arranged according to the date of entry which was recorded, sometime with other information, on a label tacked on to the piece (practice which survived in provision toshkhana into the 20th century). Price, colour and weight were also taken into account. Within these boundaries, textile took precedence according to the nature of the day, astrologically auspicious or otherwise on which they were received. A further refinement took into account the colours, of which thirty five are listed in the order of precedence. Abul Fazl further records that imperial workshops had been set up in the cities of Lahore, Agra, Fatehpur Sikri and Ahmedabad, where the best of the local craftsmen were requisitioned to supply the needs of the court.2 Persian masters were brought in to teach improved techniques. -

BED BANK County Is Declared a Disaster Area in Wake of Hurricane
Weather ~" Distribution Fair today; high about 70. BED BANK Today Cloudy tonight, low 60. Chance of rain tomorrow; high, 60s. 16,250 MONDAY THROUGH TttlDAY-EST. Wl See weather and tides page 2, 35 C P E E K VOL. 83, NO. 53 Iisucd Dally, Monday through Friday, entered as Second Clasi Matter RED BANK, N. J., THURSDAY, SEPTEMBER 15, 1960 7c PER COPY R Y S, F R PAGE ONE at the Post OHlce at Red Bank. N. J., under the Act of March 3, 1879. Soviet Attack County Is Declared On Dag Poses A Disaster Area In Crisis for UN Wake of Hurricane UNITED NATIONS, N. Y. (AP)-.The United Nations faced a major crisis today as a result of a slashing Soviet attack on Secre- tary General Dag Hammarskjold and his Congo policies. Officials Inspect Damage, A wide-open break was threatened virtually on the eve ol Soviet Premier Nikita S. Khrushchev's appearance here. The Western powers, led by Ethel Plan U.S., State Aid Bills the United States, prepared to rally to Hammarskjold's sup- Three major developments took place yesterday AF Finds in the aftermath of Hurricane Donna. port in another round of Se- •Is. New curity Council meetings begin- Rep. James C. Auchincloss toured scenes of storm ning this morning on the cha- destruction in the Bayshore, and announced that Mon- otic Congo situation. Missing The Soviet attack, more bitter Threat mouth County has been declared a disaster area, along than any ever made by a big with Atlantic, Cape May and Ocean Counties. -
Types of Dressings This List Is Not All Inclusive
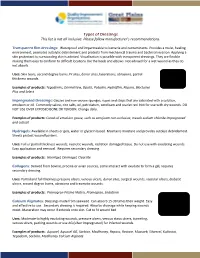
Types of Dressings This list is not all inclusive. Please follow manufacturer’s recommendations. Transparent film dressings: Waterproof and impermeable to bacteria and contaminants. Provides a moist, healing environment, promotes autolytic debridement and protects from mechanical trauma and bacterial invasion. Applying a skin protectant to surrounding skin is advised. Visualization is possible with transparent dressings. They are flexible making them easy to conform to difficult locations like the heels and elbows. Not advised for a wet wound as they do not absorb. Uses: Skin tears, second degree burns, IV sites, donor sites, lacerations, abrasions, partial thickness wounds. Examples of products: Tegaderms, DermaView, Opsite, Polyskin, Hydrofilm, Repara, Bioclusive Plus and Select Impregnated Dressings: Gauzes and non-woven sponges, ropes and strips that are saturated with a solution, emulsion or oil. Commonly saline, zinc salts, oil, petrolatum, xerofoam and scarlet red. Not for use with dry wounds. DO NOT USE OVER EXPOSED BONE OR TENDON. Change daily. Examples of products: Curad oil emulsion gauze, such as xerofoam non-occlusive, mesalt sodium chloride impregnated and cuticell Hydrogels: Available in sheets or gels, water or glycerin based. Maintains moisture and provides autolyic debridement. Sheets protect wound borders. Uses: Full or partial thickness wounds, necrotic wounds, radiation damaged tissue. Do not use with exudating wounds. Easy application and removal. Requires secondary dressing. Examples of products: Normlgel, Dermagel, Clearsite Collagens: Derived from bovine, procine or avian sources, some interact with exudate to form a gel, requires secondary dressing. Uses: Partial and full thickness pressure ulcers, venous ulcers, donor sites, surgical wounds, vascular ulcers, diabetic ulcers, second degree burns, abrasions and traumatic wounds. -

A Clinical Study Comparing Helicoll with Scarlet Red & Opsite in The
A Clinical Study Comparing Helicoll with Scarlet Red & Opsite in the Treatment of Split Thickness Skin Graft Donor Site Article Type: Manuscript Institution where the Clinical Study was performed: Shriners Burn Hospital 815 Market Street, Galveston, TX 77550-2725 Authors: Prema Dhanraj, MD; Iman AL-Haj, MD,FRCS; David Chinkes, PhD; Steven March, RN,BS; David Herndon, MD,FACS; Robert McCauley, MD Abstract: Split thickness skin graft (STSG) is a key method in the reconstructive ladder for covering skin defects utilized widely by surgeons from all specialties. The donor site is often a source of delayed healing, associated with considerable pain and discomfort even more than the recipient wound. Various methods are used for dressing of split thickness skin graft donor sites, unfortunately many of these techniques have the potential for contributing to pain, delayed healing, interference with ambulation and scarring. The aim of this prospective randomized controlled study was to compare Helicoll®, a type I pure collagen dressing, to Opsite® dressing and to Scarlet Red® dressing in the treatment of standardized split thickness skin graft donor sites. Thirty patients, over a 3-month period, underwent various reconstructive procedures, necessitating the use of split thickness skin grafts. Analysis of data: donor site pain, healing time of the donor site, initial absorption of the applied dressing and rate of infection with the three different dressings form the basis of this paper. Results: Patients in the Helicoll group reported significantly less pain and required no dressing change. The infection rate of the donor site in this group was less when compared with the Opsite or the Scarlet red groups. -

INDIAN TRADE BLANKETS in the PACIFIC NORTHWEST History and Symbolism of a Unique North American Tradition by W
WashingtonHistory.org INDIAN TRADE BLANKETS IN THE PACIFIC NORTHWEST History and Symbolism of a Unique North American Tradition By W. R. Swagerty COLUMBIA The Magazine of Northwest History, Summer 2002: Vol. 16, No. 2 To lovers of the picturesque it is a source of keen regret that the Blanket Indian, the most striking and conspicuous figure this country has ever produced, is passing. And by this I mean the Indian who formerly wore a red blanket, a beaded buckskin shirt and leggins, a gorgeous war bonnet, and who painted his face, his hands and his horse in a manner wonderful to behold. Block Quote —G. O. Shields from Blanket Indians of the Northwest, 1921 A veteran of the Indian wars, Shields, like many of his contemporaries, was convinced that the American Indian was a "vanishing race," a victim of "Progress" and the inevitable sweep of Western civilization over a once-proud people now reservation-bound and without the warrior heroes of yesteryear. Red Cloud, Sitting Bull, American Horse, Geronimo, and Chief JosePh— "The Noblest Roman of Them All"—were all gone, rePlaced by a generation of hunters-turned- farmers, and Poor ones at that. Had Shields looked carefully he would have seen many "blanket Indians" at powwows, giveaways, potlatches, funerals, saints' days, parades, rodeos, and in more traditional households on and off reservations. Writing in 1933, Luther Standing Bear, a notable Sioux, reminisced in his autobiography, Land of the Spotted Eagle: Many an Indian has accomplished his own personal salvation by "going back to the blanket." The Indian blanket or buffalo robe, a true American garment and worn with the significance of language; covered beneath it, is the prototype of the American Indian, one of the bravest attempts ever made by man on this continent to rise to the heights of true humanity. -

'Dark Side': Colour Changes in Flemish Luxury Woollens, 1300
Munich Personal RePEc Archive The anti-red shift – to the ’Dark Side’: Colour changes in Flemish luxury woollens, 1300 - 1550 Munro, John H. Department of Economics, University of Toronto June 2006 Online at https://mpra.ub.uni-muenchen.de/10876/ MPRA Paper No. 10876, posted 03 Oct 2008 01:09 UTC Medieval Clothing and Textiles Volume 3 Medieval Clothing and Textiles ISSN 1744–5787 General Editors Robin Netherton St. Louis, Missouri, USA Gale R. Owen-Crocker University of Manchester, England Editorial Board Miranda Howard Western Michigan University, USA John Hines Cardiff University, Wales Kay Lacey Swindon, England John H. Munro University of Toronto, Ontario, Canada M. A. Nordtorp-Madson University of St. Thomas, Minnesota, USA Frances Pritchard Whitworth Art Gallery, Manchester, England Monica L. Wright Middle Tennessee State University, USA Medieval Clothing and Textiles Volume 3 edited by ROBIN NETHERTON GALE R. OWEN-CROCKER THE BOYDELL PRESS © Contributors 2007 All Rights Reserved. Except as permitted under current legislation no part of this work may be photocopied, stored in a retrieval system, published, performed in public, adapted, broadcast, transmitted, recorded or reproduced in any form or by any means, without the prior permission of the copyright owner First published 2007 The Boydell Press, Woodbridge ISBN 1 84383 291 7 ISBN 978 1 84383 291 1 The Boydell Press is an imprint of Boydell & Brewer Ltd PO Box 9, Woodbridge, Suffolk IP12 3DF, UK and of Boydell & Brewer Inc. 668 Mt Hope Avenue, Rochester, NY 14620, USA website: -

A Comparative Study of Daboya (Ghana) and Abeokuta (Nigeria) Local Dyeing
A COMPARATIVE STUDY OF DABOYA (GHANA) AND ABEOKUTA (NIGERIA) LOCAL DYEING By Sherifatu Abas (B.A. Integrated Rural Art and Industry) A thesis submitted to the school of graduate studies, Kwame Nkrumah University of Science and Technology Kumasi, In partial fulfilment of the requirements for the degree of MASTER OF PHILOSOPHY IN INTEGRATED ART Faculty of Art College of Art and Built Environment September, 2014 © 2014 Department of Integrated Rural Art and Industry DECLARATION I declare that this research work is my own work towards the master of philosophy degree in Integrated Art and Industry and that to the best of my knowledge; it contains no materials previously published by another person, nor materials which has been accepted for the award of any other degree of the university, except where due acknowledgement has been made in the text. Abas Sherifatu (PG8357612) …………………….. .………………… (Student‟s Name and & ID No.) Signature Date Certified by: Dr. Abraham Ekow Asmah ..….……………........ …………………. (Supervisor‟s) Signature Date Certified by: Dr. Rudolf Steiner` ….………………….. …………………. (Head of Department) Signature Date ii ACKNOWLEDGEMENT My sincere and heartfelt gratitude goes to the Almighty Allah for the strength and guidance bestowed on me to make this project a success. My profound appreciation goes to the entire staff of the Department of Integrated Rural Art and industry for immeasurable imparting knowledge, offering advice and providing research direction. My sincere gratitude goes to Dr Abraham Ekow Asmah who did not only supervise this piece of work, but also showered me fatherly love and understanding. My special thanks go also to Dr John Osei Bobie Boahin and Dr Vincentia Okpattah for their knowledge and constructive criticism. -

Luxury Textile Imports in Eastern Africa, C. 1800–1885
Textile History ISSN: 0040-4969 (Print) 1743-2952 (Online) Journal homepage: https://www.tandfonline.com/loi/ytex20 ‘Cloths with Names’: Luxury Textile Imports in Eastern Africa, c. 1800–1885 Sarah Fee To cite this article: Sarah Fee (2017) ‘Cloths with Names’: Luxury Textile Imports in Eastern Africa, c. 1800–1885, Textile History, 48:1, 49-84, DOI: 10.1080/00404969.2017.1294819 To link to this article: https://doi.org/10.1080/00404969.2017.1294819 Published online: 10 May 2017. Submit your article to this journal Article views: 341 View related articles View Crossmark data Citing articles: 2 View citing articles Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=ytex20 Textile History, 48 (1), 49–84, May 2017 ‘Cloths with Names’: Luxury Textile Imports in Eastern Africa, c. 1800–1885 Sarah Fee In the nineteenth century, a vast area of eastern Africa stretching the length of the coast and into the reaches of the Congo River was connected by long-distance trade mostly channelled through the Omani commercial empire based in Zanzibar. As studies have recently shown, a critical factor driving trade in this zone was local demand for foreign cloth; from the 1830s the majority of it was industrially made coarse cotton sheeting from Europe and America, which largely displaced the handwoven Indian originals. Employing archival, object, image and field research, this article demonstrates that until 1885 luxury textiles were as important to economic and social life in central eastern Africa, textiles known to the Swahili as ‘cloths with names’. -

Chapter 4: History of the Industrial Stroud Valleys
DRAFT CONSERVATION AREA STATEMENT – INDUSTRIAL HERITAGE CONSERVATION AREA: VOLUME 1 - HISTORY OF THE INDUSTRIAL STROUD VALLEYS - Industry has been a part of our local environment for a thousand years, but it is the Stroud Valleys’ legacy as one of the country’s earliest cloth-making areas that has made it unique. It is a legacy which can be traced back at least as far as the 14 th century. This industrial heritage has helped to shape almost every part of the local environment; its influence can be spotted in quite unexpected places. Many mills have since diversified to other industries, and textile manufacture has virtually disappeared in the locality. However, a rich built heritage of former mills, associated buildings and the transport infrastructure (canals, roads and railways) remains. Analysis: History of the industrial Stroud valleys page 38 DRAFT CONSERVATION AREA STATEMENT – INDUSTRIAL HERITAGE CONSERVATION AREA: VOLUME 1 HISTORY OF THE INDUSTRIAL STROUD VALLEYS 4.1 Settlement in the Stroud valleys can be traced 4.6 Throughout the Stroud valleys, small, back thousands of years into pre-history: compact communities grew up around ancient sites such the Crackstone near ancient river crossing points . The names of Minchinhampton and Hetty Peglar's Tump at Ryeford and Chalford indicate that the Uley are among the obvious visible signs of crossings were originally fords and occupation, however less tangible survivals Dudbridge, Wallbridge and Bowbridge reveal criss-cross the hills and valleys – many of the that they were later superseded by bridges. lanes and tracks used by Neolithic man are still in use today. 4.7 In the narrow river valleys, the points at which the hillsides on either side could be 4.2 Having overcome resistance from the local negotiated by packhorses often dictated the Celtic tribe, the Dobunni, Romans settled in placing of the crossings. -

Designer and Modernist
DESIGNER AND MODERNIST THE IMPACT AND INFLUENCE OF LINEN DESIGN ON THE WORK OF COLIN MIDDLETON One volume DICKON HALL School of Art and Design of Ulster University Ph.D. March 2019 I confirm that the word count of this thesis is less than 100,000 words. i TABLE OF CONTENTS Acknowledgements ii Abstract iii Abbreviations iv Timeline – 1870-1945 1946-1985 Introduction 1 Chapter One – Charles Collins Middleton 45 Chapter Two, Part One – John Hewitt 79 Chapter Two, Part Two – John Hewitt (continued) 112 Chapter Three – John Middleton Murry 149 Chapter Four – Victor Waddington 180 Chapter Five – Colin Middleton 220 Conclusion 263 Bibliography 272 ii ACKNOWLEDGEMENTS I would like to thank my supervisors, Professor Karen Fleming and Dr Joseph McBrinn, for their support, advice and encouragement throughout the research and writing of this PhD thesis, as well as Dr Justin Magee and many other staff at Ulster University for their guidance and assistance at every stage. I am very grateful to Kim Mawhinney for giving me such generous access to the Colin Middleton Archive held by NMNI and also to their collection of his works, and to her colleagues at the Ulster Museum, Anne Stewart, Anna Liesching and Mary Dornan, who have been so helpful. I would also like to acknowledge the Deputy Keeper of the Records, the Public Record Office of Northern Ireland. Many other people have kindly assisted with my research in various ways and I would like to thank them and to apologise to any whom I have inadvertently left out: Nelson Bell, Terry Boyd, John Breakey, David Britton and Karen Reihill, Anne de Buck, Chris Caldwell, Professor Mike Catto, Dr Riann Coulter, David Foster, Dr Brian Kennedy, Sean Kissane, Dr Paul Larmour, David Lennon, Linda Logue, Emer Lynch, Eamonn Mallie, Charlie Minter, Shelagh Parkes, Dr Jackie Reilly, Alison Smith, Claire Walsh and Ian Whyte.