Application Forms: Canada (PDF)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Better Tomorrow, Together
RESPECT | MANNERS | TRY YOUR BEST A BETTER TOMORROW, TOGETHER. ANNUAL REPORT 2019–2020 CONTENTS MESSAGES StEP 05 The Chair, KCS Board of Governors 38 Growing Entrepreneurship StEP by StEP The Head of School EARLY LEARNING PROGRAM STORIES 40 Curriculum Night 2019 09 Our Journey Continues at KCS Senior School Re-Entry Task Force KCS At-Home Learning Program 4 DOORS HIGHLIGHTS 42 Academics We are a resilient, positive school community, ALUMNI Arts committed to overcoming challenges, while always Athletics 15 Alumni in Action Citizenship keeping an eye on the future. KCS Working Committee 20th Year Reunion Alumni Milestones GRADS Our staff, students, parents and Our Four Doors to Learning program inspires 57 Messages from 2020 Valedictorians alumni are united in ensuring the our students to find their passions in the areas of SPECIAL EVENTS academics, arts, athletics and citizenship. We are a sustainability of KCS, even in the leader among independent schools around well- 20 Welcome Back BBQ FINANCIALS most difficult times, just as we have being for students and staff. Widespread student Humbertown Park leadership, extensive engagement in service, Orange Shirt Day 60 2019–2020 Financial Report always done for the past 32 years. student-led entrepreneurship, coding and notable Terry Fox Run student growth, as learners, artists, athletes and Town Halls citizens fuels our passionate community. Grandparents and Special Friends Day PARENT NETWORK Embrace learning, think flexibly, take responsible risks, and make the Together, we are responding to our changing, 62 Updates world better are four of our twenty- uncertain times with flexibility, optimism, empathy SPEAKERS & AUTHORS Key Highlights and cohesiveness. -

Family Handbook 2016-2017
Kingsway College School Family Handbook 2016-2017 TABLE OF CONTENTS OUR MISSION ...................................................................................................................................................................3 SCHOOL PRAYER ...............................................................................................................................................................3 WELCOME TO KINGSWAY COLLEGE SCHOOL .......................................................................................................................3 A GUIDE TO UNDERSTANDING THE ORGANIZATIONAL STRUCTURE AT KCS ............................................................................3 COMMUNICATION AT KCS .................................................................................................................................................7 KNOWING WHAT MATTERS IN LIFE: KCS HABITS OF MIND, BODY AND ACTION ......................................................................8 KINGSWAY COLLEGE SCHOOL CODE OF BEHAVIOUR ............................................................................................................9 DRESS CODE .................................................................................................................................................................. 10 KCS UNIFORM ............................................................................................................................................................... 11 STUDENT BILLING ......................................................................................................................................................... -

Grade 12 Information Night
2018‐09‐25 The Student’s Role Post-secondary research before finalizing university application Visit University/College Campuses Kingsway College Meet all deadlines and read all correspondence Check application status with OUAC or Universities Ensure documents & non-academic requirements Grade 12 received by university (any grades for courses Information Night taken outside of day school, TOEFL results etc.) Have a back-up plan Discuss paying for university with family (ie, parents, caregivers, etc.) Apply for OSAP/Scholarships Are you eligible for College/University entrance? It is YOUR responsibility to ensure that: 1. You have requirements to graduate 2. You have the pre-requisites for the programs you are applying for 1 2018‐09‐25 Are you eligible for Ontario Scholar College/University entrance? A student may be designated an Ontario Scholar if he or she ● It is your responsibility as a student to research satisfies both of the following requirements: Obtains an aggregate of at least 480 marks in any combination of the minimum mark and prerequisite ministry‐approved courses providing a total of six credits requirements for each program you apply for. Recommended by the school principal for the Ontario Secondary School Diploma (OSSD) Ministry-approved courses ● It is your responsibility as a student to be in any Grade 12 university preparation, university/college regular consultation with your teachers during preparation, college preparation, workplace preparation, and/or formative assessments to find out what you open courses authorized under OSS, including locally developed have to do to attain the required averages for courses approved by the ministry your summative assessments. -
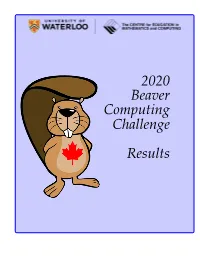
2020 Beaver Computing Challenge Results
2020 Beaver Computing Challenge Results Statistics Overall Statistics for Grade 5/6 Number of competitors: 4727 Overall average score: 44.51 Standard deviation: 13.44 Overall percentage score: 74.18 Averages by question Bear Selection: 5.72/6 Moving Packages: 2.75/5 Museum Tour: 2.90/4 Bowls: 4.44/6 Skyline: 3.03/5 Weighing Boxes: 2.83/4 Bird Watching: 4.73/6 Market Exchange: 3.94/5 Jumping Kangaroo: 3.17/4 Rare Mushrooms: 4.55/6 Beaver Homes: 4.00/5 Theatre Performance: 2.58/4 2 Statistics Overall Statistics for Grade 7/8 Number of competitors: 6368 Overall average score: 64.18 Standard deviation: 15.93 Overall percentage score: 71.31 Averages by question Skyline: 5.69/8 Library Books: 4.25/6 Spider Car: 1.88/4 Crypto Keys: 7.66/8 Market Exchange: 5.39/6 Puzzle Pieces: 2.83/4 Cookies: 7.61/8 House Painting: 4.02/6 Spreading the News: 1.34/4 Connect the Dots: 6.20/8 Treasure Hunt: 4.65/6 Book Organizer: 3.18/4 Towns and Highways: 2.37/8 Water Bottles: 4.48/6 Train Trip: 2.72/4 3 Statistics Overall Statistics for Grade 9/10 Number of competitors: 4373 Overall average score: 60.65 Standard deviation: 16.13 Overall percentage score: 67.39 Averages by question Skyline: 6.49/8 Beaver Intelligence Agency: 3.19/6 Craft: 0.48/4 Library Books: 6.08/8 Mountain Climber: 3.27/6 Vegetable Shipment: 2.05/4 Locked Chests: 6.39/8 Image Scanner: 4.21/6 DNA Sequence: 2.07/4 Water Bottles: 6.48/8 Household Appliances: 4.37/6 Mixed Results: 1.97/4 Ancient Texts: 7.56/8 Puzzle Pieces: 4.67/6 Nine Marbles: 1.52/4 4 Honour Roll for Grade 5/6 Each section is sorted by Last Name. -

Canadian Union Messenger Vol
41..1 • ki t • **4, Canadian Union Messenger Vol. 10 No. 21 October 30, 1971 Ingathering Special "Just Like Being in Heaven" . Report on Canadian Union Bible Conference E. HILLOCK, Youth Director, Canadian Union Conference "It was just like being in heaven," commented one of the Answer, spoke on the promises of God and how these can be young people at the Canadian Union Bible Conference at realized in one's life. He suggested that all in attendance at Camp Ames, Manitoba, Thanksgiving weekend. This remark the Bible Conference plan a reunion in the New Jerusalem. came at the conclusion of a session in which favourite prom- Plans were made to pray for one another that this would be- ises from the Bible had been shared with one another. Others come a reality. said, "Today I decided to become a follower of Christ." "A In an early morning meeting, Ontario-Quebec Conference month and two days ago I accepted Christ." "God is real. He Youth Director, Don Aldridge, directed the youth to the Source is a person and I want to get to heaven." "You know, many of Power. Lloyd Janzen, Manitoba-Saskatchewan Youth Di- of those young people believe that the coming of Christ is rector, led in periods of singspiration throughout the program. soon." "I recommend Him to everybody." "When I gave my Previous to the celebration of the ordinances in the final meet- heart to Him He helped me to live a wonderful life." One ing, Arnold White, Youth Director of the Alberta Conference, camper expressed her joy in knowing Jesus by saying, "This directed the minds of the youth to the experience of the Pass- is the only way to happiness." And so it went as one after over, showing its relationship to Jesus as the Passover lamb another told of how happy he was in experiencing fellowship and to the Lord's supper. -

A CENTURY of ADVENTIST EDUCATION the Spotlight Here and There On
Canadian Union Messenger vol. 41, No. 21, October 30, 1972 A CENTURY OF ADVENTIST EDUCATION The Spotlight Here and There on The Basis By P. W. MANUEL of Executive Secretary Department of Education True Education Canadian Union Conference Centuries ago as a group of students discussed the current begins in the home at birth. Gradually, a mother teaches her educational philosophies for happy, successful living, they had child to express love to her, then to others in the family as the difficulty in agreeing on which was the most important. A young child learns to know them, and to God, the source of all love. lawyer in the group presented the question to the greatest It must be a loving, personal relationship with people the child Teacher of all time who gave the secret in three words "Thou knows. shalt love . ." "God so loved the world that He gave . ." If we would be Modern educators and doctors all agree that love is an im- like Him, we must learn to express our love by giving. A child's portant ingredient of life. Dr. Harold Shyrock says, "Love is natural instinctive reaction is to "get". He must be allowed and uniquely important to the well-being of the human personality. encouraged to give gifts. Christian parents want to teach their Without it, personal characteristics do not develop normally". children to know and to love God. They realize that much of He goes on to differentiate between "love received", and "love the education in the world today is based on selfish desires to bestowed", and emphasizes that love must be experienced from excel in mental ability, in position, in financial affairs, or in birth and as a child grows older, it is necessary to "experience influence. -

CAT~News a Publication from the Seventh-Day Adventist Church in Canada Office of Education
Volume 6, Issue 1 CANADIAN ADVENTIST TEACHERS’ NEWSLETTER Winter 2012 CAT~news A publication from the Seventh-day Adventist Church in Canada Office of Education THE SPIRIT OF GENEROSITY make-shift tents and sleeping bags in alleys and less Dennis Marshall, General Vice-President/Director of Educa- travelled streets; some live in shelters and other pub- tion lic places; others live unnoticed in your neighborhood. Two thousand years ago a phenomenal A great opportunity awaits you this Christmas to show event took place that would change the love to the needy people living among you. Let the world. The angel Gabriel appeared to a spirit of generosity come alive in your heart today and virgin named Mary living in Nazareth, a take the initial steps to bring joy to someone in des- town in Galilee, and said to her: perate need of your help. In addition or in lieu of “Greetings, you who are highly favored! sharing gifts with those you love, plan to give a gift to The Lord is with you.”...Do not be afraid, a family in need or to a homeless stranger. Mary, you have found favor with God. You will be with child and give birth to a son, and you In this edition of CAT~news, the focus is on the are to give him the name Jesus." (Luke 1:28-31) theme, The Spirit of Generosity, most appropriate for the Christmas season. In the next few pages, you Mary believed the angel and nine months later she will read stories from different schools about their bore a son and named Him Jesus, as she was told. -

Pastors Corner
THE CHURCH AT STUDY PASTORS CORNER MONDAY A variety of Sabbath School classes for each age group meet to pray, Caring and Sharing Ministry (Knitting & Crocheting): 1:30 - 4pm at 61 God gives Christians spiritual gifts, to be used to "build up the fellowship, study and learn more about Jesus. Our children, youth Grandview St. N. Contact 905-723-0267 or [email protected]. and young adult classes are held in the lower levels. church" (1Cor 14:12). And by church, He means us, the believers, the body of Christ. We sometimes tend to think of the church as a building, TUESDAY Season of Prayer Congregation or an entity different than ourselves. But each of us is an invaluable part Pathfinders: 6:30pm regular meeting at CPES. Membership Care and Fellowship Classes of the church. We are the church. So when we see that God intends for Sabbath School Study Classes us to build up the church, He intends for us to build up each other. No WEDNESDAY Special Music Burrell Brothers and Son matter your age, young or old, I encourage you to ask yourself this Prayer Meeting: 7pm in the East Chapel. We will be using the 10 days Mission Spotligt Flowing to Unwatered Lands question: "How can God use me to build up the church?". Remember, of Prayer materials. Week 5 Topic: The Fruit of the Holy Spirit. the church is people. There are many ministries in this church, and you Materials are available at https://www.tendaysofprayer.org Closing Comments and Prayer Ingrid and Glendon Delisser Sabbath School loose offerings will be allocated 50% to S.S. -

News from Sandy Lake Academy Paul Llewellyn, Superintendent Pray 100
Maritime Pulse Page 5 June 2015 Education News From Sandy Lake Academy Paul Llewellyn, Superintendent Pray 100 Chris Dupuis, an alumnus of Sandy Lake Academy, During our Chapel and Prayer Warrior time, we have returned 7 years ago to take the helm at guiding started Pray 100, where our students are praying for the our school to new growth. His vision has brought enrollment to reach 100 next school year. We have seen our school to a place of high educational standard answers to prayer many times at Sandy Lake Academy and in our Conference. Under his leadership, our dorm we know God will answer again! We are asking everyone to Pray 100. Let’s teach the kids how powerful prayer can be! is full and our children are Sandy Lake Academy Offering—April 25 receiving a top- Sandy Lake Academy was the recipient of our Maritime churches’ offering on Sabbath, April 25. A total of $3,015.92 notch education was received! Thank you to each one who generously at Sandy Lake. contributed to this vital ministry for our youth and their One of the families! May God richly bless as we work together to initiatives that prepare our youth for God’s kingdom. Chris has brought Spirit Week—April 20-24 to our school has A different been our new theme was program of hands chosen for each on learning. We day of spirit now offer shop, week. Students home economics, strutted around outdoor living, and in their finest computer design, fashions on Formal Day. that is training our children in the practical arts Tuesday’s of daily living. -

Celebrating 50 Years
WINTER 2013 features Celebrating 50 Years 2 From the Editor BY REMY GUENIN, ‘86 3 President’s Message BY SCOTT BOWES 4 BHSN 50th Reunion BY BEV MATIKO, ‘69 6 2013 Alumni of the Year 7 A Message from Graduation 2013 BY ALICIA DOOKS, ‘13 8 Homecoming Weekend 2013 Gallery 10 Brazil Comes to KC BY REMY GUENIN, ‘86 12 Go Into All Nations BY GREG GRYTE 13 In Memoriam 14 Births & Announcements 15 News & Events 16 2013 Awards Ceremony Brazil comes to Kingsway! Read more on page 10 Don’t Miss Any News! facebook.com/groups/ kingswaycollege twitter.com/kingswayc kingswaycollege.on.ca Interested in receiving Kingsway E-News? Send us your email at [email protected] Please send address changes to: Alumni Relations Kingsway College Road 1200 Leland Road Oshawa, ON L1K 2H4 Office: (905) 433-1144 ext 210 ScanScan oror visitvisit usus atat www.kingswaycollege.on.cawww.kingswaycollege.on.ca [email protected] SUMMER ESL CAMP 2013 - BRA- FROM THE EDITOR BY REMY GUENIN, ‘86 Dear Alumni of Kingsway College, KC team this past summer as the new Fall on campus is, in Development Coordinator. She is re- my opinion, the most sponsible for planning events such as the Editor beautiful time of the Fun(d) Dinner, Alum- ni Golf Tournament, Remy Guenin, ‘86 year. As I contemplate this past year and and Alumni Chapter Assistant Editor think about the jour- Meetings. She will Christina Lister ney that Kingsway also be managing our College is on, I realize Alumni database and what an amazing blessing it is to have this receipting along with school still vibrant and operating in the her many extra-cur- 2013 Alumni Association year 2013. -
Alumni Homecoming 2014
Alumni Homecoming 2014 Heather Bruce, Rachel Aka, Dustin Bruce Cindy & Jeff Adema Class of 1964: Beverly (Lennox) Thorne, John Thorne, Sandra Gallop, Anne Gutman, Vanja Gyllenhammer, Pharolyn (Von Gunten) Perk, Brenda Cheeseman , Annemarie Geissler, Roberta (Crawford) McElmurry Scan or visit us at www.kingswaycollege.on.ca SUMMER ESL CAMP 2013 - BRA- FROM THE EDITOR BY REMY GUENIN, ‘86 Dear Kingsway Alumni, one of our dear alumnae Patricia (Ferreira) It has been a beau- Lopez ‘92. You can read her article on page tiful fall this year in 7. One never knows when a memory will Editor Ontario. The weather come to mind, so be ready with a pen Remy Guenin, ‘86 has been fantastic and and paper or if you are tech savvy a pen the colours spectacu- and tablet to jot down that memory and Co-Editor lar on our beautiful share it with the Kingsway family at large. Christina Lister campus and beyond. Speaking of tablets, the exciting news for There is something this school year has been the addition of about the change of seasons that encour- Dell tablets to the arsenal of tools used for ages reflection upon one’s life. I hope Academic purposes. These tablets have features that as you take a moment from your been placed in students hands and are busy schedule and spend time reading being used in the classroom to enhance 2 From the Editor through this edition of the KC Contact lov- the learning experience. It is by the grace BY REMY GUENIN, ‘86 ingly prepared for you by Christina Lister of God and a dedicated team led by Chris 3 President’s Message and myself, you can reflect on what King- Mortenson that we were able to get these BY SCOTT BOWES sway College has meant to you. -

Canadian Union Messenger for 1968
Canadian Union MESSENGER Volume XXXVII, No. 7 Oshawa, Ontario ,!4 March 20, 1968 Andrews University Offers Advantages of . Association With Those of Rich, Varied Background M. E. ERICKSON, Secretary, Department of Education, Canadian Union One of the great advantages and privileges of a Seventh- emy principals; union and divisional educational secretaries; day Adventist is the opportunity to become acquainted with missionaries; pastors; evangelists; departmental secretaries; all parts of the world through travel, acquaintance with conference presidents and even college presidents. missionaries and other travellers, reports from other coun- Last year Andrews conferred 183 Master's degrees, of tries by means of our publications and Sabbath School which 127 were granted to candidates preparing to teach. mission reports, and by association with folk from other The majority of these are not teaching in Seventh-day parts of the world at our Colleges and Universities. Andrews Adventist schools. The University offers a programme for University has a greater percentage of students coming from the professional preparation of school administrators, super- abroad than any other university, with one exception, in visors of instruction, and school guidance counsellors. the United States. Sixty members of the faculty have foreign The entire world field looks to Andrews for denomina- background or experience. What a great advantage there is tional and secular leaders. A great many ministers and for students at Andrews to associate with these who come teachers as well as others now working in Canada have from such rich and varied backgrounds. received a part of their training at this University. In the classes at Andrews University have been found On Sabbath, April 13, the offering in our churches is for students coming directly from college; elementary and sec- the advancement of the work at Andrews University.