Ajmaline in the Management of Cardiac Arrhythmias
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2D6 Substrates 2D6 Inhibitors 2D6 Inducers
Physician Guidelines: Drugs Metabolized by Cytochrome P450’s 1 2D6 Substrates Acetaminophen Captopril Dextroamphetamine Fluphenazine Methoxyphenamine Paroxetine Tacrine Ajmaline Carteolol Dextromethorphan Fluvoxamine Metoclopramide Perhexiline Tamoxifen Alprenolol Carvedilol Diazinon Galantamine Metoprolol Perphenazine Tamsulosin Amiflamine Cevimeline Dihydrocodeine Guanoxan Mexiletine Phenacetin Thioridazine Amitriptyline Chloropromazine Diltiazem Haloperidol Mianserin Phenformin Timolol Amphetamine Chlorpheniramine Diprafenone Hydrocodone Minaprine Procainamide Tolterodine Amprenavir Chlorpyrifos Dolasetron Ibogaine Mirtazapine Promethazine Tradodone Aprindine Cinnarizine Donepezil Iloperidone Nefazodone Propafenone Tramadol Aripiprazole Citalopram Doxepin Imipramine Nifedipine Propranolol Trimipramine Atomoxetine Clomipramine Encainide Indoramin Nisoldipine Quanoxan Tropisetron Benztropine Clozapine Ethylmorphine Lidocaine Norcodeine Quetiapine Venlafaxine Bisoprolol Codeine Ezlopitant Loratidine Nortriptyline Ranitidine Verapamil Brofaramine Debrisoquine Flecainide Maprotline olanzapine Remoxipride Zotepine Bufuralol Delavirdine Flunarizine Mequitazine Ondansetron Risperidone Zuclopenthixol Bunitrolol Desipramine Fluoxetine Methadone Oxycodone Sertraline Butylamphetamine Dexfenfluramine Fluperlapine Methamphetamine Parathion Sparteine 2D6 Inhibitors Ajmaline Chlorpromazine Diphenhydramine Indinavir Mibefradil Pimozide Terfenadine Amiodarone Cimetidine Doxorubicin Lasoprazole Moclobemide Quinidine Thioridazine Amitriptyline Cisapride -

Pakistan Journal of Scientific and Industrial Research Series B: Biological Sciences
Pakistan Journal of Scientific and Industrial Research Series B: Biological Sciences EDITORIAL BOARD Dr. Shahzad Alam Chief Editor Shagufta Yasmin Iqbal Executive Editor MEMBERS Dr. T. A. Ajith Dr. A. Khanum Prof. E. Miraldi Prof. Dr. T. Toyosaki Amala Institute of Medical Pir Mehr Ali Shah Agriculture Pharmaceutical Biology Section Dept. of Foods and Nutrition Science, Kerala, India University, Rawalpindi, Pakistan Universiity of Siena, Siena, Italy Fukuoka, Japan Dr. S. A. Barlas Prof. Dr. K. Krishnan Dr. G. Müller Dr. S. Vaithianathan Environ. Protection Division The University of Newcastle, Sanofi-Aventis Pharma Frankfurt, Bayer Healthcare, USA Penticton, BC V0H 1Z4, Australia Germany Prof. Dr. Z. Xu Canada Prof. Dr. A. Maqbool Dr. M. Murkovic Chinese Academy of Sciences, China Dr. A. Bukhari University of Veterinary and Graz University of Technology, Austria Prof. Dr. X. Yang Bahauddin Zakariya University Animal Sciences, Dr. J. S. Sangha Kunming Medical University, China Multan, Pakistan Lahore, Pakistan Dalhousie University Truro, Canada Dr. V. Zambare Prof. M. J. Jaskani Dr. S. Mathews Dr. H. Shimoda Centre for Bioprocessing University of Agriculture, Pharmacology, The University Oryza Oil & Fat Chemical Co. Ltd., Research and Development, Faisalabad, Pakistan of Sydney, NSW, Australia Aichi, Japan South Dakota, USA Editors: Shahida Begum, Seema Iqbal and Sajid Ali Pakistan Journal of Scientific and Industrial Research is published triannually into two series: Series A: Physical Sciences [ISSN 2221-6413 (Print); ISSN 2223-2559 (Online)] (appearing as issues of January-April, May-August and September-December) and Series B: Biological Sciences [ISSN 2221-6421 (Print); ISSN 2223-2567 (Online)] (appearing as issues of January-April, May- August and September-December). -

Systematic Review of the Effect of Intravenous Lipid Emulsion Therapy for Non-Local Anesthetics Toxicity
Clinical Toxicology ISSN: 1556-3650 (Print) 1556-9519 (Online) Journal homepage: http://www.tandfonline.com/loi/ictx20 Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity Michael Levine, Robert S. Hoffman, Valéry Lavergne, Christine M. Stork, Andis Graudins, Ryan Chuang, Samuel J. Stellpflug, Martin Morris, Andrea Miller-Nesbitt, Sophie Gosselin & for the Lipid Emulsion Workgroup* To cite this article: Michael Levine, Robert S. Hoffman, Valéry Lavergne, Christine M. Stork, Andis Graudins, Ryan Chuang, Samuel J. Stellpflug, Martin Morris, Andrea Miller-Nesbitt, Sophie Gosselin & for the Lipid Emulsion Workgroup* (2016) Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity, Clinical Toxicology, 54:3, 194-221, DOI: 10.3109/15563650.2015.1126286 To link to this article: http://dx.doi.org/10.3109/15563650.2015.1126286 Published online: 06 Feb 2016. Submit your article to this journal Article views: 692 View related articles View Crossmark data Citing articles: 2 View citing articles Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ictx20 Download by: [UPSTATE Medical University Health Sciences Library] Date: 03 August 2016, At: 08:19 CLINICAL TOXICOLOGY, 2016 VOL. 54, NO. 3, 194–221 http://dx.doi.org/10.3109/15563650.2015.1126286 REVIEW Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity Michael Levinea, Robert S. Hoffmanb, Vale´ry Lavergnec, Christine M. Storkd, Andis Graudinse, Ryan Chuangf, Samuel J. Stellpflugg, Martin Morrish, Andrea Miller-Nesbitth, Sophie Gosselini and for the Lipid Emulsion Workgroup* aDepartment of Emergency Medicine, Section of Medical Toxicology, University of Southern California, Los Angeles, CA, USA; bDivision of Medical Toxicology, Ronald O. -

Organic Chemists of Pre-Independence India: with Special Focus on Natural Products
Indian Journal of History of Science, 53.4 (2018) T108-T114 DOI: 10.16943/ijhs/2018/v53i4/49533 Organic Chemists of Pre-Independence India: With Special Focus on Natural Products D Balasubramanian* (Received 17 May 2018; revised 22 June 2018) Abstract Using materials obtained from plants and animals for medicinal, community and technical purposes has been going on in Indian and other ancient civilizations for millennia. With the introduction of western scientific methods into colonial India, isolating, purifying and determining the chemical structures of the components in these materials, and some understanding of the basis of their action became possible. We focus here on the birth and growth of the chemistry of natural products of medicinal and technical value. We discuss here the roles of three pioneers in organic chemistry who started their work in colonial India and enabled the blossoming and growth of outstanding research the field, once the colonial bondage was freed: Professors T R Seshadri, who was single-handedly responsible in generating excellent schools of medicinal products chemistry across the country, K Venkataraman who catalyzed many Indian-initiated chemical industries through his research and mentorship, and Salimuzzaman Siddiqui, who became the father of organic chemistry as well as modern scientific research in Pakistan in particular. Key words: Dyes, Foundations of science in Pakistan, Molecular structure, Natural products, Seshadri, Salimuzzaman Siddiqui, Venkataraman. 1. INTRODUCTION sense of national pride, and -

Studies on the Chemical Constituents of Azadirachta Indica A
Studies on the Chemical Constituents of Azadirachta indica A. Juss (Meliaceae), Part VII [1] Salimuzzaman Siddiqui*, Shaheen Faizi, and Bina Shaheen Siddiqui H. E. J. Research Institute of Chemistry, University of Karachi, Karachi-32, Pakistan Z. Naturforsch. 41b, 922 — 924 (1986); received September 30, 1985 Azadirachta indica, Meliaceae , 7-Deacetoxy-7 a-hydroxyazadiradione A new limonoid, nimbocinol, has been isolated from the fresh, undried, ripe fruits of Azadirachta indica (neem) along with known components, azadirone, epoxyazadiradione, azadiradione, gedunin, 17-hydroxyazadiradione and cholesterol. It is the first report of the isola tion of cholesterol from any part of the neem tree. Introduction unsaturated carbonyl), 1690 (cyclopentenone) and 3450 (OH). The molecular formula suggested the Azadirachta indica A. Juss (Meliaceae) is indige presence of 11 double bond equivalents, 3 of which nous to the Indo-Pakistan subcontinent and its various have been accounted for by a furan ring, 4 by two parts are reputed as therapeutic agents [2, 3]. Some a,/3-unsaturated ketone systems and the remaining 4 of the constituents of neem have recently been by the four rings of the nucleus. These suggestions shown to possess significant pesticidal activity [4]. were further supported by the mass spectrum of nim More recent studies undertaken on the fresh, un bocinol which showed peaks at mle 137 (ring-A with dried, uncrushed, ripe and unripe, fruits and the un a,/?-unsaturated ketone), and mle 81 (ion “a”) in dried leaves of the plant by Siddiqui et al. have led to addition to peaks at mle 408 (M+), 393 (M-15)+, the isolation and structure elucidation of nine new 390 (M-18)+, 375 (M-18-15)+, 328 (M-80)+, 309 triterpenoids viz, nimolicinol [5], nimocinol [ 6], (M-81-18)+, 299 (M-109)+ and 227 (ion “b”). -

Ventricular Tachycardia Drugs Versus Devices John Camm St
Cardiology Update 2015 Davos, Switzerland: 8-12th February 2015 Ventricular Arrhythmias Ventricular Tachycardia Drugs versus Devices John Camm St. George’s University of London, UK Imperial College, London, UK Declaration of Interests Chairman: NICE Guidelines on AF, 2006; ESC Guidelines on Atrial Fibrillation, 2010 and Update, 2012; ACC/AHA/ESC Guidelines on VAs and SCD; 2006; NICE Guidelines on ACS and NSTEMI, 2012; NICE Guidelines on heart failure, 2008; NICE Guidelines on Atrial Fibrillation, 2006; ESC VA and SCD Guidelines, 2015 Steering Committees: multiple trials including novel anticoagulants DSMBs: multiple trials including BEAUTIFUL, SHIFT, SIGNIFY, AVERROES, CASTLE- AF, STAR-AF II, INOVATE, and others Events Committees: one trial of novel oral anticoagulants and multiple trials of miscellaneous agents with CV adverse effects Editorial Role: Editor-in-Chief, EP-Europace and Clinical Cardiology; Editor, European Textbook of Cardiology, European Heart Journal, Electrophysiology of the Heart, and Evidence Based Cardiology Consultant/Advisor/Speaker: Astellas, Astra Zeneca, ChanRX, Gilead, Merck, Menarini, Otsuka, Sanofi, Servier, Xention, Bayer, Boehringer Ingelheim, Bristol- Myers Squibb, Daiichi Sankyo, Pfizer, Boston Scientific, Biotronik, Medtronic, St. Jude Medical, Actelion, GlaxoSmithKline, InfoBionic, Incarda, Johnson and Johnson, Mitsubishi, Novartis, Takeda Therapy for Ventricular Tachycardia Medical therapy Antiarrhythmic drugs Autonomic management Ventricular tachycardia Monomorphic Polymorphic Ventricular fibrillation Ventricular storms Ablation therapy Device therapy Surgical Defibrillation Catheter Antitachycardia pacing History of Antiarrhythmic Drugs 1914 - Quinidine 1950 - Lidocaine 1951 - Procainamide 1946 – Digitalis 1956 – Ajmaline 1962 - Verapamil 1962 – Disopyramide 1964 - Propranolol 1967 – Amiodarone 1965 – Bretylium 1972 – Mexiletine 1973 – Aprindine, Tocainide 1969 - Diltiazem 1975- Flecainide 1976 – Propafenone Encainide Ethmozine 2000 - Sotalol D-sotalol 1995 - Ibutilide (US) Recainam 2000 – Dofetilide US) IndecainideX Etc. -
Open Access Journal of Cardiology Ventricular Tachycardia During Ajmaline Challenge
Open Access Journal of Cardiology Ventricular Tachycardia During Ajmaline Challenge Estrada Parra I, Pavón Jimenez R, Leal del Ojo J, Garcia Medina D, Case Report Picon Heras R* and Pastor Torres L Volume 1 Issue 1 Received Date: May 22, 2017 Departamento de Cardiologia, Hospital Universitario Virgen de Valme, Spain Published Date: August 19, 2017 *Corresponding author: Rocio Picon, Departamento de Cardiologia, Hospital Universitario Virgen de Valme, Spain, E- mail: [email protected] Abstract We report the case of a 63 year old woman who comes to an ajmaline challenged. After 8 minutes of infusion her baseline ECG showed significant QRS complex prolongation and switched over to the typical coved-type ECG. Subsequently a sustained monomorphic ventricular tachycardia was developed, followed by a sustained polymorphyc VT onset, which finally degenerated in a hemodynamically non relevant sustained monomorphic VT. Finally, a 200J defibrillation was required to terminate the arrythmia. Sustained ventricular arrhytmia (SVA) is infrequent but not an exceptional event (0.1-18%) and ajmaline is considered a valuable drug. In addition, provocation testing must be performed in an appropiate environment with advanced life support facilities. The evidence shows that the occurrence of ajmaline-induced sustained ventricular arryhtmia in patients with BS might not identify a category at higher risk for further arrhythmic events during follow-up. Keywords: Brugada syndrome; Sodium channel blocker Challenge; Ajmaline Challenge; Ventricular arrhythmias; Proarrhythmia Abbrevations: ECG: Electrocardiography; BS: Brugada infusion she showed significant QRS complex Syndrome; SCB: Sodium Channel Blockers; VT: prolongation (174 ms) and ST elevation in the right Ventricular Tachycardia; SVA: Sustained ventricular precordial leads, which switched over to the typical arrhytmia coved-type ECG (Figure 2). -

Shanti Swarup Bhatnagar, Working Through/Against the Colonial System
Indian Journal of History of Science, 53.4 (2018) T51-T59 DOI: 10.16943/ijhs/2018/v53i4/49525 Shanti Swarup Bhatnagar, Working through/against the Colonial System Robert Anderson* (Received 18 April 2018; revised 17 May 2018) Abstract Shanti Swarup Bhatnagar was unusual in the scientific community of twentieth century India, perhaps unique. His behaviour tested the ‘default settings’ of the political and administrative system in which he lived and worked, as shown here in three examples from his life. Constrained by those settings like everyone else, he nevertheless found an entrepreneurial space in which he could experiment with innovations. He was a leader with an ego, but also seems to have been an enabler, still able to identify promise in others. Although he was deep in the rules of the system, he does not appear to have been a blocker of other peoples’ potential. Bhatnagar was, when we see him in these three situations, usually in transition from one state [in the chemical sense] to another. He was polyvalent, combining and acting with quite difference forces. He seems never to have been trapped in a binary set of oppositions, at least not for long. He was a sign, in the semiotic sense, which could be read in two or three different ways. All this made him an intermediary leader in the building of scientific institutions for the scientific community, channeling the energies and resources of the colonial system through the hands of the builders, some of whom he had picked himself. But what kind of leader was Bhatnagar in the last stage of his life? Key words: Atomic energy, Bhabha, Chemistry and chemists, Coerseduction, Colonial ‘system’, CSIR, Delhi, Entrepreneurial space, Hegemony, IISc, Intermediary leader, Lahore, London rules, National laboratories, Raman, Saha. -

Year: 1959; Month: January; Page: 1
VOL.: 2; NO.:1; YEAR: 1959; MONTH: JANUARY; PAGE: 1 STUDIES IN THE PROPERTIES OF HEAT INSULATING BUILDING MATERIALS Part II. – The Thermal Conductivity of Binary Mixtures with Particular Reference to Cellular Concrete MAZHAR MAHMOOD QURASHI AND A. K. M. AHSANULLAH Central Laboratories, Pakistan Council of Scientific and Industrial Research, Karachi Vol.: 2; No.:1; Year: 1959; Month: January; Page: 10 SOME VALUABLE CONSTITUENTS OF OIL CAKES FROM EAST PAKISTAN M. QUDRAT-I-KHUDA, H. RAHMAN, S. FAZL-I-RUBBI, B. D. MUKHERJEE AND N. A. KHAN East Regional Laboratories, Pakistan Council of Scientific and Industrial Research, Tejgaon, Dacca Vol.: 2; No.:1; Year: 1959; Month: January; Page: 13 DEVELOPMENT OF RAPID METHODS FOR THE ESTIMATION OF THE OIL CONTENT OF SINGLE COTTONSEEDS Part I.—An Oil-Expression Technique S. NURUL AHMAD AND MAZHAR MAHMOOD QURASHI Central Laboratories, Pakistan Council of Scientific and Industrial Research, Karachi Vol.: 2; No.:1; Year: 1959; Month: January; Page: 19 SPECTROPHOTOMETRIC STUDY OF MERCURIC CHLORIDE- DIPHENYLCARBAZONE COMPLEX BETWEEN 4000° AND 7000° A NASIM MUFTI AND NAHEED FATIMA Department of Physics, University of Sind, Hyderabad Vol.: 2; No.:1; Year: 1959; Month: January; Page: 21 INFRARED ABSORPTION STUDY OF THE RELATION BETWEEN VISCOSITY AND INTERMOLECULAR HYDROGEN BOND FORMATION FOR SOLUTIONS OF PHENOLIC COMPOUNDS IN OIL Part I.—Solutions of Bhilawanol in Mineral Oil MAZHAR MAHMOOD QURASHI AND SARFARAZ H. ZAIDI Central Laboratories, Pakistan Council of Scientific and Industrial Research, Karachi. Vol.: -

The Anti-Addiction Drug Ibogaine and the Heart: a Delicate Relation
Molecules 2015, 20, 2208-2228; doi:10.3390/molecules20022208 OPEN ACCESS molecules ISSN 1420-3049 www.mdpi.com/journal/molecules Review The Anti-Addiction Drug Ibogaine and the Heart: A Delicate Relation Xaver Koenig * and Karlheinz Hilber * Department of Neurophysiology and Neuropharmacology, Center for Physiology and Pharmacology, Medical University of Vienna, Schwarzspanierstrasse 17, Vienna 1090, Austria * Authors to whom correspondence should be addressed; E-Mails: [email protected] (X.K.); [email protected] (K.H.); Tel.: +43-1-40160-31232 (X.K.); +43-1-40160-31230 (K.H.); Fax: +43-1-40160-931300 (X.K. & K.H.). Academic Editor: Patricia Valentao Received: 24 October 2014 / Accepted: 26 November 2014 / Published: 29 January 2015 Abstract: The plant indole alkaloid ibogaine has shown promising anti-addictive properties in animal studies. Ibogaine is also anti-addictive in humans as the drug alleviates drug craving and impedes relapse of drug use. Although not licensed as therapeutic drug and despite safety concerns, ibogaine is currently used as an anti-addiction medication in alternative medicine in dozens of clinics worldwide. In recent years, alarming reports of life-threatening complications and sudden death cases, temporally associated with the administration of ibogaine, have been accumulating. These adverse reactions were hypothesised to be associated with ibogaine’s propensity to induce cardiac arrhythmias. The aim of this review is to recapitulate the current knowledge about ibogaine’s effects on the heart and the cardiovascular system, and to assess the cardiac risks associated with the use of this drug in anti- addiction therapy. The actions of 18-methoxycoronaridine (18-MC), a less toxic ibogaine congener with anti-addictive properties, are also considered. -

Vol.: 1; No.:1; Year: 1958; Month: January; Page: 3 Studies In
VOL.: 1; NO.:1; YEAR: 1958; MONTH: JANUARY; PAGE: 3 STUDIES IN THE ALKALOIDS OF RAUWOLFIA SERPENTINA, BENTH. AND THE MODE OF THEIR OCCURRENCE Isolation of a new Hypotensive Factor and other Alkaloidal Complexes from the Roots SALIMUZZAMAN SIDDIQUI (In experimental collaboration with M. Alauddin) Central Laboratories, Pakistan Council of Scientific and Industrial Research, Karachi Vol.: 1; No.: 1; Year: 1958; Month: January; Page: 6 PHARMACOLOGICAL INVESTIGATION OF AN ALKALOIDAL FACTOR OF RAUWOLFIA SERPENTINA ROLF DEININGER Central Laboratories, Pakistan Council of Scientific and Industrial Research, Karachi Vol.: 1; No.: 1; Year: 1958; Month: January; Page: 7 STUDIES IN THE INFLUENCE OF LONG-CHAIN PHENOLIC ADDITIVES ON THE VISCOSITY OF MINERAL OILS Part I.—Mixture of Mineral Oil with Bhilawanol and its Derivatives MAZHAR MAHMOOD QURASHI Central Laboratories, Pakistan Council of Scientific and Industrial Research, Karachi Vol.: 1; No.: 1; Year: 1958; Month: January; Page: 12 INFRARED STUDIES ON SOME FEATURES OF METHYLENE-INTERRUPTED DOUBLE BOND IN AUTOXIDATION OF FATTY ACID ESTERS NURUL ABSAR KHAN East Regional Laboratories, Pakistan Council of Scientific and Industrial Research, Tejgaon, Dacca, East Pakistan Vol.: 1; No.: 1; Year: 1958; Month: January; Page: 17 OXIDATION OF SODIUM SULPHIDE WITH NITRIC OXIDE QAZI MOHAMMAD SIDDIQUE AND BADRUDDIN University Institute of Chemistry, Lahore, West Pakistan Vol.: 1; No.: 1; Year: 1958; Month: January; Page: 26 RADIO FREQUENCY TRANSMISSION SYSTEM A 30 MEV ELECTRON CYCLOTRON M. INNAS ALI Physics -
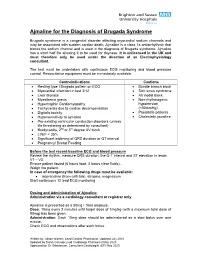
Use of Ajmaline for the Diagnosis of Brugada Syndrome
Ajmaline for the Diagnosis of Brugada Syndrome Brugada syndrome is a congenital disorder affecting myocardial sodium channels and may be associated with sudden cardiac death. Ajmaline is a class 1a antiarrhythmic that blocks the sodium channel and is used in the diagnosis of Brugada syndrome. Ajmaline has a short half life allowing it to be used for daycase. It is unlicensed in the UK and must therefore only be used under the direction of an Electrophysiology consultant. The test must be undertaken with continuous ECG monitoring and blood pressure control. Resuscitative equipment must be immediately available. Contraindications Cautions Resting type I Brugada pattern on ECG Bundle branch block Myocardial infarction in last 3/12 Sick sinus syndrome Liver disease AV nodal block Myasthenia gravis Non-rhythmogenic Hypertrophic Cardiomyopathy hypotension Tachycardia due to cardiac decompensation (<90mmHg) Digitalis toxicity Paediatric patients Hypersensitivity to ajmaline Cholestatic jaundice Pre-existing ventricular conduction disorders (unless life threatening as determined by consultant) Bradycardia, 2nd or 3rd degree AV block LVEF < 35% Significant widening of QRS duration or QT interval Pregnancy/ Breast Feeding Before the test record baseline ECG and blood pressure Review the rhythm, measure QRS duration, the Q-T interval and ST elevation in leads V1 – V3. Ensure patient fasted (6 hours food, 2 hours clear fluids). Weigh the patient. In case of emergency the following drugs must be available: isoprenaline (from cath lab), atropine, magnesium Start continuous 12 lead ECG monitoring Dosing and Administration of Ajmaline: Administration via a cardiology consultant or registrar only Ajmaline is presented as a 50mg / 10ml ampoule. Dose: 10mg every 2 minutes until target dose of 1mg/kg (with a maximum total dose of 80mg) has been given.