Ajmaline-Induced Block of Sodium Current in Rat Ventricular Myocytes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2D6 Substrates 2D6 Inhibitors 2D6 Inducers
Physician Guidelines: Drugs Metabolized by Cytochrome P450’s 1 2D6 Substrates Acetaminophen Captopril Dextroamphetamine Fluphenazine Methoxyphenamine Paroxetine Tacrine Ajmaline Carteolol Dextromethorphan Fluvoxamine Metoclopramide Perhexiline Tamoxifen Alprenolol Carvedilol Diazinon Galantamine Metoprolol Perphenazine Tamsulosin Amiflamine Cevimeline Dihydrocodeine Guanoxan Mexiletine Phenacetin Thioridazine Amitriptyline Chloropromazine Diltiazem Haloperidol Mianserin Phenformin Timolol Amphetamine Chlorpheniramine Diprafenone Hydrocodone Minaprine Procainamide Tolterodine Amprenavir Chlorpyrifos Dolasetron Ibogaine Mirtazapine Promethazine Tradodone Aprindine Cinnarizine Donepezil Iloperidone Nefazodone Propafenone Tramadol Aripiprazole Citalopram Doxepin Imipramine Nifedipine Propranolol Trimipramine Atomoxetine Clomipramine Encainide Indoramin Nisoldipine Quanoxan Tropisetron Benztropine Clozapine Ethylmorphine Lidocaine Norcodeine Quetiapine Venlafaxine Bisoprolol Codeine Ezlopitant Loratidine Nortriptyline Ranitidine Verapamil Brofaramine Debrisoquine Flecainide Maprotline olanzapine Remoxipride Zotepine Bufuralol Delavirdine Flunarizine Mequitazine Ondansetron Risperidone Zuclopenthixol Bunitrolol Desipramine Fluoxetine Methadone Oxycodone Sertraline Butylamphetamine Dexfenfluramine Fluperlapine Methamphetamine Parathion Sparteine 2D6 Inhibitors Ajmaline Chlorpromazine Diphenhydramine Indinavir Mibefradil Pimozide Terfenadine Amiodarone Cimetidine Doxorubicin Lasoprazole Moclobemide Quinidine Thioridazine Amitriptyline Cisapride -

Systematic Review of the Effect of Intravenous Lipid Emulsion Therapy for Non-Local Anesthetics Toxicity
Clinical Toxicology ISSN: 1556-3650 (Print) 1556-9519 (Online) Journal homepage: http://www.tandfonline.com/loi/ictx20 Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity Michael Levine, Robert S. Hoffman, Valéry Lavergne, Christine M. Stork, Andis Graudins, Ryan Chuang, Samuel J. Stellpflug, Martin Morris, Andrea Miller-Nesbitt, Sophie Gosselin & for the Lipid Emulsion Workgroup* To cite this article: Michael Levine, Robert S. Hoffman, Valéry Lavergne, Christine M. Stork, Andis Graudins, Ryan Chuang, Samuel J. Stellpflug, Martin Morris, Andrea Miller-Nesbitt, Sophie Gosselin & for the Lipid Emulsion Workgroup* (2016) Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity, Clinical Toxicology, 54:3, 194-221, DOI: 10.3109/15563650.2015.1126286 To link to this article: http://dx.doi.org/10.3109/15563650.2015.1126286 Published online: 06 Feb 2016. Submit your article to this journal Article views: 692 View related articles View Crossmark data Citing articles: 2 View citing articles Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ictx20 Download by: [UPSTATE Medical University Health Sciences Library] Date: 03 August 2016, At: 08:19 CLINICAL TOXICOLOGY, 2016 VOL. 54, NO. 3, 194–221 http://dx.doi.org/10.3109/15563650.2015.1126286 REVIEW Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity Michael Levinea, Robert S. Hoffmanb, Vale´ry Lavergnec, Christine M. Storkd, Andis Graudinse, Ryan Chuangf, Samuel J. Stellpflugg, Martin Morrish, Andrea Miller-Nesbitth, Sophie Gosselini and for the Lipid Emulsion Workgroup* aDepartment of Emergency Medicine, Section of Medical Toxicology, University of Southern California, Los Angeles, CA, USA; bDivision of Medical Toxicology, Ronald O. -

Ventricular Tachycardia Drugs Versus Devices John Camm St
Cardiology Update 2015 Davos, Switzerland: 8-12th February 2015 Ventricular Arrhythmias Ventricular Tachycardia Drugs versus Devices John Camm St. George’s University of London, UK Imperial College, London, UK Declaration of Interests Chairman: NICE Guidelines on AF, 2006; ESC Guidelines on Atrial Fibrillation, 2010 and Update, 2012; ACC/AHA/ESC Guidelines on VAs and SCD; 2006; NICE Guidelines on ACS and NSTEMI, 2012; NICE Guidelines on heart failure, 2008; NICE Guidelines on Atrial Fibrillation, 2006; ESC VA and SCD Guidelines, 2015 Steering Committees: multiple trials including novel anticoagulants DSMBs: multiple trials including BEAUTIFUL, SHIFT, SIGNIFY, AVERROES, CASTLE- AF, STAR-AF II, INOVATE, and others Events Committees: one trial of novel oral anticoagulants and multiple trials of miscellaneous agents with CV adverse effects Editorial Role: Editor-in-Chief, EP-Europace and Clinical Cardiology; Editor, European Textbook of Cardiology, European Heart Journal, Electrophysiology of the Heart, and Evidence Based Cardiology Consultant/Advisor/Speaker: Astellas, Astra Zeneca, ChanRX, Gilead, Merck, Menarini, Otsuka, Sanofi, Servier, Xention, Bayer, Boehringer Ingelheim, Bristol- Myers Squibb, Daiichi Sankyo, Pfizer, Boston Scientific, Biotronik, Medtronic, St. Jude Medical, Actelion, GlaxoSmithKline, InfoBionic, Incarda, Johnson and Johnson, Mitsubishi, Novartis, Takeda Therapy for Ventricular Tachycardia Medical therapy Antiarrhythmic drugs Autonomic management Ventricular tachycardia Monomorphic Polymorphic Ventricular fibrillation Ventricular storms Ablation therapy Device therapy Surgical Defibrillation Catheter Antitachycardia pacing History of Antiarrhythmic Drugs 1914 - Quinidine 1950 - Lidocaine 1951 - Procainamide 1946 – Digitalis 1956 – Ajmaline 1962 - Verapamil 1962 – Disopyramide 1964 - Propranolol 1967 – Amiodarone 1965 – Bretylium 1972 – Mexiletine 1973 – Aprindine, Tocainide 1969 - Diltiazem 1975- Flecainide 1976 – Propafenone Encainide Ethmozine 2000 - Sotalol D-sotalol 1995 - Ibutilide (US) Recainam 2000 – Dofetilide US) IndecainideX Etc. -
Open Access Journal of Cardiology Ventricular Tachycardia During Ajmaline Challenge
Open Access Journal of Cardiology Ventricular Tachycardia During Ajmaline Challenge Estrada Parra I, Pavón Jimenez R, Leal del Ojo J, Garcia Medina D, Case Report Picon Heras R* and Pastor Torres L Volume 1 Issue 1 Received Date: May 22, 2017 Departamento de Cardiologia, Hospital Universitario Virgen de Valme, Spain Published Date: August 19, 2017 *Corresponding author: Rocio Picon, Departamento de Cardiologia, Hospital Universitario Virgen de Valme, Spain, E- mail: [email protected] Abstract We report the case of a 63 year old woman who comes to an ajmaline challenged. After 8 minutes of infusion her baseline ECG showed significant QRS complex prolongation and switched over to the typical coved-type ECG. Subsequently a sustained monomorphic ventricular tachycardia was developed, followed by a sustained polymorphyc VT onset, which finally degenerated in a hemodynamically non relevant sustained monomorphic VT. Finally, a 200J defibrillation was required to terminate the arrythmia. Sustained ventricular arrhytmia (SVA) is infrequent but not an exceptional event (0.1-18%) and ajmaline is considered a valuable drug. In addition, provocation testing must be performed in an appropiate environment with advanced life support facilities. The evidence shows that the occurrence of ajmaline-induced sustained ventricular arryhtmia in patients with BS might not identify a category at higher risk for further arrhythmic events during follow-up. Keywords: Brugada syndrome; Sodium channel blocker Challenge; Ajmaline Challenge; Ventricular arrhythmias; Proarrhythmia Abbrevations: ECG: Electrocardiography; BS: Brugada infusion she showed significant QRS complex Syndrome; SCB: Sodium Channel Blockers; VT: prolongation (174 ms) and ST elevation in the right Ventricular Tachycardia; SVA: Sustained ventricular precordial leads, which switched over to the typical arrhytmia coved-type ECG (Figure 2). -

The Anti-Addiction Drug Ibogaine and the Heart: a Delicate Relation
Molecules 2015, 20, 2208-2228; doi:10.3390/molecules20022208 OPEN ACCESS molecules ISSN 1420-3049 www.mdpi.com/journal/molecules Review The Anti-Addiction Drug Ibogaine and the Heart: A Delicate Relation Xaver Koenig * and Karlheinz Hilber * Department of Neurophysiology and Neuropharmacology, Center for Physiology and Pharmacology, Medical University of Vienna, Schwarzspanierstrasse 17, Vienna 1090, Austria * Authors to whom correspondence should be addressed; E-Mails: [email protected] (X.K.); [email protected] (K.H.); Tel.: +43-1-40160-31232 (X.K.); +43-1-40160-31230 (K.H.); Fax: +43-1-40160-931300 (X.K. & K.H.). Academic Editor: Patricia Valentao Received: 24 October 2014 / Accepted: 26 November 2014 / Published: 29 January 2015 Abstract: The plant indole alkaloid ibogaine has shown promising anti-addictive properties in animal studies. Ibogaine is also anti-addictive in humans as the drug alleviates drug craving and impedes relapse of drug use. Although not licensed as therapeutic drug and despite safety concerns, ibogaine is currently used as an anti-addiction medication in alternative medicine in dozens of clinics worldwide. In recent years, alarming reports of life-threatening complications and sudden death cases, temporally associated with the administration of ibogaine, have been accumulating. These adverse reactions were hypothesised to be associated with ibogaine’s propensity to induce cardiac arrhythmias. The aim of this review is to recapitulate the current knowledge about ibogaine’s effects on the heart and the cardiovascular system, and to assess the cardiac risks associated with the use of this drug in anti- addiction therapy. The actions of 18-methoxycoronaridine (18-MC), a less toxic ibogaine congener with anti-addictive properties, are also considered. -
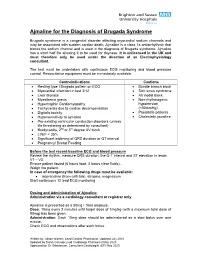
Use of Ajmaline for the Diagnosis of Brugada Syndrome
Ajmaline for the Diagnosis of Brugada Syndrome Brugada syndrome is a congenital disorder affecting myocardial sodium channels and may be associated with sudden cardiac death. Ajmaline is a class 1a antiarrhythmic that blocks the sodium channel and is used in the diagnosis of Brugada syndrome. Ajmaline has a short half life allowing it to be used for daycase. It is unlicensed in the UK and must therefore only be used under the direction of an Electrophysiology consultant. The test must be undertaken with continuous ECG monitoring and blood pressure control. Resuscitative equipment must be immediately available. Contraindications Cautions Resting type I Brugada pattern on ECG Bundle branch block Myocardial infarction in last 3/12 Sick sinus syndrome Liver disease AV nodal block Myasthenia gravis Non-rhythmogenic Hypertrophic Cardiomyopathy hypotension Tachycardia due to cardiac decompensation (<90mmHg) Digitalis toxicity Paediatric patients Hypersensitivity to ajmaline Cholestatic jaundice Pre-existing ventricular conduction disorders (unless life threatening as determined by consultant) Bradycardia, 2nd or 3rd degree AV block LVEF < 35% Significant widening of QRS duration or QT interval Pregnancy/ Breast Feeding Before the test record baseline ECG and blood pressure Review the rhythm, measure QRS duration, the Q-T interval and ST elevation in leads V1 – V3. Ensure patient fasted (6 hours food, 2 hours clear fluids). Weigh the patient. In case of emergency the following drugs must be available: isoprenaline (from cath lab), atropine, magnesium Start continuous 12 lead ECG monitoring Dosing and Administration of Ajmaline: Administration via a cardiology consultant or registrar only Ajmaline is presented as a 50mg / 10ml ampoule. Dose: 10mg every 2 minutes until target dose of 1mg/kg (with a maximum total dose of 80mg) has been given. -

Stembook 2018.Pdf
The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 WHO/EMP/RHT/TSN/2018.1 © World Health Organization 2018 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances. Geneva: World Health Organization; 2018 (WHO/EMP/RHT/TSN/2018.1). Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. -

Searchable Word Index for the 11Th Edition
Index 2319 Index A Acnisal 1921 Acomplia 1891 A2 234 aconite 34 AA-3 1014 aconitine 34 AAtack 2096 acrivastine 36 AAtrex 183 acrodynia 1297, 2086 abacavir 1 acrolein 37, 567 abamectin 2, 1135 acrylamide 38 Abba 2 acrylonitrile 40 AB-CHMINACA 2008 actein 619 ABDF 284 Actidex 631 Abelcet 127 Actifed 2193 Abilify 159 actinomycin D 41 abiraterone acetate 3 Actiq 883 Abitat 159 Actimax 1471 abobotulinumtoxinA 268 Actol 1527 abortifacients 344, 1436, 1449, 1648 Actonel 1892 AB-PINACA 2008 Actos 1733 Abraxane 1617 Actril 1108 abrin 4 Acular 1148 absinthe 2097 Acupan 1503 Abstral 883 Acuphase 2303 acamprosate 5 Acuvel 180 Acapodene 2143 acyclovir 42, 2214 acarbose 6 Adalat 1525 acaricides 111, 430, 2061 adalimumab 44 Acarin 663 Adalin 370 Accolate 2277 Adapin 745 Accupril 1853 Adartrel 1904 Accuprin 1853 Adasept 2175 Accuretic 1853 ADB-FUBINACA 2008 Accutane 1127 ADB-PINACA 2008 Accutrim 1707 Adcirca 2017 Acebron 9 Adco-Linctopent 280, 1580 acebutolol 7 Adderall 124 acecainide 1787 Addyi 898 aceclofenac 8 Adecut 612 Acecor 7 adefovir dipivoxil 45 ACE inhibitors 213, 350, 612, 952, 1205, 1223, 1460, 1669, ademine 2162 1853, 1865, 2035, 2151, 2291 Adempas 1892 acenocoumarol 9 Adenocard 46 Aceon 1669 adenosine 46, 666 acephate 11 ADHD drugs (see attention deficit disorder drugs) acepromazine 12 Adiazine 1989 Acetadote 24 Adion 137 acetaldehyde 13, 338, 819, 825, 1309, 1543, 1628 Adipex 1700 acetamide 698 Adizem 685 acetaminophen 15, 142, 1676, 1679 adrafinil 47, 1459 acetamiprid 18 adrenaline 789 acetanilide 142 Adriacin 747 acetazolamide 19 Adriamycin -
Egdb1de1.Pdf
1 2 A todos los que me han dado la fuerza y la ilusión para llegar aquí A mis padres, hermanas y Ricard, por su cariño, sus cuidados y su ejemplo, sin vosotros no hubiese sido posible. A Iñaki, porque cuando te fuiste, te llevaste parte de mi vida, pero lo vivido me acompañará siempre, y tu recuerdo me ayuda a ser mejor. 3 4 EVALUATION OF CARDIOTOXICITY OF RUPATADINE, AN ANTIHISTAMINE, AS RECOMMENDED BY THE ICH E14 AIMS: To evaluate the effects of therapeutic and supratherapeutic doses of rupatadine on cardiac repolarization in line with a 'thorough QT/QTc study' protocol performed according to International Conference on Harmonization guidelines. METHODS: This was a randomized (gender-balanced), parallel-group study involving 160 healthy volunteers. Rupatadine, 10 and 100 mg od, and placebo were administered single- blind for 5 days, whilst moxifloxacin 400 mg/day was given on days 1 and 5 in open- label fashion. ECGs were recorded over a 23-h period by continuous Holter monitoring at baseline and on treatment days 1 and 5. Three 10-s ECG samples were downloaded at regular intervals and were analysed independently. The primary analysis of QTc was based on individually corrected QT (QTcI). Treatment effects on QTcI were assessed using the largest time-matched mean difference between the drug and placebo (baseline-subtracted) for the QTcI interval. A negative 'thorough QT/QTc study' is one where the main variable is around < or =5 ms, with a one-sided 95% confidence interval that excludes an effect >10 ms. RESULTS: The validity of the trial was confirmed by the fact that the moxifloxacin-positive control group produced the expected change in QTcI duration (around 5 ms). -

Management of Tachyarrhythmia During Pregnancy
Turk Kardiyol Dern Ars 2017;45(2):189-196 doi: 10.5543/tkda.2016.78606 189 INVITED REVIEW Management of tachyarrhythmia during pregnancy Gebelik sırasında taşiaritmi tedavisi Emily Ann Enderlin, Khaldia Taufiq Khaled, M.D.,# Luke Oke, M.D.,* Mohammed Madmani, M.D.,† Hakan Paydak, M.D.* College of Medicine, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA #Department of Internal Medicine, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA *Department of Clinical Cardiac Electrophysiology, University of Arkansas for Medical Sciences, Lit †Department of Cardiovascular Medicine, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA Summary– Maternal tachyarrhythmia is a common compli- Özet– Annede taşiaritmi, hamile kadınlarda önceden var cation during pregnancy due to hormonal changes that en- olan aritmileri arttıran veya doğuştan kalp defektleri varlı- hance pre-existing arrhythmias or induce new arrhythmias ğında yeni aritmileri başlatan hormonal değişikliklere bağlı in the presence of congenital heart defects in pregnant fe- olarak sık görülen bir komplikasyondur. Gebelik sırasında males. Presence of tachyarrhythmia during pregnancy pos- taşiaritminin varlığı anne ve fetüs için risk oluşturmakta ve es risk to the mother and fetus, calling for proper treatment ilaçlarla uygun tedaviyi gerektirmektedir. Teratojenik yan et- with medications. Use of antiarrhythmic drugs in cases of kilerini de göz önüne alarak maternal taşiaritmide antiarit- maternal tachyarrhythmia must give due consideration of mik ilaçların kullanılması düşünülmelidir. Gebelik sırasında potential teratogenic side effects. Utilization of antiarrhyth- antiaritmik ilaçların kullanılması iyice incelenmiş olup bazı- mic drugs during pregnancy has been well studied; some ları minimal fötal hasara yol açacak bazıları hiç zararlı olma- result in minimal fetal harm or none at all. -

FDA-Approved Drug Library Mini (96-Well)
• Inhibitors • Agonists • Screening Libraries www.MedChemExpress.com FDA-Approved Drug Library Mini (96-well) Product Details: Catalog Number: HY-L022M Formulation: A collection of 1559 marketed drugs supplied as pre-dissolved DMSO solutions Container: 96 Well Microplate With Peelable Foil Seal Storage: -80°C Shipping: Blue ice Packaging: Inert gas Plate layout: HY-L022M-1 1 2 3 4 5 6 7 8 9 10 11 12 Plerixafor Zoledronic a Empty Sisomicin Streptomycin (octahydrochl acid Paromomycin Netilmicin Neomycin Levoleucovori Peramivir Capreomycin Empty (sulfate) (sulfate) oride) (monohydrate (sulfate) (sulfate) (sulfate) n (Calcium) (trihydrate) (sulfate) 4- L-Glutamic b Empty Amikacin Stibogluconat Gluconate Histamine Mangafodipir Cromolyn (Aminomethyl acid Citicoline Tranexamic Empty (sulfate) e (sodium) (Calcium) (phosphate) (trisodium) (sodium) )benzoic acid monosodium acid Ozagrel Chloroquine Heparin Sugammadex Citicoline Ribostamycin c Empty sodium (diphosphate) Gadobutrol L-Ornithine (sodium salt) (sodium) Zanamivir sodium salt (sulfate) Glucosamine Empty d Empty L-Arginine Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty e Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty f Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty g Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty h Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Empty Plate layout: HY-L022M-2 1 2 3 4 5 6 7 8 9 10 11 12 Etomidate Epirubicin Tetramisole a Empty Ibrutinib (hydrochlorid -

Fibrillation Promoting Sinus Rhythm in Patients with Atrial the Effectiveness of Antiarrhythmic Agents at Meta-Analysis of Rando
Downloaded from heart.bmj.com on August 12, 2010 - Published by group.bmj.com Meta-analysis of randomised controlled trials of the effectiveness of antiarrhythmic agents at promoting sinus rhythm in patients with atrial fibrillation G Nichol, F McAlister, B Pham, et al. Heart 2002 87: 535-543 doi: 10.1136/heart.87.6.535 Updated information and services can be found at: http://heart.bmj.com/content/87/6/535.full.html These include: Supplemental http://heart.bmj.com/content/suppl/2002/07/10/87.6.535.DC1.html Material References This article cites 118 articles, 55 of which can be accessed free at: http://heart.bmj.com/content/87/6/535.full.html#ref-list-1 Article cited in: http://heart.bmj.com/content/87/6/535.full.html#related-urls Email alerting Receive free email alerts when new articles cite this article. Sign up in the box at service the top right corner of the online article. Topic collections Articles on similar topics can be found in the following collections Drugs: cardiovascular system (22936 articles) Epidemiology (4934 articles) Notes To order reprints of this article go to: http://heart.bmj.com/cgi/reprintform To subscribe to Heart go to: http://heart.bmj.com/subscriptions Downloaded from heart.bmj.com on August 12, 2010 - Published by group.bmj.com 535 CARDIOVASCULAR MEDICINE Meta-analysis of randomised controlled trials of the effectiveness of antiarrhythmic agents at promoting sinus rhythm in patients with atrial fibrillation G Nichol, F McAlister, B Pham, A Laupacis, B Shea, M Green, A Tang, G Wells ............................................................................................................................