Introduction Remove the Udder Removing the Pizzle (Penis)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reference Sheet 1
MALE SEXUAL SYSTEM 8 7 8 OJ 7 .£l"00\.....• ;:; ::>0\~ <Il '"~IQ)I"->. ~cru::>s ~ 6 5 bladder penis prostate gland 4 scrotum seminal vesicle testicle urethra vas deferens FEMALE SEXUAL SYSTEM 2 1 8 " \ 5 ... - ... j 4 labia \ ""\ bladderFallopian"k. "'"f"";".'''¥'&.tube\'WIT / I cervixt r r' \ \ clitorisurethrauterus 7 \ ~~ ;~f4f~ ~:iJ 3 ovaryvagina / ~ 2 / \ \\"- 9 6 adapted from F.L.A.S.H. Reproductive System Reference Sheet 3: GLOSSARY Anus – The opening in the buttocks from which bowel movements come when a person goes to the bathroom. It is part of the digestive system; it gets rid of body wastes. Buttocks – The medical word for a person’s “bottom” or “rear end.” Cervix – The opening of the uterus into the vagina. Circumcision – An operation to remove the foreskin from the penis. Cowper’s Glands – Glands on either side of the urethra that make a discharge which lines the urethra when a man gets an erection, making it less acid-like to protect the sperm. Clitoris – The part of the female genitals that’s full of nerves and becomes erect. It has a glans and a shaft like the penis, but only its glans is on the out side of the body, and it’s much smaller. Discharge – Liquid. Urine and semen are kinds of discharge, but the word is usually used to describe either the normal wetness of the vagina or the abnormal wetness that may come from an infection in the penis or vagina. Duct – Tube, the fallopian tubes may be called oviducts, because they are the path for an ovum. -

The Anatomy of the Rectum and Anal Canal
BASIC SCIENCE identify the rectosigmoid junction with confidence at operation. The anatomy of the rectum The rectosigmoid junction usually lies approximately 6 cm below the level of the sacral promontory. Approached from the distal and anal canal end, however, as when performing a rigid or flexible sigmoid- oscopy, the rectosigmoid junction is seen to be 14e18 cm from Vishy Mahadevan the anal verge, and 18 cm is usually taken as the measurement for audit purposes. The rectum in the adult measures 10e14 cm in length. Abstract Diseases of the rectum and anal canal, both benign and malignant, Relationship of the peritoneum to the rectum account for a very large part of colorectal surgical practice in the UK. Unlike the transverse colon and sigmoid colon, the rectum lacks This article emphasizes the surgically-relevant aspects of the anatomy a mesentery (Figure 1). The posterior aspect of the rectum is thus of the rectum and anal canal. entirely free of a peritoneal covering. In this respect the rectum resembles the ascending and descending segments of the colon, Keywords Anal cushions; inferior hypogastric plexus; internal and and all of these segments may be therefore be spoken of as external anal sphincters; lymphatic drainage of rectum and anal canal; retroperitoneal. The precise relationship of the peritoneum to the mesorectum; perineum; rectal blood supply rectum is as follows: the upper third of the rectum is covered by peritoneum on its anterior and lateral surfaces; the middle third of the rectum is covered by peritoneum only on its anterior 1 The rectum is the direct continuation of the sigmoid colon and surface while the lower third of the rectum is below the level of commences in front of the body of the third sacral vertebra. -

How to Increase Your Enjoyment of Sex
BETTER SEX BETTER SEX BETTER SEX BETTER SEX BETTER SEX OF SEX ENJO YOUR INCREASE HOW TO for women and women for their partners YMENT “Sexual health is a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled.” Definition of sexual health, World Health Organisation SAFER SEX Using condoms for penetrative sex is the best way to protect yourself and your partners from Sexually Transmitted Infections, including HIV. Condoms also offer good protection from unwanted pregnancy. In the text of this booklet, we have chosen not to refer constantly to the use of condoms. Instead, we encourage you to make your own decisions about protecting yourself and others in each instance of sexual activity you undertake. 1 HOW TO INCREASE YOUR ENJOYMENT OF SEX This leaflet provides information on how to help yourself improve your enjoyment of sex. It has three main parts: Suggestions on how to improve sex generally, without doing formal exercises. These apply to both casual and regular partners. Exercises you can do on your own — for women who have difficulty getting turned on or experiencing orgasm, and who may or may not have a regular partner. Exercises you can do with a partner — for women who have difficulty getting turned on, or who have difficulty having an orgasm or enjoying penetrative sex. -

View of Urothelial and Metastatic Carcinoma Including Clinical Presentation, Diagnostic Testing, Treatment and Chiropractic Considerations Is Discussed
Daniels et al. Chiropractic & Manual Therapies (2016) 24:14 DOI 10.1186/s12998-016-0097-8 CASE REPORT Open Access Bladder metastasis presenting as neck, arm and thorax pain: a case report Clinton J. Daniels1,2,3*, Pamela J. Wakefield1,2 and Glenn A. Bub1,2 Abstract Background: A case of metastatic carcinoma secondary to urothelial carcinoma presenting as musculoskeletal pain is reported. A brief review of urothelial and metastatic carcinoma including clinical presentation, diagnostic testing, treatment and chiropractic considerations is discussed. Case presentation: This patient presented in November 2014 with progressive neck, thorax and upper extremity pain. Computed tomography revealed a destructive soft tissue mass in the cervical spine and additional lytic lesion of the 1st rib. Prompt referral was made for surgical consultation and medical management. Conclusion: Distant metastasis is rare, but can present as a musculoskeletal complaint. History of carcinoma should alert the treating chiropractic physician to potential for serious disease processes. Keywords: Chiropractic, Neck pain, Transitional cell carcinoma, Bladder cancer, Metastasis, Case report Background serious complication of UC is distant metastasis—with Urothelial carcinoma (UC), also known as transitional higher stage cancer and lymph involvement worsening cell carcinoma (TCC), accounts for more than 90 % of prognosis and cancer survival rate [10]. The 5-year all bladder cancers and commonly metastasizes to the cancer-specific survival rate of UC is estimated to be pelvic lymph nodes, lungs, liver, bones and adrenals or 78 % [10, 11]. brain [1, 2]. The spread of bladder cancer is mainly done Neck pain accounts for 24 % of all disorders seen by via the lymphatic system with the most frequent location chiropractors [12]. -

The Ear, Nose, and Throat Exam Jeffrey Texiera, MD and Joshua Jabaut, MD CPT, MC, USA LT, MC, USN
The Ear, Nose, and Throat Exam Jeffrey Texiera, MD and Joshua Jabaut, MD CPT, MC, USA LT, MC, USN Midatlantic Regional Occupational and Environmental Medicine Conference Sept. 23, 2017 Disclosures ●We have no funding or financial interest in any product featured in this presentation. The items included are for demonstration purposes only. ●We have no conflicts of interest to disclose. Overview ● Overview of clinically oriented anatomy - presented in the format of the exam ● The approach ● The examination ● Variants of normal anatomy ● ENT emergencies ● Summary/highlights ● Questions Anatomy ● The head and neck exam consists of some of the most comprehensive and complicated anatomy in the human body. ● The ear, nose, and throat comprise a portion of that exam and a focused clinical encounter for an acute ENT complaint may require only this portion of the exam. Ears www.Medscape.com www.taqplayer.info Ear – Vestibular organ www.humanantomylibrary.com Nose/Sinus Anatomy Inferior Middle Turbinate Turbinate Septum Dorsum Sidewalls Ala Floor Tip www.ENT4Students.blogspot.com Columella Vestibule www.beautyepic.com Oral cavity and oropharynx (throat) www.apsubiology.org Neck www.rdhmag.com The Ear, Nose, and Throat exam Perform in a standardized systematic way that works for you Do it the same way every time, this mitigates risk of missing a portion of the exam Practice the exam to increase comfort with performance and familiarize self with variants of normal Describe what you are doing to the patient, describe what you see in your documentation Use your PPE as appropriate A question to keep in mind… ●T/F: The otoscope is the optimal tool for examining the tympanic membrane. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Silent Reflux (Also Called LPR Or EOR)
Silent reflux (also called LPR or EOR) This leaflet explains what your condition is, why it happens, what the symptoms are and how it can be managed. If there is anything you don’t understand or if you have any further questions please talk to your doctor or nurse. What is silent reflux? Everyone has juices in the stomach which are acidic and digest and break down food. At the top of the stomach there is a muscular valve which closes to prevent food and stomach juices escaping upwards into the gullet. If this muscular valve (oesophageal sphincter) does not work very well, the stomach juices can leak backwards into the gullet, causing reflux or symptoms of indigestion (heartburn). However, in some people, small amounts of stomach juice can spill even further back into the back of your throat, affecting the throat lining and your voice box (larynx) and causing irritation and hoarseness. This is known as laryngo pharyngeal reflux (LPR) or extra oesophageal reflux (EOR). Its common name is 'silent reflux' because many people do not experience any of the classic symptoms of heartburn or indigestion. Silent reflux can occur during the day or night, even if a person hasn't eaten anything. Usually, however, silent reflux occurs at night. What are the symptoms of silent reflux? The most common symptoms are: • A sensation of food sticking or a feeling of a lump in the throat. • A hoarse, tight or 'croaky' voice. • Frequent throat clearing. • Difficulty swallowing (especially tablets or solid foods). • A sore, dry and sensitive throat. • Occasional unpleasant "acid" or "bilious" taste at the back of the mouth. -

Bowel Function Anatomy
BOWEL FUNCTION ANATOMY Most of America gives little thought to bowel control. However, bowel control is actually a complex process involving the coordination of many different muscles and nerves. The bowel is considered to be a part of the digestive or gastrointestinal system. It is designed to help the body absorb nutrients and fluids from the foods we eat and drink. After taking out everything the body needs, the bowel then expels the leftover waste. The beginning of the bowel is the small intestine, sometimes referred to as the small bowel. This is where the useful nutrients are absorbed from what you eat. The small bowel delivers the waste to the colon, or large bowel. The colon is a 5-6 foot long muscular tube that delivers stool to the rectum. As the stool moves through the colon, the fluids are removed and absorbed into the body. The consistency of the stool is dependent upon many things, including how long the stool sits in the colon, how much of the water has been absorbed from the waste, and the amount of fiber and fluids in your diet. Stool consistency can vary from hard lumps to mushy to very loose, watery stool. The best and easiest consistency of stool is soft, like toothpaste; this consistency may be attained by adding fiber to your diet. Fiber helps move waste through the colon because it is indigestible by the human body. In other words, fiber adds ‘bulk’ to the stool. It is important to eat a diet high in fiber, however, most Americans lack fiber in their diet. -

Anal Sex an Informative Guide by Bedroom Kandi
AN INTRODUCTION TO ANAL SEX AN INFORMATIVE GUIDE BY BEDROOM KANDI Anal sex encompasses a variety of sexual acts involving the anus and rectum. These can include anal fingering, analingus (oral-anal sex, sometimes called “rimming”), anal insertion (using an object like a strap-on or other toy) and anal intercourse (penis-in-anus sex). Anal sex can be enjoyed by individuals of any gender, and any orientation. Everyone has a back door, after all! But it requires preparation, care, and patience to make it pleasurable. Communication is Key! No surprise butt-sex. Always check in with your partner, talk things through, and 36% communicate about whether you’re Of American Women both on board for trying anal. Check in during anal sex to report having tried ? make sure you’re both enjoying yourselves! ANAL SEX “Is Anal Sex Common?” International Society for Sexual Medicine :) http://www.issm.info/sexual-health-qa/is-anal-sex-common/ www.bedroomkandi.com ©2017 Bedroom Kandi WHY TRY ANAL? IT FEELS GOOD - There are a lot IT FEELS BAD - in a good way! The of nerve endings to stimulate around taboos around anal sex can make it a the anus, including those in the man’s thrill and add something exciting to your prostate. bedroom routine. You naughty thing! IT SPICES THINGS UP - Trying IT CAN SUBVERT GENDER new things keeps things fresh, and ROLES - Either partner can penetrate anal sex will open up a whole new or receive, (using strap-ons or other toys range of sexual positions and activities for Lesbian or Straight couples), so you for you and your partner to share. -

What's New in Stis?
WHAT’S NEW IN STIS? Sarah Weninger, HIV.STD.Viral Hepatitis Prevention Coordinator Division of Sexually Transmitted and Bloodborne Diseases January 27, 2021 OBJECTIVES ▪ Describe the updated gonorrhea treatment recommendations ▪ Identify the five goals of STI National Strategic Plan. ▪ Describe three strategies to implement for best practices for the prevention and treatment of STIs. GONORRHEA TREATMENT ▪ Combination therapy since 1985 ▪ Evidence and Rationale ▪ Antimicrobial Stewardship ▪ Pharmacokinetics ▪ Azithromycin Susceptibility 2020 UPDATE TO TREATMENT FOR GONOCOCCAL INFECTIONS. Uncomplicated urogenital, rectal or pharyngeal gonorrhea 500 mg IM Ceftriaxone* *For persons weighing ≥ 300 lbs, 1 g of IM Ceftriaxone should be administered 2020 UPDATE TO TREATMENT FOR GONOCOCCAL INFECTIONS. Uncomplicated urogenital, rectal or pharyngeal gonorrhea 500 mg IM Ceftriaxone^ + Doxycycline 100 mg orally BID * 7 Days (If Chlamydia is NOT ruled out) ^For persons weighing ≥ 300 lbs, 1 g of IM Ceftriaxone should be administered AZITHROMYCIN IS PREGNANT INDIVIDUALS WITH GONORRHEA AND CHLAMYDIA NOT RULED OUT. Uncomplicated urogenital, rectal or pharyngeal gonorrhea 500 mg IM Ceftriaxone^ + 1 G Azithromycin 2020 UPDATE TO TREATMENT FOR GONOCOCCAL INFECTIONS. Uncomplicated urogenital, rectal or pharyngeal gonorrhea - Cephalosporin Allergy 240 mg IM dose of Gentamicin + Single 2 g Oral Dose of Azithromycin EPT CAN STILL BE USED FOR GONORRHEA. Uncomplicated urogenital, rectal or pharyngeal gonorrhea Single 800 mg Oral Dose of Cefixime + Doxycycline 100 -

Larynx, Hypopharynx and Mandible Injury Due to External Penetrating Neck Injury
Turkish Journal of Trauma & Emergency Surgery Ulus Travma Acil Cerrahi Derg 2013;19 (3):271-273 Case Report Olgu Sunumu doi: 10.5505/tjtes.2013.58259 Larynx, hypopharynx and mandible injury due to external penetrating neck injury Eksternal penetran boyun yaralanmasına bağlı gelişen larinks, hipofarinks ve mandibula yaralanması Gül ÖZBİLEN ACAR, Muhammet TEKİN, Osman H. ÇAM, Emre KAYTANCI Esophageal and laryngeal injuries due to ballistic injuries are Blastik travmalara bağlı özöfageal ve laringeal yaralanma- seldom encountered. Ballistic external neck traumas gener- lar nadir görülürler. Blastik travmalara bağlı gelişen dış ally result in death. Incidence of external penetrant neck boyun travmaları genellikle ölümle sonuçlanır. Penetran injuries may vary between 1/5000-137000 patients among dış boyun travmalarının acil servise başvuran hastalar ara- emergency service referrals. Vascular injuries, esophagus- sındaki insidansı 1/5000-137000 arasında değişmektedir. hypopharynx perforations, laryngotracheal injuries, bony Dış boyun travmalarında vasküler yaralanmalar, özofa- fractures, and segmentations may be encountered in exter- gus-hipofarenks perforasyonları, laringotrakeal yaralan- nal neck traumas. Here we report a 27-year-old male pa- malar, kemik yapılarda kırık ve parçalanmalar görülebilir. tient who was referred to our emergency department and Bu yazıda, eksternal blastik boyun travmasına bağlı ola- presented with hyoid bone fracture, multiple mandibular rak acil servise başvuran hiyoid kırığı, multipl mandibula fractures, and hypopharynx -
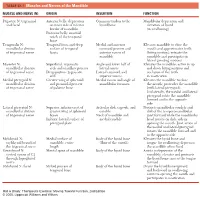
1 TABLE 23-1 Muscles and Nerves of the Mandible
0350 ch 23-Tab 10/12/04 12:19 PM Page 1 Chapter 23: The Temporomandibular Joint 1 TABLE 23-1 Muscles and Nerves of the Mandible MUSCLE AND NERVE (N) ORIGIN INSERTION FUNCTION Digastric N: trigeminal Anterior belly: depression Common tendon to the Mandibular depression and and facial on inner side of inferior hyoid bone elevation of hyoid border of mandible (in swallowing) Posterior belly: mastoid notch of the temporal bone Temporalis N: Temporal fossa and deep Medial and anterior Elevates mandible to close the mandibular division surface of temporal coronoid process and mouth and approximates teeth of trigeminal nerve fascia anterior ramus of (biting motion); retracts the mandible mandible and participates in lateral grinding motions Masseter N: Superficial: zygomatic Angle and lower half of Elevates the mandible; active in up mandibular division arch and maxillary process lateral ramus and down biting motions and of trigeminal nerve Deep portion: zygomatic Lateral coronoid and occlusion of the teeth arch superior ramus in mastication Medial pterygoid N: Greater wing of sphenoid Medial ramus and angle of Elevates the mandible to close mandibular division and pyramidal process mandibular foramen the mouth; protrudes the mandible of trigeminal nerve of palatine bone (with lateral pterygoid). Unilaterally, the medial and lateral pterygoid rotate the mandible forward and to the opposite side Lateral pterygoid N: Superior: inferior crest of Articular disk, capsule, and Protracts mandibular condyle and mandibular division greater wing of sphenoid condyle disk of the temporomandibular of trigeminal nerve bones Neck of mandible and joint forward while the mandibular Inferior: lateral surface of medial condyle head rotates on disk; aids in pterygoid plate opening the mouth.