Official American Thoracic Society/Centers for Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Browser Wars
Uppsala universitet Inst. för informationsvetenskap Browser Wars Kampen om webbläsarmarknaden Andreas Högström, Emil Pettersson Kurs: Examensarbete Nivå: C Termin: VT-10 Datum: 2010-06-07 Handledare: Anneli Edman "Anyone who slaps a 'this page is best viewed with Browser X' label on a Web page appears to be yearning for the bad old days, before the Web, when you had very little chance of read- ing a document written on another computer, another word processor, or another network" - Sir Timothy John Berners-Lee, grundare av World Wide Web Consortium, Technology Review juli 1996 Innehållsförteckning Abstract ...................................................................................................................................... 1 Sammanfattning ......................................................................................................................... 2 1 Inledning .................................................................................................................................. 3 1.1 Bakgrund .............................................................................................................................. 3 1.2 Syfte ..................................................................................................................................... 3 1.3 Frågeställningar .................................................................................................................... 3 1.4 Avgränsningar ..................................................................................................................... -

Aquatic Microbial Ecology 75:117
Vol. 75: 117–128, 2015 AQUATIC MICROBIAL ECOLOGY Published online June 4 doi: 10.3354/ame01752 Aquat Microb Ecol Metagenomic assessment of viral diversity in Lake Matoaka, a temperate, eutrophic freshwater lake in southeastern Virginia, USA Jasmin C. Green1, Faraz Rahman1, Matthew A. Saxton2,3, Kurt E. Williamson1,2,* 1Department of Biology, College of William & Mary, Williamsburg, Virginia 23185, USA 2Environmental Science and Policy Program, College of William & Mary, Williamsburg, Virginia 23185, USA 3Present address: Department of Marine Sciences, University of Georgia, Athens, Georgia 30602, USA ABSTRACT: Little is known about the composition and diversity of temperate freshwater viral communities. This study presents a metagenomic analysis of viral community composition, taxo- nomic and functional diversity of temperate, eutrophic Lake Matoaka in southeastern Virginia (USA). Three sampling sites were chosen to represent differences in anthropogenic impacts: the Crim Dell Creek mouth (impacted), the Pogonia Creek mouth (less impacted) and the main body of the lake (mixed). Sequences belonging to tailed bacteriophages were the most abundant at all 3 sites, with Podoviridae predominating. The main lake body harbored the highest virus genotype richness and included cyanophage and eukaryotic algal virus sequences not found at the other 2 sites, while the impacted Crim Dell Creek mouth showed the lowest richness. Cross-contig com- parisons indicated that similar virus genotypes were found at all 3 sites, but at different rank- abundances. Hierarchical cluster analysis of multiple viral metagenomes indicated high genetic similarity between viral communities of related environments, with freshwater, marine, hypersaline, and eukaryote-associated environments forming into clear groups despite large geographic dis- tances between sampling locations within each environment type. -

Discontinued Browsers List
Discontinued Browsers List Look back into history at the fallen windows of yesteryear. Welcome to the dead pool. We include both officially discontinued, as well as those that have not updated. If you are interested in browsers that still work, try our big browser list. All links open in new windows. 1. Abaco (discontinued) http://lab-fgb.com/abaco 2. Acoo (last updated 2009) http://www.acoobrowser.com 3. Amaya (discontinued 2013) https://www.w3.org/Amaya 4. AOL Explorer (discontinued 2006) https://www.aol.com 5. AMosaic (discontinued in 2006) No website 6. Arachne (last updated 2013) http://www.glennmcc.org 7. Arena (discontinued in 1998) https://www.w3.org/Arena 8. Ariadna (discontinued in 1998) http://www.ariadna.ru 9. Arora (discontinued in 2011) https://github.com/Arora/arora 10. AWeb (last updated 2001) http://www.amitrix.com/aweb.html 11. Baidu (discontinued 2019) https://liulanqi.baidu.com 12. Beamrise (last updated 2014) http://www.sien.com 13. Beonex Communicator (discontinued in 2004) https://www.beonex.com 14. BlackHawk (last updated 2015) http://www.netgate.sk/blackhawk 15. Bolt (discontinued 2011) No website 16. Browse3d (last updated 2005) http://www.browse3d.com 17. Browzar (last updated 2013) http://www.browzar.com 18. Camino (discontinued in 2013) http://caminobrowser.org 19. Classilla (last updated 2014) https://www.floodgap.com/software/classilla 20. CometBird (discontinued 2015) http://www.cometbird.com 21. Conkeror (last updated 2016) http://conkeror.org 22. Crazy Browser (last updated 2013) No website 23. Deepnet Explorer (discontinued in 2006) http://www.deepnetexplorer.com 24. Enigma (last updated 2012) No website 25. -

Microbetrace: Retooling Molecular Epidemiology for Rapid Public Health Response
bioRxiv preprint doi: https://doi.org/10.1101/2020.07.22.216275; this version posted July 24, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. This article is a US Government work. It is not subject to copyright under 17 USC 105 and is also made available for use under a CC0 license. 1 Title: MicrobeTrace: Retooling Molecular Epidemiology for Rapid Public Health Response 2 Authors: Ellsworth M. Campbell1,*, Anthony Boyles2,, Anupama Shankar1, Jay Kim 2, Sergey 3 Knyazev1,3,4, William M. Switzer1 4 Affiliations 5 1Centers for Disease Control and Prevention, Atlanta, GA 30329 6 2Northrup Grumman, Atlanta, GA 30345 7 3Oak Ridge Institute for Science and Education, Oak Ridge, TN 37830 8 4Department of Computer Science, Georgia State University, Atlanta, GA, 30303 9 Title character count (with spaces): 71 10 Abstract word count: 165 (of limit 150) 11 Manuscript word count, excluding figure captions: 4552 (of limit 5000) 12 Figure caption word count: 490 13 Conflicts of Interest and Source of Funding: None 14 * To whom correspondence should be addressed. 15 Authors contributed equally. 16 Abstract 17 Motivation 18 Outbreak investigations use data from interviews, healthcare providers, laboratories and surveillance 19 systems. However, integrated use of data from multiple sources requires a patchwork of software that 20 present challenges in usability, interoperability, confidentiality, and cost. Rapid integration, visualization 21 and analysis of data from multiple sources can guide effective public health interventions. 22 Results 23 We developed MicrobeTrace to facilitate rapid public health responses by overcoming barriers to data 24 integration and exploration in molecular epidemiology. -
BIJOU BROWSER Sirer, Fotolia .Com
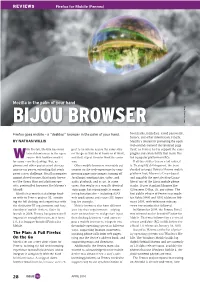
RevIews Firefox for Mobile (Fennec) Mozilla in the palm of your hand BIJOU BROWSER .com Fotolia Sirer, Firefox goes mobile – a “desktop” browser in the palm of your hand. bookmarks, form data, saved passwords, history, and other information. Finally, BY NATHAN WILLIS Mozilla’s interest in promoting the open web extends beyond the rendered page ith Firefox, Mozilla has main- pect to be able to access the same sites itself, so Fennec had to support the same tained dominance in the open on the go as they do at home or at work, plugins and extensibility that make Fire- wsource web browser market and they expect them to work the same fox a popular platform on PCs. for years – on the desktop. But, as way. If all this strikes you as a tall order, it phones and other pocket-sized devices Other mobile browsers invariably cut is. To simplify development, the team increase in power, extending that reach corners on the web experience by com- decided to target Nokia’s Maemo mobile poses a new challenge. Mozilla competes pressing pages into images; turning off platform first; Maemo is Linux-based against closed source, third-party brows- JavaScript; omitting tabs, video, and and arguably the most desktop-Linux- ers like Opera Mini and platform-spe- audio playback; and so on. In some like of any of the Linux mobile phone cific, preinstalled browsers like Maemo’s cases, this results in a visually identical stacks. It uses standard libraries like MicroB. static page, but increasingly, it means GStreamer, D-Bus, Qt, any others. -

Chemical Communication in Songbirds
Western University Scholarship@Western Electronic Thesis and Dissertation Repository 4-15-2020 10:30 AM Chemical Communication in Songbirds Leanne A. Grieves The University of Western Ontario Supervisor MacDougall-Shackleton, Elizabeth A. The University of Western Ontario Graduate Program in Biology A thesis submitted in partial fulfillment of the equirr ements for the degree in Doctor of Philosophy © Leanne A. Grieves 2020 Follow this and additional works at: https://ir.lib.uwo.ca/etd Part of the Behavior and Ethology Commons, Integrative Biology Commons, and the Molecular Genetics Commons Recommended Citation Grieves, Leanne A., "Chemical Communication in Songbirds" (2020). Electronic Thesis and Dissertation Repository. 6926. https://ir.lib.uwo.ca/etd/6926 This Dissertation/Thesis is brought to you for free and open access by Scholarship@Western. It has been accepted for inclusion in Electronic Thesis and Dissertation Repository by an authorized administrator of Scholarship@Western. For more information, please contact [email protected]. Abstract Avian chemical communication has been understudied due to the misconception that olfaction is unimportant or even lacking in birds. Early work focused on the olfactory foraging capabilities of seabirds because of their ecology (open ocean foraging) and large olfactory bulbs. In contrast, olfaction in passerine birds, comprising over half of all extant avian taxa, was long overlooked due to their relatively small olfactory bulbs. It is now well established that passerines can smell, and their olfactory acuity is comparable to that of macrosmatic mammals such as rats. Much of our theory on communication and mate choice has involved studying visual and acoustic signals in birds, especially passerines. -

Fall 1998 Fee Charts
2 1998-99 Annual Schedule of Classes What’s New? Bruin Direct now required for credit balance refunds UCLA now requires direct deposit for all credit balance refunds in BAR. If you are not currently enrolled in Bruin Direct, and did not receive an authorization form in the mail, pick up an authorization form from the Administrative Main Cashier Office at 1125 Murphy Hall or Student Ac- counting at B303 Murphy Hall. Enhanced features for online Schedule of Classes Now the UCLA online Schedule of Classes, at http://www.registrar.ucla.edu/schedule, includes powerful new search capabilities to let students easily find the courses they are looking for and the courses they need. Whether targeting courses that fulfill GE requirements or looking for something to fit into a busy work schedule, students have a range of options that make searching a snap. In addition, beginning week nine of the quarter, students can link directly to final examination information — including exam code, date and time, and location — from their individual course selections in the online class listings. Library launches Web-based Orion2 As the UCLA Library replaces the Orion catalog system with Orion2, 1998-99 students will be among the first to have access to the World Wide Web-based system. Orion2 can also serve anyone anywhere in the world who has access to a Web browser. The system has the capability of searching databases other than the UCLA catalog and including active links to a variety of relevant Web resources. Check out the new changes at www.library.ucla.edu. -

Developing Hybrid Web/GTK+ Rich Internet Applications
WebKit GTK+ Developing hybrid Web/GTK+ rich internet applications February 2008 FOSDEM Brussels Alp Toker JavaScriptCore WebCore portable C API content engine WebKit GObject API GTK+ applications C, C#, C++, Vala, Python WebKit language bindings Vala bindings Language binding features – Maintained by Jürg Billeter 1 – Covers core API WebKit widget Python bindings and related classes – Created by the OLPC team 2 – Maintained by Jan Alonzo DOM binding C#/CLR bindings (WIP) – JS bridge available 3 JavaScript runtime JavaScript bindings bridge – DOM only (part of JavaScriptCore) Introducing WebView Write a browser in a dozen lines import gtk import webkit view = webkit.WebView() sw = gtk.ScrolledWindow() sw.add(view) win = gtk.Window(gtk.WINDOW_TOPLEVEL) win.add(sw) win.show_all() view.open("http://planet.gnome.org/") gtk.main() WebView modes: Scrollable Packed in a GtkScrolledWindow – Provides a full-featured browser engine for document display and editing WebView modes: Packed Packed directly into the UI – Acts as an integral part of the surrounding GTK+ UI – Place Web content in amongst GTK+ widgets Web content / GTK+ size request interop (landing soon) Develop and design in parallel ● Let programmers work on the core ● Let designers produce UI elements using Web skills When to use a WebView When do you use straight GTK+? When does Web content enrich the experience? Great power; great responsibility WebView isn't the right tool for every job – Continue to use GtkTextView for light viewing and editing – Use GtkTreeView and GtkIconView unless -
Advances in Visualization Tools for Phylogenomic and Phylodynamic Studies of Viral Diseases
REVIEW published: 02 August 2019 doi: 10.3389/fpubh.2019.00208 Advances in Visualization Tools for Phylogenomic and Phylodynamic Studies of Viral Diseases Kristof Theys, Philippe Lemey, Anne-Mieke Vandamme and Guy Baele* Department of Microbiology, Immunology and Transplantation, Rega Institute for Medical Research, Clinical and Epidemiological Virology, KU Leuven, Leuven, Belgium Genomic and epidemiological monitoring have become an integral part of our response to emerging and ongoing epidemics of viral infectious diseases. Advances in high-throughput sequencing, including portable genomic sequencing at reduced costs and turnaround time, are paralleled by continuing developments in methodology to infer evolutionary histories (dynamics/patterns) and to identify factors driving viral spread in space and time. The traditionally static nature of visualizing phylogenetic trees that represent these evolutionary relationships/processes has also evolved, albeit perhaps at a slower rate. Advanced visualization tools with increased resolution assist in drawing conclusions from phylogenetic estimates and may even have potential to better inform Edited by: public health and treatment decisions, but the design (and choice of what analyses Vitali Sintchenko, are shown) is hindered by the complexity of information embedded within current University of Sydney, Australia phylogenetic models and the integration of available meta-data. In this review, we discuss Reviewed by: Denis Baurain, visualization challenges for the interpretation and exploration -
End of Year Progress Report Overview
DOE Joint Genome Institute FY15 - End of Year Progress Report Overview The present FY15 End-of-Year Progress Report concludes the FY15 series of “Quarterly Metrics” progress reports from the JGI in which we described several new experimental or computational capabilities for the assembly, analysis, and functional annotation of genomes. The topic of the Q1 report was “New computational developments for improving microbial, metagenomic, or plant genome assemblies”. We described the development of Meraculous2, a state- of-the-art de novo assembler for short reads; its parallelization for use in high performance computing settings; the development of efficient methods for shotgun genetic mapping; whole-genome shotgun assembly of hexaploid wheat; and the development of merAligner, a highly parallel sequence aligner. In Q2, we reported on “Progress developing new experimental capabilities to analyze complex genomic or metagenomic datasets.” We described the development of a general strategy for the genome-wide functional annotation of microbial genes using saturation transposon mutagenesis, followed by sequencing (TnSeq). In particular, we reported on the implementation of a new random barcode- enabled transposon site-sequencing approach (RB-TnSeq) and its application in the context of the Functional Encyclopedia of Bacteria and Archaea (FEBA) project. A report on “New computational approaches for the annotation of genomic data,” published in Q3, described the development of ProDeGe, a fully automated protocol for decontamination of single amplified genomes derived from single uncultivated microbial cells, as well as genomes assembled from metagenomic data. In Q4, we provided a report on a “New computational method for improving the interpretation of microbial, metagenomic, or plant genomes.” We described the development of a new data mart for the Integrated Microbial Genomes (IMG) resource, the Atlas of Biosynthetic gene Clusters (IMG-ABC). -
Frontend Day Workshop
The mobile browser world Peter-Paul Koch http://quirksmode.org http://twitter.com/ppk Front-end Day workshop, 26 April 2011 1 Mobile First! • Luke Wroblewski invented it • Design your sites for mobile first. • You’ll be forced to decide what is so important that it MUST be shown in the mobile device’s tiny display. • The things you leave out of the mobile version don’t really need to be in the desktop version, either. 2 The mobile browsers • Safari iPhone • Obigo WebKit • Android WebKit • Ovi • Dolfin for bada • Palm WebKit • BlackBerry WebKit • BlackBerry old • Opera Mobile • Phantom • Opera Mini • Obigo old • MicroB • NetFront • Nokia WebKit • IE • Firefox • UCWeb You may groan now. 3 The mobile browsers • Safari iPhone • Obigo WebKit • Android WebKit • Ovi • Dolfin for bada • Palm WebKit • BlackBerry WebKit • BlackBerry old • Opera Mobile • Phantom • Opera Mini • Obigo old • MicroB • NetFront • Nokia WebKit • IE • Firefox • UCWeb Gecko-based 4 The mobile browsers • Safari iPhone • Obigo WebKit • Android WebKit • Ovi • Dolfin for bada • Palm WebKit • BlackBerry WebKit • BlackBerry old • Opera Mobile • Phantom • Opera Mini • Obigo old • MicroB • NetFront • Nokia WebKit • IE • Firefox • UCWeb Presto-based 5 The mobile browsers • Safari iPhone • Obigo WebKit • Android WebKit • Ovi • Dolfin for bada • Palm WebKit • BlackBerry WebKit • BlackBerry old • Opera Mobile • Phantom • Opera Mini • Obigo old • MicroB • NetFront • Nokia WebKit • IE • Firefox • UCWeb Other rendering engines 6 The mobile browsers • Safari iPhone • Obigo WebKit • Android WebKit • Ovi • Dolfin for bada • Palm WebKit • BlackBerry WebKit • BlackBerry old • Opera Mobile • Phantom • Opera Mini • Obigo old • MicroB • NetFront • Nokia WebKit • IE • Firefox • UCWeb WebKit-based 7 WebKit on Mobile There is no WebKit on mobile! There's iPhone Safari (3 and 4), and Android (2.1 and 2.3 and 3.0), and Nokia WebKit (S40 and Symbian), and BlackBerry WebKit, and Dolfin for bada, and Palm, and Obigo, and a few more These WebKits are all diferent. -

Xe922-3GR Starting Guide
xE922-3GR Starting Guide 1VV0301316 Rev.1- 2017-07-04 xE922-3GR Starting Guide 1VV0301316 Rev.1 2017-07-04 APPLICABILITY TABLE PRODUCT HE922-3GR WE922-3GR APPLICABILITY TABLE 1 Reproduction forbidden without written authorization from Telit Communications S.p.A. - All Rights Reserved. Page 2 of 61 xE922-3GR Starting Guide 1VV0301316 Rev.1 2017-07-04 SPECIFICATIONS SUBJECT TO CHANGE WITHOUT NOTICE Notice While reasonable efforts have been made to assure the accuracy of this document, Telit assumes no liability resulting from any inaccuracies or omissions in this document, or from use of the information obtained herein. The information in this document has been carefully checked and is believed to be entirely reliable. However, no responsibility is assumed for inaccuracies or omissions. Telit reserves the right to make changes to any products described herein and reserves the right to revise this document and to make changes from time to time in content hereof with no obligation to notify any person of revisions or changes. Telit does not assume any liability arising out of the application or use of any product, software, or circuit described herein; neither does it convey license under its patent rights or the rights of others. It is possible that this publication may contain references to, or information about Telit products (machines and programs), programming, or services that are not announced in your country. Such references or information must not be construed to mean that Telit intends to announce such Telit products, programming, or services in your country. Copyrights This instruction manual and the Telit products described in this instruction manual may be, include or describe copyrighted Telit material, such as computer programs stored in semiconductor memories or other media.