Annual Report 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Koto Walking Map in Your Hand! Swing Your Arms Rhythmically in Time with Your Feet
Koto City, a warm-hearted town with a passion for sports FAQs about Walking Let’s start walking to keep you healthy. Enjoy walking without injury, in a good posture, and healthily Why don’t you try getting healthy and enjoy sightseeing spots in Q What is the proper walking form? A ▶▶▶ Pull your chin in and Stay upright and Koto City at the same time? look straight ahead puff out your chest We have created attractive 14 courses with the cooperation of residents who routinely walk for exercise. Let’s walk Koto City with the Koto Walking Map in your hand! Swing your arms rhythmically in time with your feet Put your heel on the ground first Then walk with a heel stride Kick the ground of about 5 to 7 cm bigger than usual with the base of your big toe Q When is a good time to hydrate ourselves? A ▶▶▶ ■1 Get hydrated frequently before feeling thirsty, such as before, during and after walking. ■2 As for what you drink, water is basically OK. It is better if you can also get an adequate amount of minerals (such as salt). ■3 Beverages containing caffeine, which has a diuretic effect such as coffee or tea, are not suitable for hydrating. Good things about walking Walking Style Calorie consumption by walking Before/After Walking What are the benefits of walking? What are appropriate clothes for walking? How many calories are consumed? How should we warm up before walking? FAQs about Q Q Q Q ▶▶▶ ■1 Prevent lifestyle-related ▶▶▶ ■1 Shirts and pants that dry quickly and absorb ▶▶▶ ■1 10-minute walking= calorie ▶▶▶ ■1 Stretch to warm up your body gradually and Walking A A A A diseases moisture well. -

Suica Pasmo Network
To Matō Kassemba Ienaka Tōbu-kanasaki Niregi Momiyama Kita-kanuma Itaga Shimo-goshiro Myōjin Imaichi Nikkō Line To Aizu-Wakamatsu To Sendai To Fukushima Jōban Line To Haranomachi Watarase Keikoku Railway Nikkō Ban-etsu-East Line Shin-kanuma Niigata Area Akagi Tanuma Tada Tōbu Nikkō Line Minami- Tōbu-nikkō Iwaki / Network Map To Chuo-Maebashi ※3 To Kōriyama Kuzū Kami- Uchigō To Murakami ★ Yashū-ōtsuka Kuniya Omochanomachi Nishikawada Esojima utsunomiya Tōhoku Line Tōbu Sano Line TsurutaKanumaFubasami Shin-fujiwara Jomo Electric Railway Yoshimizu Shin-tochigi Shimo- imaichi Shin-takatokuKosagoeTobu WorldKinugawa-onsen SquareKinugawa-kōen Yumoto ■Areas where Suica /PASMO can be used Yashū-hirakawa Mibu Tōbu Utsunomiya Line Yasuzuka Kuroiso Shibata Tōhoku Tōhoku Shinkansen imaichi Line Aizu Kinugawa Aioi Nishi-Kiryu Horigome Utsunomiya Line Shimotsuke-Ōsawa Tōbu Kinugawa Line Izumi Daiyamukō Ōkuwa Railway Yagantetsudo To Naoetsu To Niigata Omata YamamaeAshikagaAshikaga TomitaFlower Park Tōbu-utsunomiya Ueda Yaita Nozaki Nasushiobara Nishi-Shibata Nakaura Echigo TOKImeki Railway Ishibashi Suzumenomiya Nakoso Kunisada Iwajuku Shin-kiryū Kiryū Ryōmō Line Sano Iwafune Ōhirashita Tochigi Omoigawa To Naganoharakusatsuguchi ShikishimaTsukudaIwamotoNumataGokan KamimokuMinakami Shin-ōhirashita Jichi Medical Okamoto Hōshakuji Karasuyama Ujiie Utsunomiya Kamasusaka Kataoka Nishi-Nasuno Ōtsukō Sasaki To Echigo-Yuzawa Azami Sanoshi To Motegi Utsunomiya Line Line Uetsu LineTsukioka Jōmō-Kōgen ★ Shizuwa University Isohara Shibukawa Jōetsu Line Yabuzuka -

The Preservation of Railway Heritage in Japan: an Outline History and General View Eiichi Aoki
Feature Heritage Railways The Preservation of Railway Heritage in Japan: An Outline History and General View Eiichi Aoki works of Nippon Railway—the first private Introduction Prewar Railway Museums railway; and two early Imperial carriages. The railway museum was provisionally The first railway museum in Japan was The first railway in Japan, owned and opened in 1921 at Tokyo Station, but opened in 1921, but the first museum for operated by the Japanese government, found its final location in 1936 at preservation of steam locomotives in was opened between Shimbashi in Tokyo Mansebashi Station, the former working order was opened in 1972, as and Yokohama in 1872 with the technical temporary terminus of the Chuo Line. the Umekoji Steam Locomotive Museum. leadership of British engineers. Most of (The station was later abandoned in Although the last steam trains on the materials for railway construction and 1943.) This was the sole museum related Japanese National Railways (JNR) ceased rolling stock were imported from Britain, to railway history in prewar days, and it commercial operations in 1975, regular but American and German manufacturers was reorganized as the Transport steam operations restarted in the soon became suppliers to Japanese Museum after WWII. following year on Oigawa Railway, a railways. Private railways extended their private rural railway in Shizuoka main-line network from 1883 but most Preservation of Steam Locos Prefecture. The revival of steam were nationalized in 1906–07. in 1950s and 1960s locomotive means a creation of new In 1911, a railway museum project was tourism resources, as well as preservation started and began preserving railway From the latter half of the 1950s, Japan of railway heritage in regional societies. -

List of Airports by IATA Code: a Wikipedia, the Free Encyclopedia List of Airports by IATA Code: a from Wikipedia, the Free Encyclopedia
9/8/2015 List of airports by IATA code: A Wikipedia, the free encyclopedia List of airports by IATA code: A From Wikipedia, the free encyclopedia List of airports by IATA code: A B C D E F G H I J K L M N O P Q R S T U V W X Y Z See also: List of airports by ICAO code A The DST column shows the months in which Daylight Saving Time, a.k.a. Summer Time, begins and ends. A blank DST box usually indicates that the location stays on Standard Time all year, although in some cases the location stays on Summer Time all year. If a location is currently on DST, add one hour to the time in the Time column. To determine how much and in which direction you will need to adjust your watch, first adjust the time offsets of your source and destination for DST if applicable, then subtract the offset of your departure city from the offset of your destination. For example, if you were flying from Houston (UTC−6) to South Africa (UTC+2) in June, first you would add an hour to the Houston time for DST, making it UTC−5, then you would subtract 5 from +2. +2 (5) = +2 + (+5) = +7, so you would need to advance your watch by seven hours. If you were going in the opposite direction, you would subtract 2 from 5, giving you 7, indicating that you would need to turn your watch back seven hours. Contents AA AB AC AD AE AF AG AH AI AJ AK AL AM AN AO AP AQ AR AS AT AU AV AW AX AY AZ https://en.wikipedia.org/wiki/List_of_airports_by_IATA_code:_A 1/24 9/8/2015 List of airports by IATA code: A Wikipedia, the free -

Chapter 3 Aircraft Accident and Serious Incident Investigations
Chapter 3 Aircraft accident and serious incident investigations Chapter 3 Aircraft accident and serious incident investigations 1 Aircraft accidents and serious incidents to be investigated <Aircraft accidents to be investigated> ◎Paragraph 1, Article 2 of the Act for Establishment of the Japan Transport Safety Board (Definition of aircraft accident) The term "Aircraft Accident" as used in this Act shall mean the accident listed in each of the items in paragraph 1 of Article 76 of the Civil Aeronautics Act. ◎Paragraph 1, Article 76 of the Civil Aeronautics Act (Obligation to report) 1 Crash, collision or fire of aircraft; 2 Injury or death of any person, or destruction of any object caused by aircraft; 3 Death (except those specified in Ordinances of the Ministry of Land, Infrastructure, Transport and Tourism) or disappearance of any person on board the aircraft; 4 Contact with other aircraft; and 5 Other accidents relating to aircraft specified in Ordinances of the Ministry of Land, Infrastructure, Transport and Tourism. ◎Article 165-3 of the Ordinance for Enforcement of the Civil Aeronautics Act (Accidents related to aircraft prescribed in the Ordinances of the Ministry of Land, Infrastructure, Transport and Tourism under item 5 of the paragraph1 of the Article 76 of the Act) The cases (excluding cases where the repair of a subject aircraft does not correspond to the major repair work) where navigating aircraft is damaged (except the sole damage of engine, cowling, engine accessory, propeller, wing tip, antenna, tire, brake or fairing). <Aircraft serious incidents to be investigated> ◎Item 2, Paragraph 2, Article 2 of the Act for Establishment of the Japan Transport Safety Board (Definition of aircraft serious incident) A situation where a pilot in command of an aircraft during flight recognized a risk of collision or contact with any other aircraft, or any other situations prescribed by the Ordinances of Ministry of Land, Infrastructure, Transport and Tourism under Article 76-2 of the Civil Aeronautics Act. -

Construction of Ueno–Tokyo Line
Special Feature Construction of Ueno–Tokyo Line JR East Construction Department Introduction to support through services between the Utsunomiya, Takasaki, Joban, and Tokaido lines (Fig. 1). The Council East Japan Railway Company (JR East) has a wide-ranging for Transport Policy Report No. 18 published in January operations area from Kanto and Koshin’etsu to Tohoku. When 2000, targeted opening of the Ueno–Tokyo Line (A1) by JR East was established in 1987, traffic conditions on most 2015. In November 2007, the Minister of Transport gave sections of conventional (narrow-gauge) lines in the Tokyo permission to change the basic plan to a plan for laying area, including major sections of lines radiating from central new tracks between Tokyo Station and Ueno Station and Tokyo (Tokaido, Chuo, Joban, Sobu lines), the Yamanote then permission was given in March 2008 to change the Line, etc., had morning rush-hour congestion rates in excess railway facilities. Construction started in May 2008 and was of 200%. As a result, enhancing transportation capacity completed in about 6 years. The line opened on 14 March to alleviate congestion was a major issue. Furthermore, 2015, following 5–month training run. with subsequent diversification of values accompanying social changes, users’ railway needs went beyond merely Expected Effects alleviating congestion to shorter travel times and improved comfort while travelling, etc., so problems related to Alleviating congestion on Yamanote and Keihin-Tohoku improving transportation in the Tokyo area also diversified. In lines this context, JR East has taken various initiatives to improve The sections between Ueno Station and Okachimachi the quality of railway services. -
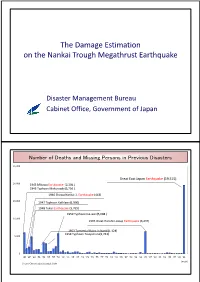
The Damage Estimation on the Nankai Trough Megathrust
The Damage Estimation onthen the Nankai Trough Megathrust Earthquake Disaster Management Bureau Cabinet Office, Government of Japan Number of Deaths and Missing Persons in Previous Disasters 25, 000 Great East Japan Earthquake (19,515) 20,000 1945 Mikawa Earthquake (2,306 ) 1945 Typhoon Makurazaki(3,756 ) 1946 Showa Nankai 1, Earthquake (443) 15,000 1947 Typhoon Kathleen(1,930) 1948 Fukui Earthquake (3,769) 1959 Typhoon Ise-wan(5,098 ) 10,000 1995 Great Hanshin-Awaji Earthquake (6,437) 1953 Torrential Rains in Nanki(1,124) 1954 Typhoon Touyamaru(1,761) 5,000 0 '45 '47 '49 '51 '53 '55 '57 '59 '61 '63 '65 '67 '69 '71 '73 '75 '77 '79 '81 '83 '85 '87 '89 '91 '93 '95 '97 '99 '01 '03 '05 '07 '09 '11 (year) Source: Chronological Scientific Table Large Earthquakes Reviewed by the Central Disaster Management Council Super wide-area earthquake extending to western Japan Tokikai Eart hqua ke Huge tsunami over 20 meters Tonankai, Nankai Earthquake Rate of earthquake production over 30 years: Oceanic-type earthquakes 60 ~ 70% in the vicinity of the Japan and Chishima Trenches Concerns about neglected timber buildings and Unknown ( Miyagi offshore cultural assets earthquake production rate over 30 years: 99% prior to the Great East Cyubu region, Kinki region Japan Earthquake) Inland Earthquake Concern about critical national operations Tokyyqo Inland Earthquake Rate of earthquake production over 30 years: approx 70% (Magnitude 7 in southern Kanto area) Oceanic earthquake Inland earthquake Rate of earthquake occurrence is by Ministry of Education, Culture, Sports, Science and Technology Planning and Review for Countermeasures Against Earthquakes (1) Estimate distribution of seismic intensity, tsunami height, etc. -

Chapter 3 Railway Accident and Serious Incident Investigation
Chapter 3 Railway accident and serious incident investigation Chapter 3 Railwayroad 第3章 accident 鉄道事故等調査活動and serious incident investigation 1. Railway accidents and serious incidents to be investigated <Railway accidents to be investigated> ◎ Paragraph 3, Article 2 of the Act for Establishment of the Japan Transport Safety Board (Definition of railway accident) The term "Railway Accident" as used in this Act shall mean a serious accident prescribed by the Ordinance of Ministry of Land, Infrastructure, Transport and Tourism among those of the following kinds of accidents; an accident that occurs during the operation of trains or vehicles as provided in Article 19 of the Railway Business Act, collision or fire involving trains or any other accidents that occur during the operation of trains or vehicles on a dedicated railway, collision or fire involving vehicles or any other accidents that occur during the operation of vehicles on a tramway. ◎ Article 1 of Ordinance for Enforcement of the Act for Establishment of the Japan Transport Safety Board (Serious accidents prescribed by the Ordinance of Ministry of Land, Infrastructure, Transport and Tourism, stipulated in paragraph 3, Article 2 of the Act for Establishment of the Japan Transport Safety Board) 1. The accidents specified in items 1 to 3 inclusive of paragraph 1 of Article 3 of the Ordinance on Report on Railway Accidents, etc. (the Ordinance); 2. From among the accidents specified in items 4 to 6 inclusive of paragraph 1 of Article 3 of the Ordinance, that which falls under any of the following sub-items: (a) an accident involving any passenger, crew, etc. -

Asia Pacific Region Infrastructure Report 2017
2017 ASIA PACIFIC REGION INFRASTRUCTURE REPORT 2017 INFRASTRUCTURE REPORT | I Beijing Seoul Penglai Chengdu Shanghai Shenzhen Hong Kong Bangkok Manila ABOUT ASIAN SKY GROUP ASIAN SKY GROUP (ASG), headquartered in Hong Kong and with offices throughout Asia, has assembled the most experienced aviation team in the Asia Pacific region to provide a wide range of independent services for both fixed and rotary-wing aircraft. ASG also provides access to a significant customer base around the world with the help of its exclusive partners. ASG provides its clients with the following business aviation services: Sales & Acquisitions | Market Research and Consulting | Operational Oversight | Luxury Charter Services The acclaimed Asian Sky Fleet Reports are produced by ASG’s market research and consulting team, in collaboration with Asian Sky Media — a branch of ASG focusing on media and publications. Asian Sky Media has a growing portfolio of business aviation reports designed to provide valuable information to readers for a better understanding of the market. Included in the portfolio is the Asia Pacific Fleet Reports for both civil helicopters and business jets, and the Africa Business Jet Fleet Report for a breakdown of fleet within respective countries. Asian Sky Quarterly provides a reader-friendly look at market dynamics within the pre-owned markets of civil helicopters and business jets. ASG’s latest reports include the Asia Pacific Business Jet Charter Report, Asia Pacific Training Report and the Asia Pacific Infrastructure Report focusing on respective industry segments showcasing the current status and challenges of the industry. DISCLAIMER The information contained in this report is provided free of charge for reference only. -

SMOKING AREA MAP Akihabara
Ginza Line Iidabashi Station Area Akihabara Station Area Suehirocho Sta. Ueno Public Smoking Area Private Smoking Area Iidabashi Oedo Line Both cigarette and Only heating type Government Offices Bldg. Iidabashi Sta. 2 00 00 heating type are possible 00 is possible Taito 3 Akihabara Tsukudo Elem. Sch. 4 Iidabashi Station Area Akihabara Station Area paspa Iidabashi West Exit Café Veloce Akihabara Station East Exit store Namboku Line/ 36 B-3 52 B-5 Kanda Fire Station Legal Affairs Bureau Onabuta Building 1F 1-7-7 Fujimi Ohgaku Building 1F 2-19 Kanda-Sakumacho Yurakucho Line 70 Taito Branch Office Iidabashi Sta. paspa Iidabashi East Exit Café Veloce Akihabara Station Ekimae-Square store B-5 37 Create Building 1F 1-8-10 Iidabashi B-3 53 Tsk building 1F 104 Kanda-Matsunagacho Agebacho 34 Shohei Elem. Sch. 22 Tabacco Sale Free Smoking Area Toshida Tully's Coffee Akihabara UDX store 29 38 B-3 80 B-5 80 1-7-8 Iidabashi Akihabara UDX 1 4-14-1 Soto-Kanda 69 Tokyo Kusei Kaikan 4 Iidabashi Sta. Soto-Kanda Doutor Coffee Shop Iidabashi Tokyo Kusei-Kaikan store Tully's Coffee Sumitomo Fudosan Akihabara First Building Terrace store 102 Tozai Line 34 B-3 81 B-4 Akihabara Tokyo Kusei Kaikan 3-5-1 Iidabashi Sumitomo Fudosan Akihabara First Building Terrace 1F 1-9-1 Soto-Kanda Kaguragashi Iidabashi Sta. 44 90 Chuo-dori Ave. 87 Sta. 12 Doutor Coffee Shop Iidabashi-Fujimi store 8 35 2-3-10 Fujimi B-2 Kanda- 53 Café de Crie Iidabashi East Exit store Kanda Station Area B-3 Aioicho 69 Rock Belay Building 1F 4-7-1 Iidabashi KISUKE SMOKING SPACE 81 C-4 13 Café de Crie Iidabashi Ramla store 16 3-3-9 Kanda-Kajicho B-2 37 11 70 Iidabashi Central Plaza Ramla 1F 4-25 Iidabashi 35 Iidabashi Kaneko Tobacco Shop Smoking Area 7 10 17 C-4 Akihabara Sta. -

Keio Presso Inn Otemachi
KEIO PRESSO INN OTEMACHI TEL Check-in 3:00 p.m. 03-3241-0202 We may cancel your reservation, if you do not arrive at the indicated FAX 03-3241-0203 arrival time without any notice. URL www.presso-inn.com/otemachi/ Check-out 10:00 a.m. 4-4-1 Honkokucho, Nihombashi, Chuo-ku, Number of Guest Rooms 386 Tokyo 103-0021 Number Room Type Room Size Capacity of Rooms Single 363Rooms 12m2 1Person Double 11Rooms 18m2 1-2 Persons Twin 11Rooms 18m2 1-2 Persons (Example pictured above) Universal- Complimentary Breakfast 1Room 24m2 1-2 Persons Designed Twin 6:30a.m. 9:30a.m. Kanda Sta. JR Yamanote Line Kamakurabashi South Mizuho Shin-nihombashi Tozai Line Ueno Exit Sta. Chugoku Bank Ginza Line Exit2 Mitsukoshi-mae Sta. JR Chuo Line/ Muromachi Sobu Line Kanda 3 chome COREDO Muromachi Edo Dori MINI STOP Mitsukoshimae Hanzomon Line Bank of Japan, Otemachi Sta. Chiyoda Line Otemachi Sta. Mitsukoshi Marunouchi Line Head Office Shin- Nihombashi River jobanbashi Marunouchi Line Otemachi Kayabacho Jobanbashi Hanzomon Line Ginza Line ExitB1 Tokyo Hanzomon Mitsukoshi-mae Sta. Toei Asakusa Line Nihombashi Line Shutoko Circular LineNihombashi Sta. Chiyoda Line Kasumigaseki ExitA5 COREDO Nihombashi ExitB6 Tozai Line Roppongi Tozai Line Otemachi Sta. Eitai Dori Nihombashi Sta. Otemachi Sta. Sta. Nihombashi Hibiya Ginza Line Hibiya Line Toei Mita Line Marunouchi Gofukubashi Ginza Nihombashi Sotobori Dori Toei Mita Line Oazo Exit Takashimaya Tokaido Shinkansen Marunouchi Line JR Keiyo Line Tokyo Sta. Yaesu North Showa Dori Shinagawa Hamamatsucho Exit Chuo Dori Monorail Tokyo Marunouchi North Exit Daimaru Marunouchi Tokyo Yaesu Dori Building Sta. -

Railway Operator : Chichibu Railway Co., Ltd. Accident Type : Level
Railway Accident Investigation Report, Synopsis Japan Transport Safety Board ~ Accident with human death caused by the collision between the train and a pedestrian, at the class 4 level crossing ~ Railway operator : Chichibu Railway Co., Ltd. Accident type : Level crossing accident Date and time : At about 16:52, December 19, 2018 Location : Hanyu No.22 level crossing, class 4 level crossing without automatic barrier machine nor road warning machine, in the premises of Shingo station of Chichibu Main Line, Hanyu City, Saitama Prefecture <SUMMARY> While the outbound 1545 train, started from Hanyu station bound for Kagemori station of Chichibu Main Line, was running in the premises of Shingo station at a velocity of about 43 km/h, the driver of the train noticed a pedestrian entering Hanyu No.22 level crossing, then sounded a whistle and applied an emergency brake immediately, but the train hit the pedestrian. The pedestrian was dead in the accident. Japan Transport Safety Board <PROBABLE CAUSES> - It is highly probable that the accident occurred as the train hit the pedestrian because the pedestrian entered Hanyu No.22 level crossing, class 4 level crossing without automatic barrier machine nor road warning device, in the situation that the train was approaching. - It could not be determined why the pedestrian entered the level crossing in the situation that the train was approaching, because the pedestrian was dead in the accident. <EXPECTED MEASURES TO PREVENT THE RECURRENCE> - The class 4 level crossing, that is not equipped with the automatic barrier machine nor the road warning device, should be abolished or should be equipped with the level crossing protection device.