The China Acute Myocardial Infarction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dressing for the Times: Fashion in Tang Dynasty China (618-907)
Dressing for the Times: Fashion in Tang Dynasty China (618-907) BuYun Chen Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2013 © 2013 BuYun Chen All rights reserved ABSTRACT Dressing for the Times: Fashion in Tang Dynasty China (618-907) BuYun Chen During the Tang dynasty, an increased capacity for change created a new value system predicated on the accumulation of wealth and the obsolescence of things that is best understood as fashion. Increased wealth among Tang elites was paralleled by a greater investment in clothes, which imbued clothes with new meaning. Intellectuals, who viewed heightened commercial activity and social mobility as symptomatic of an unstable society, found such profound changes in the vestimentary landscape unsettling. For them, a range of troubling developments, including crisis in the central government, deep suspicion of the newly empowered military and professional class, and anxiety about waste and obsolescence were all subsumed under the trope of fashionable dressing. The clamor of these intellectuals about the widespread desire to be “current” reveals the significant space fashion inhabited in the empire – a space that was repeatedly gendered female. This dissertation considers fashion as a system of social practices that is governed by material relations – a system that is also embroiled in the politics of the gendered self and the body. I demonstrate that this notion of fashion is the best way to understand the process through which competition for status and self-identification among elites gradually broke away from the imperial court and its system of official ranks. -

Resettlement Monitoring Report: People's Republic of China: Henan
Resettlement Monitoring Report Project Number: 34473 December 2010 PRC: Henan Wastewater Management and Water Supply Sector Project – Resettlement Monitoring Report No. 8 Prepared by: Environment School, Beijing Normal University For: Henan Province Project Management Office This report has been submitted to ADB by Henan Province Project Management Office and is made publicly available in accordance with ADB’s public communications policy (2005). It does not necessarily reflect the views of ADB. Henan Wastewater Management and Water Supply Sector Project Financed by Asian Development Bank Monitoring and Evaluation Report on the Resettlement of Henan Wastewater Management and Water Supply Sector Project (No. 8) Environment School Beijing Normal University, Beijing,China December , 2010 Persons in Charge : Liu Jingling Independent Monitoring and : Liu Jingling Evaluation Staff Report Writers : Liu Jingling Independent Monitoring and : Environment School, Beijing Normal University Evaluation Institute Environment School, Address : Beijing Normal University, Beijing, China Post Code : 100875 Telephone : 0086-10-58805092 Fax : 0086-10-58805092 E-mail : jingling @bnu .edu.cn Content CONTENT ...........................................................................................................................................................I 1 REVIEW .................................................................................................................................................... 1 1.1 PROJECT INTRODUCTION .................................................................................................................. -

World Bank Document
CONFORMED COPY LOAN NUMBER 7909-CN Public Disclosure Authorized Project Agreement Public Disclosure Authorized (Henan Ecological Livestock Project) between INTERNATIONAL BANK FOR RECONSTRUCTION AND DEVELOPMENT Public Disclosure Authorized and HENAN PROVINCE Dated July 26, 2010 Public Disclosure Authorized PROJECT AGREEMENT AGREEMENT dated July 26, 2010, entered into between INTERNATIONAL BANK FOR RECONSTRUCTION AND DEVELOPMENT (the “Bank”) and HENAN PROVINCE (“Henan” or the “Project Implementing Entity”) (“Project Agreement”) in connection with the Loan Agreement of same date between PEOPLE’S REPUBLIC OF CHINA (“Borrower”) and the Bank (“Loan Agreement”) for the Henan Ecological Livestock Project (the “Project”). The Bank and Henan hereby agree as follows: ARTICLE I – GENERAL CONDITIONS; DEFINITIONS 1.01. The General Conditions as defined in the Appendix to the Loan Agreement constitute an integral part of this Agreement. 1.02. Unless the context requires otherwise, the capitalized terms used in the Project Agreement have the meanings ascribed to them in the Loan Agreement or the General Conditions. ARTICLE II – PROJECT 2.01. Henan declares its commitment to the objective of the Project. To this end, Henan shall: (a) carry out the Project in accordance with the provisions of Article V of the General Conditions; and (b) provide promptly as needed, the funds, facilities, services and other resources required for the Project. 2.02. Without limitation upon the provisions of Section 2.01 of this Agreement, and except as the Bank and Henan shall otherwise agree, Henan shall carry out the Project in accordance with the provisions of the Schedule to this Agreement. ARTICLE III – REPRESENTATIVE; ADDRESSES 3.01. -

Westlake Youth Forum 2019 第四届西湖青年论坛
Westlake Youth Forum 2019 第四届西湖青年论坛 Call for Application Zhejiang University and China Medical Board (CMB) joint hands to host the 4th Westlake Youth Forum in 2019, with facilitation from China Health Policy and Management Society (CHPAMS). The Organizing Committee of the Forum is pleased to invite applications for participating in the Forum. The Forum provides a platform for young scholars worldwide to build up academic network, to exchange scientific thoughts and research experience, to communicate with senior scholars and policymakers, and to advance health policy in China. The 2019 Forum will be a three-day event for young researchers and practitioners in health policy and system on June 10-13, 2019 at Zhejiang University, China. Westlake Youth Forum: • When: June 10-13, 2019 • Where: Zhejiang University International Campus, Haining, Zhejiang Province, China • Preliminary Program: June 10. Registration and social activities June 11-12. Academic sessions and events of the Westlake Youth Forum June 13. Field visit What will be provided to all participants: • Local expenses including meals, accommodation, and local transportation in Haining, Zhejiang; • Networking with world-class academic leaders and young scholars from inside and outside of China; • Networking with Chinese academic leaders to explore your career opportunities in China; • Presenting your research and communicating with academic leaders and peers at the Forum. Who can apply for the participation (Eligibility)? • Scholars under 45 years old from CMB OC eligible schools (see Appendix I), OC awardees preferred but not required; • Working in public health related fields; • Having the interest to build collaboration with academic and research institutions, governmental departments, and corporations in China. -

Henan Wastewater Management and Water Supply Sector Project (11 Wastewater Management and Water Supply Subprojects)
Environmental Assessment Report Summary Environmental Impact Assessment Project Number: 34473-01 February 2006 PRC: Henan Wastewater Management and Water Supply Sector Project (11 Wastewater Management and Water Supply Subprojects) Prepared by Henan Provincial Government for the Asian Development Bank (ADB). The summary environmental impact assessment is a document of the borrower. The views expressed herein do not necessarily represent those of ADB’s Board of Directors, Management, or staff, and may be preliminary in nature. CURRENCY EQUIVALENTS (as of 02 February 2006) Currency Unit – yuan (CNY) CNY1.00 = $0.12 $1.00 = CNY8.06 The CNY exchange rate is determined by a floating exchange rate system. In this report a rate of $1.00 = CNY8.27 is used. ABBREVIATIONS ADB – Asian Development Bank BOD – biochemical oxygen demand COD – chemical oxygen demand CSC – construction supervision company DI – design institute EIA – environmental impact assessment EIRR – economic internal rate of return EMC – environmental management consultant EMP – environmental management plan EPB – environmental protection bureau GDP – gross domestic product HPG – Henan provincial government HPMO – Henan project management office HPEPB – Henan Provincial Environmental Protection Bureau HRB – Hai River Basin H2S – hydrogen sulfide IA – implementing agency LEPB – local environmental protection bureau N – nitrogen NH3 – ammonia O&G – oil and grease O&M – operation and maintenance P – phosphorus pH – factor of acidity PMO – project management office PM10 – particulate -

PPP Case Studies – People's Republic of China
1 PPP Case Studies People’s Republic of China Craig Sugden, Principal PPP Specialist East Asia Department 13 May 2015 The views expressed in this presentation are the views of the author and do not necessarily reflect the views or policies of the Asian Development Bank Institute (ADBI), the Asian Development Bank (ADB), its Board of Directors, or the governments they represent. ADBI does not guarantee the accuracy of the data included in this paper and accepts no responsibility for any consequences of their use. Terminology used may not necessarily be consistent with ADB official terms. 2 Background PPP Case Studies: the PRC PRC’s PPP projects 3 EIU’s 1,186 infrastructure PPPs finalised in the Infrascope PRC from 1990 to 2014 highlighted the PRC’s Compared to 838 in India, 126 in the Philippines, 108 in Indonesia, 73 in Sri Lanka, “phenomenal” 65 in Bangladesh wealth of project 648 active PPPs in the UK, 567 in the experience Republic of Korea, 127 in Australia (as of 2013) Source: World Bank. 2015. Private Participation in Infrastructure Projects Database and Burger P. and I. Hawkesworth. 2013. Capital Budgeting and Procurement Practices. Organization for Economic Cooperation and Development. Paris. PPP Case Studies: the PRC PPP activity in the PRC 4 Note: Excludes projects that are led by a majority-state owned enterprise Source: World Bank PIAF Database and IMF PPP Case Studies: the PRC Case studies 5 • Beijing Subway Line 4 The PRC has • Shanghai Huadian Xinzhuang Industrial Park combined cycle heat and power project • Baiyinchagan-Yongtaigong -

Job Burnout and Occupational Stressors Among Chinese Healthcare Professionals at County-Level Health Alliances Yan Liu, Li Lu, W
Job Burnout and Occupational Stressors among Chinese Healthcare Professionals at County-Level Health Alliances Yan Liu, Li Lu, W. X. Wang, S. Liu, H. R. Chen, X. Gao, M. Y. Huang, Y. M. Ren, C. C. Wang To cite this version: Yan Liu, Li Lu, W. X. Wang, S. Liu, H. R. Chen, et al.. Job Burnout and Occupational Stressors among Chinese Healthcare Professionals at County-Level Health Alliances. International Journal of Environmental Research and Public Health, MDPI, 2020, 17 (6), pp.1848. 10.3390/ijerph17061848. hal-03130467 HAL Id: hal-03130467 https://hal.archives-ouvertes.fr/hal-03130467 Submitted on 3 Feb 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution| 4.0 International License International Journal of Environmental Research and Public Health Article Job Burnout and Occupational Stressors among Chinese Healthcare Professionals at County-Level Health Alliances Yan Liu 1,2, Li Lu 3,* , Wen-Xin Wang 1, Shou Liu 1,2, Hong-Ru Chen 1,2, Xiang Gao 2, Ming-Yu Huang 2, Yong-Nian Liu 2, Yan-Ming Ren 2 and -
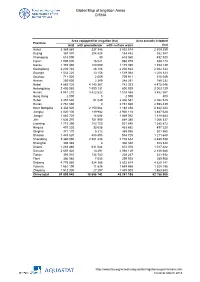
Global Map of Irrigation Areas CHINA
Global Map of Irrigation Areas CHINA Area equipped for irrigation (ha) Area actually irrigated Province total with groundwater with surface water (ha) Anhui 3 369 860 337 346 3 032 514 2 309 259 Beijing 367 870 204 428 163 442 352 387 Chongqing 618 090 30 618 060 432 520 Fujian 1 005 000 16 021 988 979 938 174 Gansu 1 355 480 180 090 1 175 390 1 153 139 Guangdong 2 230 740 28 106 2 202 634 2 042 344 Guangxi 1 532 220 13 156 1 519 064 1 208 323 Guizhou 711 920 2 009 709 911 515 049 Hainan 250 600 2 349 248 251 189 232 Hebei 4 885 720 4 143 367 742 353 4 475 046 Heilongjiang 2 400 060 1 599 131 800 929 2 003 129 Henan 4 941 210 3 422 622 1 518 588 3 862 567 Hong Kong 2 000 0 2 000 800 Hubei 2 457 630 51 049 2 406 581 2 082 525 Hunan 2 761 660 0 2 761 660 2 598 439 Inner Mongolia 3 332 520 2 150 064 1 182 456 2 842 223 Jiangsu 4 020 100 119 982 3 900 118 3 487 628 Jiangxi 1 883 720 14 688 1 869 032 1 818 684 Jilin 1 636 370 751 990 884 380 1 066 337 Liaoning 1 715 390 783 750 931 640 1 385 872 Ningxia 497 220 33 538 463 682 497 220 Qinghai 371 170 5 212 365 958 301 560 Shaanxi 1 443 620 488 895 954 725 1 211 648 Shandong 5 360 090 2 581 448 2 778 642 4 485 538 Shanghai 308 340 0 308 340 308 340 Shanxi 1 283 460 611 084 672 376 1 017 422 Sichuan 2 607 420 13 291 2 594 129 2 140 680 Tianjin 393 010 134 743 258 267 321 932 Tibet 306 980 7 055 299 925 289 908 Xinjiang 4 776 980 924 366 3 852 614 4 629 141 Yunnan 1 561 190 11 635 1 549 555 1 328 186 Zhejiang 1 512 300 27 297 1 485 003 1 463 653 China total 61 899 940 18 658 742 43 241 198 52 -
Deepbstn: a Deep Bidirection Network Model for Urban Traffic Prediction
2019 5th International Conference on Big Data Computing and Communications (BIGCOM 2019) Qingdao, China 9 – 11 August 2019 IEEE Catalog Number: CFP19N32-POD ISBN: 978-1-7281-4025-4 Copyright © 2019 by the Institute of Electrical and Electronics Engineers, Inc. All Rights Reserved Copyright and Reprint Permissions: Abstracting is permitted with credit to the source. Libraries are permitted to photocopy beyond the limit of U.S. copyright law for private use of patrons those articles in this volume that carry a code at the bottom of the first page, provided the per-copy fee indicated in the code is paid through Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923. For other copying, reprint or republication permission, write to IEEE Copyrights Manager, IEEE Service Center, 445 Hoes Lane, Piscataway, NJ 08854. All rights reserved. *** This is a print representation of what appears in the IEEE Digital Library. Some format issues inherent in the e-media version may also appear in this print version. IEEE Catalog Number: CFP19N32-POD ISBN (Print-On-Demand): 978-1-7281-4025-4 ISBN (Online): 978-1-7281-4024-7 Additional Copies of This Publication Are Available From: Curran Associates, Inc 57 Morehouse Lane Red Hook, NY 12571 USA Phone: (845) 758-0400 Fax: (845) 758-2633 E-mail: [email protected] Web: www.proceedings.com 2019 5th International Conference on Big Data Computing and Communications (BIGCOM) BIGCOM 2019 Table of Contents Welcome Message from the Chairs xi Conference Organization xii Session 1: Machine Learning and -

Congressional-Executive Commission on China Annual Report 2012
CONGRESSIONAL-EXECUTIVE COMMISSION ON CHINA ANNUAL REPORT 2012 ONE HUNDRED TWELFTH CONGRESS SECOND SESSION OCTOBER 10, 2012 Printed for the use of the Congressional-Executive Commission on China ( Available via the World Wide Web: http://www.cecc.gov 2012 ANNUAL REPORT CONGRESSIONAL-EXECUTIVE COMMISSION ON CHINA ANNUAL REPORT 2012 ONE HUNDRED TWELFTH CONGRESS SECOND SESSION OCTOBER 10, 2012 Printed for the use of the Congressional-Executive Commission on China ( Available via the World Wide Web: http://www.cecc.gov U.S. GOVERNMENT PRINTING OFFICE 76–190 PDF WASHINGTON : 2012 For sale by the Superintendent of Documents, U.S. Government Printing Office Internet: bookstore.gpo.gov Phone: toll free (866) 512–1800; DC area (202) 512–1800 Fax: (202) 512–2104 Mail: Stop IDCC, Washington, DC 20402–0001 CONGRESSIONAL-EXECUTIVE COMMISSION ON CHINA LEGISLATIVE BRANCH COMMISSIONERS House Senate CHRISTOPHER H. SMITH, New Jersey, SHERROD BROWN, Ohio, Cochairman Chairman MAX BAUCUS, Montana FRANK WOLF, Virginia CARL LEVIN, Michigan DONALD A. MANZULLO, Illinois DIANNE FEINSTEIN, California EDWARD R. ROYCE, California JEFF MERKLEY, Oregon TIMOTHY J. WALZ, Minnesota SUSAN COLLINS, Maine MARCY KAPTUR, Ohio JAMES RISCH, Idaho MICHAEL M. HONDA, California EXECUTIVE BRANCH COMMISSIONERS SETH D. HARRIS, Department of Labor MARIA OTERO, Department of State FRANCISCO J. SANCHEZ, Department of Commerce KURT M. CAMPBELL, Department of State NISHA DESAI BISWAL, U.S. Agency for International Development PAUL B. PROTIC, Staff Director LAWRENCE T. LIU, Deputy Staff -

Minimum Wage Standards in China August 11, 2020
Minimum Wage Standards in China August 11, 2020 Contents Heilongjiang ................................................................................................................................................. 3 Jilin ............................................................................................................................................................... 3 Liaoning ........................................................................................................................................................ 4 Inner Mongolia Autonomous Region ........................................................................................................... 7 Beijing......................................................................................................................................................... 10 Hebei ........................................................................................................................................................... 11 Henan .......................................................................................................................................................... 13 Shandong .................................................................................................................................................... 14 Shanxi ......................................................................................................................................................... 16 Shaanxi ...................................................................................................................................................... -

Building a Smoking Society: Culture and Ecology of the Tobacco
BUILDING A SMOKING SOCIETY: CULTURE AND ECOLOGY OF THE TOBACCO INDUSTRY IN NORTH CHINA, 1902-1937 By SIKANG SONG A dissertation submitted in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY WASHINGTON STATE UNIVERSITY Department of History MAY 2017 © Copyright by SIKANG SONG, 2017 All Rights Reserved © Copyright by SIKANG SONG, 2017 All Rights Reserved To the Faculty of Washington State University: The members of the Committee appointed to examine the dissertation of SIKANG SONG find it satisfactory and recommend that it be accepted. ______________________________________ David A. Pietz, Ph.D., Chair ___________________________________ Jeffrey C. Sanders, Ph.D., Co-Chair ___________________________________ Heather E. Streets-Salter, Ph.D. ___________________________________ Noriko Kawamura, Ph.D. ii ACKNOWLEDGMENTS I would like to express the deepest appreciation to my advisor Dr. David A. Pietz for his continuous support of my research and life, for his patience, motivation, enthusiasm, and invaluable knowledge. Without his guidance and persistent help, this dissertation would not have been possible. I also would like to express my immense gratitude to my committee members, Dr. Jeffery C. Sanders, Dr. Heather E. Streets-Salter, and Dr. Noriko Kawamura, whose expertise and dedication to Environmental History, World History, and East Asian Studies inspired me greatly. Their assistance and knowledge accompanied me on my graduate career at Washington State University. I am also very grateful for the WSU History Department and Graduate School providing me years of financial assistance for my study and living in Pullman. Especially, the Claudius O. and Mary W. Johnson Research Fellowship and the Conney Family Graduate Fellowship from the History Department supported my travels to China and allowed me to gather historical records and sources for my research in various locations there.