Introduction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Abstract Dermatophytes and Other Skin Mycoses Found in Featherless
Dermatophytes and other skin mycoses found in featherless broiler toe webs – Mbata Dermatophytes and other skin mycoses found in featherless broiler toe webs T.I. Mbata . (1) Department of Microbiology, Federal Polytechnic, Nekede, Owerri, Nigeria . Author of Correspondence: T.I.Mbata, Department of Microbiology, Federal Polytechnic, Nekede, Owerri, Nigeria, E-mail: [email protected]. +2348032618922 Abstract Background: Feartherless broilers which are produced by a complex breeding programme from feathered parents carrying the Sc-gene, dissipates excessive body heat under hot and humid conditions. It has high body weight, and grows very rapidly when compared with standard commercial broilers. Their toe webs are bigger than standard commercial broilers, and could harbor fungi which can cause infections where there is the opportunity. Objectives: To isolate and identify the presence of fungi in toe webs of featherless broilers. Methods: A total of 50 featherless broilers' toe webs samples were examined microscopically for the presence of fungi. The samples were examined microscopically and culturally using standard microbiological techniques. Results: The fungi recovered were as follows. Microsporum gypseum 9 (22%), Trichophyton mentagrophytes var. mentagrophytes 5 (12%), Microsporum gallinae 3 (7%), Aspergilus flavus 10 (24%), Fusarium sp 6 (15%), Alternaria alternata 3 (7%) Scopulariopsis brevicaulis 2 (5%) and Candida albicans 3 (7%), Conclusion: The featherless broilers' toe webs habour fungi which cause mycotic skin disease and cannot be regarded as ordinary normal flora of toe webs Key words: Dermatophytes, Non- dermatophytes, featherless broiler, toe webs. INTRODUCTION Animals serve as reservoirs of the zoophilic dermatophytes, and their infections have Dermatophytes are among the most frequent considerable zoonotic importance. -

The New Species Concept in Dermatophytes—A Polyphasic Approach
Mycopathologia DOI 10.1007/s11046-008-9099-y The New Species Concept in Dermatophytes—a Polyphasic Approach Yvonne Gra¨ser Æ James Scott Æ Richard Summerbell Received: 15 October 2007 / Accepted: 30 January 2008 Ó Springer Science+Business Media B.V. 2008 Abstract The dermatophytes are among the most among these are the cosmopolitan bane of nails and frequently observed organisms in biomedicine, yet feet, Trichophyton rubrum, and the endemic African there has never been stability in the taxonomy, agent of childhood tinea capitis, Trichophyton identification and naming of the approximately 25 soudanense, which are effectively inseparable in all pathogenic species involved. Since the identification analyses. The molecular data require some reinter- of these species is often epidemiologically and pretation of results seen in conventional phenotypic ethically important, the difficulties in dermatophyte tests, but in most cases, phylogenetic insight is identification are a fruitful topic for modern molec- readily integrated with current laboratory testing ular biological investigation, done in tandem with procedures. renewed investigation of phenotypic characters. Molecular phylogenetic analyses such as multilocus Keywords Dermatophytes Á Taxonomy Á sequence typing have had to be tailored to accom- Molecular identification Á modate differing the mechanisms of speciation that Morphological identification Á Species concept have produced the dermatophytes that are commonly seen today. Even so, some biotypes that were unambiguously considered species in the past, based Introduction: Why Dermatophyte Biosystematics on profound differences in morphology and pattern of and Identification are Important (Medical infection, appear consistently not to be distinct and Scientific Aspects) species in modern molecular analyses. Most notable The dermatophytes belong to the small category of disease organisms that almost every human alive will Y. -

Dermatophytosis in Small Animals Antonella S
www.symbiosisonline.org Symbiosis www.symbiosisonlinepublishing.com Review Article SOJ Microbiology & Infectious Diseases Open Access Dermatophytosis in Small Animals Antonella S. Mattei1*, Márcia A. Beber2 and Isabel M. Madrid3 1University Federal of Rio Grande (FURG), Medical School, RS, Brazil 2Undergraduate Student in Dentistry, Federal University of Pelotas (UFPel), Pelotas, RS, Brazil 3Facuty of Veterinary, Zoonosis Center Control, Federal University of Pelotas (UFPel), Pelotas, RS, Brazil Received: March 06, 2014; Accepted: September 19, 2014; Published: November 04, 2014 *Corresponding author: Antonella Souza Mattei, University Federal of Rio Grande (FURG), Medical School, RS, Brazil, Tel: +55(53)-91447884; E-mail: an- [email protected] Originally soil inhabitants, dermatophytes have evolved to Abstract geophilic, zoophilic, and anthropophilic species based on their dermatophytosis in small animals. In the last years, the pet population maininfect habitatanimals or and host. humans Three dermatophytes and are accordingly genera classified Trichophyton into, has increasedThe purpose as well of the this interest article in havingwas animalsto briefly as pets.review Because about of Microsporum, and Epidermophyton-comprise more than 40 this, these small animals are more and more inserted in our daily life. different species [4,5]. The understanding of ringworm epidemiology, diagnosis, treatment and control in pets is very important for the reason that pets are often Animals can be infected by a great variety of dermatophytes, asymptomatic carriers of dermatophytes being important sources of mostly zoophilic but also geophilic species, and exceptionally infection and/or carriers of infection. So, it is very important to know about this disease to reduce the spread of zoophilic fungal infections anthropophilic dermatophytes (Table 1) [6]. -
Dr. Poonam Shakya Fungi That Require and Use Keratin for Growth Confined to the Superficial Integument of the Skin, Nails, Claws & Hair of Animals and Man
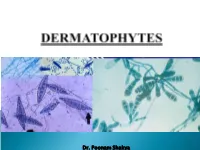
Dr. Poonam Shakya Fungi that require and use keratin for growth Confined to the superficial integument of the skin, nails, claws & hair of animals and man Classical lesions- circular ( ringworm) Traditionally the dermatophytes are placed in the Deuteromycota or Fungi Imperfecti in 3 genera: Microsporum, Trichophyton Epidermophyton The Microsporum species tend to produce spindle shaped macroconidia Microsporum canis: spindle-shaped macroconidia. (LPCB, ×400) Microsporum gypseum: boat shaped macroconidia. (LPCB) Trichophyton mentagrophytes: cigar shaped numerous microconidia and a macroconidium. Microsporum nanum: round & two celled macroconidia. (LPCB) The geophilic (soil-loving) dermatophytes inhabit the soil and can exist there as free-living saprophytes. Example- Microsporum gypseum and M. nanum The zoophilic dermatophytes are obligate pathogens, primarily parasitizing animals but also capable of infecting humans. Humans are the main host for the anthropophilic dermatophytes and these very rarely cause ringworm in animals Some dermatophytes have become adapted for survival in the skin of specific host animals, for example: Microsporum canis: cats Microsporum persicolor: voles Trichophyton mentagrophytes var. mentagrophytes: rodents Trichophyton verrucosum: cattle. Trichophyton erinacei: muzzle alopecia in a terrier known to worry hedgehogs. Infective arthrospores germinate within 6 hours of adhering to keratinized structures. Minor trauma of the skin and dampness may facilitate infection. The ability of the dermatophytes -

Dermatophyte and Non Dermatophyte Fungi in Riyadh City, Saudi Arabia
Saudi Journal of Biological Sciences (2015) xxx, xxx–xxx King Saud University Saudi Journal of Biological Sciences www.ksu.edu.sa www.sciencedirect.com ORIGINAL ARTICLE Dermatophyte and non dermatophyte fungi in Riyadh City, Saudi Arabia Jamal M. Khaled a,b,*, Hammed A Golah c, Abdulla S. Khalel a, Naiyf S. Alharbi a, Ramzi A. Mothana d a Department of Botany and Microbiology, College of Science, King Saud University, Riyadh, Saudi Arabia b Department of Biotechnology and Food Technology, Thamar University, Yemen c Agriculture and Veterinary Medicine, Department of Veterinary Medicine, Thamar University, Yemen d Department of Pharmacognosy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia Received 2 September 2014; revised 24 November 2014; accepted 15 December 2014 KEYWORDS Abstract Background: Dermatophytes are a scientific label for a group of three genera (Micros- Dermatophytes; porum, Epidermophyton and Trichophyton) of fungus that causes skin disease in animals and Microsporum; humans. Conventional methods for identification of these fungi are rapid and simple but are not Epidermophyton; accurate comparing to molecular methods. Trichophyton; Objective: This study aimed to isolate human pathogenic dermatophytes which cause dermato- Tinea phytosis in Riyadh City, Saudi Arabia and to identify these fungi by using conventional and molec- ular methods. Methods: The study was conducted in Medical Complex, Riyadh and King Saud University. Samples of infected skin, hairs and nails were collected from 112 patients. Diagnosis of skin infec- tions, direct microscopic test, isolation and identification of dermatophytes by conventional and molecular methods were carried out. Results: The results indicated that the tinea capitis infection had the highest prevalence among the patients (22.3%) while Tinea barbae had the lowest. -

Descriptions of Medical Fungi
DESCRIPTIONS OF MEDICAL FUNGI THIRD EDITION (revised November 2016) SARAH KIDD1,3, CATRIONA HALLIDAY2, HELEN ALEXIOU1 and DAVID ELLIS1,3 1NaTIONal MycOlOgy REfERENcE cENTRE Sa PaTHOlOgy, aDElaIDE, SOUTH aUSTRalIa 2clINIcal MycOlOgy REfERENcE labORatory cENTRE fOR INfEcTIOUS DISEaSES aND MIcRObIOlOgy labORatory SERvIcES, PaTHOlOgy WEST, IcPMR, WESTMEaD HOSPITal, WESTMEaD, NEW SOUTH WalES 3 DEPaRTMENT Of MOlEcUlaR & cEllUlaR bIOlOgy ScHOOl Of bIOlOgIcal ScIENcES UNIvERSITy Of aDElaIDE, aDElaIDE aUSTRalIa 2016 We thank Pfizera ustralia for an unrestricted educational grant to the australian and New Zealand Mycology Interest group to cover the cost of the printing. Published by the authors contact: Dr. Sarah E. Kidd Head, National Mycology Reference centre Microbiology & Infectious Diseases Sa Pathology frome Rd, adelaide, Sa 5000 Email: [email protected] Phone: (08) 8222 3571 fax: (08) 8222 3543 www.mycology.adelaide.edu.au © copyright 2016 The National Library of Australia Cataloguing-in-Publication entry: creator: Kidd, Sarah, author. Title: Descriptions of medical fungi / Sarah Kidd, catriona Halliday, Helen alexiou, David Ellis. Edition: Third edition. ISbN: 9780646951294 (paperback). Notes: Includes bibliographical references and index. Subjects: fungi--Indexes. Mycology--Indexes. Other creators/contributors: Halliday, catriona l., author. Alexiou, Helen, author. Ellis, David (David H.), author. Dewey Number: 579.5 Printed in adelaide by Newstyle Printing 41 Manchester Street Mile End, South australia 5031 front cover: Cryptococcus neoformans, and montages including Syncephalastrum, Scedosporium, Aspergillus, Rhizopus, Microsporum, Purpureocillium, Paecilomyces and Trichophyton. back cover: the colours of Trichophyton spp. Descriptions of Medical Fungi iii PREFACE The first edition of this book entitled Descriptions of Medical QaP fungi was published in 1992 by David Ellis, Steve Davis, Helen alexiou, Tania Pfeiffer and Zabeta Manatakis. -

Monograph on Dermatophytes
Monograph On Dermatophytes A guide for isolation and identification of dermatophytes, diseases and treatment By Mohamed Refai, Heidy Abo El-Yazid and Mahmoud El-Hariri Department of Microbiology, Faculty of Veterinary Medicine, Cairo University 2013 1 Dedication This monograph is dedicated to my master, friend, teacher and spiritual father Prof. Dr. Dr. Hans Rieth, whom I met for the first time in July 1962, in Travemunde on the occasion of the second meeting of the German-speaking Mycological society, 6 months after my arrival to Germany, and whom I met for the last time in September, 1993 in Greifswald on the occasion of 27th meeting of the society, 5 months before his death. During the 30 years I visited him almost every year, where I always updated my knowledge in mycology Mohamed Refai Late Prof. Dr. Dr. Hans Rieth, 11.12.1914-10.2.1994 1962, in Travemunde Greifswald, 30.9. 1993 2 Contents 1. Introduction and historical 2. classification of dermatophytes 3. Morphology of dermatophytes 4. Gallery of the commonly isolated dermatophytes 5. Diseases caused by dermatophytes 5.1. Diseases caused by dermatophytes in man 5.2. Diseases caused by dermatophytes in animals 6. Diagnosis of diseases caused by dermatophytes 6.5. Phenotypic identification of dermatophytes 6.6. Molecular identification of dermatophytes 7. Treatment of diseases caused by dermatophytes 7.1. Treatment of diseases caused by dermatophytes in man 7.2. Treatment of diseases caused by dermatophytes in animals 8. Prevention and control of diseases caused by dermatophytes 8.1. Hygienic measures 8.2. Vaccination 9. Materials used for identification of dermatophytes 10. -

Favus in a Backyard Chicken (Gallus Gallus Domesticus)
FAVUS IN A BACKYARD CHICKEN (GALLUS GALLUS DOMESTICUS) Hamish R Baron1, Bob Doneley2 1 School of Veterinary Science University of Sydney Camden, NSW 2570, Australia 2Senior Lecturer in Avian and Exotic Pet Medicine School of Veterinary Science University of Queensland, Gatton 4343 Introduction Favus, or avian ringworm, is a dermatophytosis that is rarely reported in poultry today. (Saif and Fadly 2008) However, given the strong influx in backyard poultry being presented to avian and exotic veterinarians in recent years, it is an important diagnosis which should not be overlooked. The classical clinical presentation includes white crusting lesions on unfeathered skin which can extend to the feathered portion of the skin and form scutula around the base of feather follicles, leading to feather loss. The most commonly isolated organism is Microsporum gallinae, however M. gypseum and Trichophyton simii have also been isolated as causative agents. (Fonseca and Mendoza 1984, Droual, Bickford et al. 1991, Bradley, Bickford et al. 1993) The present report describes a particularly striking and intensely pruritic case of generalised feather loss with hyperkeratosis in a backyard laying hen. Case report A 16 month old black Orpington (Gallus gallus domesticus) hen presented to the University of Queensland Veterinary Medical Centre, Gatton for intense pruritis and feather loss progressively worsening over one month. The hen was obtained as a layer pullet in July 2013 and was kept in a coop with nine other chickens which were clinically healthy. The chickens were fed a commercial layer diet and were given free range of the owner’s yard during the day. Two months prior to presentation the chicken was treated at a local veterinary clinic after the owners noticed discharge from the nares and bubbles from the conjunctival sac. -

Características Morfológicas De 45 Cepas De Microsporum Canis Revista Mexicana De Micología, Vol
Revista Mexicana de Micología ISSN: 0187-3180 [email protected] Sociedad Mexicana de Micología México Moreno-Coutiño, Gabriela; Palomares, María de la Paz; Fernández-Martínez, Ramón; Arenas, Roberto Características morfológicas de 45 cepas de Microsporum canis Revista Mexicana de Micología, vol. 29, junio, 2009, pp. 31-35 Sociedad Mexicana de Micología Xalapa, México Disponible en: http://www.redalyc.org/articulo.oa?id=88316057005 Cómo citar el artículo Número completo Sistema de Información Científica Más información del artículo Red de Revistas Científicas de América Latina, el Caribe, España y Portugal Página de la revista en redalyc.org Proyecto académico sin fines de lucro, desarrollado bajo la iniciativa de acceso abierto Características morfológicas de 45 cepas de Microsporum canis Gabriela Moreno-Coutiño1, María de la Paz Palomares2 Ramón Fernández-Martínez 1, Roberto Arenas1 1 Sección de Micología, Hospital General Dr. Manuel Gea González, SSA. 2Clínica de Especialidades No. 4 de la Secretaría de Salud de la Ciudad de México 9 0 0 Morphologic characteristics of 45 Microsporum canis strains 2 , 5 3 - Abstract. Dermatophytes are pathogen fungi of skin and its appendages. One of them, 1 3 Microsporum spp. has micro and macroscopic characteristics mainly based on the shape and : 9 2 size of macroconidia and echinulations that allow the identification of the species. The macro A Í and micromorphological characteristics of 45 M. canis strains were analized with the G O intention of classifying them into subspecies. All samples had a previous positive direct exam L O C with KOH and were cultured in both Sabouraud dextrose agar with antibiotic and rice media. -

Características Morfológicas De 45 Cepas De Microsporum Canis O R IG IN
Características morfológicas de 45 cepas de Microsporum canis Gabriela Moreno-Coutiño1, María de la Paz Palomares2 Ramón Fernández-Martínez 1, Roberto Arenas1 1 Sección de Micología, Hospital General Dr. Manuel Gea González, SSA. 2Clínica de Especialidades No. 4 de la Secretaría de Salud de la Ciudad de México 9 0 0 Morphologic characteristics of 45 Microsporum canis strains 2 , 5 3 - Abstract. Dermatophytes are pathogen fungi of skin and its appendages. One of them, 1 3 Microsporum spp. has micro and macroscopic characteristics mainly based on the shape and : 9 2 size of macroconidia and echinulations that allow the identification of the species. The macro A Í and micromorphological characteristics of 45 M. canis strains were analized with the G O intention of classifying them into subspecies. All samples had a previous positive direct exam L O C with KOH and were cultured in both Sabouraud dextrose agar with antibiotic and rice media. I M Thirty five percent grew by the second week. A white velvety colony with a yellowish color on E D the reversal side was the usual phenotype. Fifteen percent of cultures on rice media were A negative. The typical M. canis morphology was seen in 81.1% and macroconidia had an N A C average of 9.08 septa. Sixteen cases had a mixed morphology. Microsporum canis strains are I X easily identified in most cases, however, in atypical specimens, M. audouinii should be ruled E M out. A T S Key words: dermatophytes, Microsporum audouinii. I V E R Resumen. Los dermatofitos son hongos que parasitan la piel y sus anexos. -

103 Wang.Pdf
564 ISAH-2007 Tartu, Estonia BIODIVERSITY AND CONCENTRATION OF AIRBORNE FUNGI IN CHICKEN HOUSE Wang, Y.1 , Lu, G.1, Zhang, X.2, Ma, R.3 and Chai, T.2* 1 College of life Science, Dalian Nationalities University, Dalian 116600, China; 2 College of Animal Science and Veterinary Medicine, Shandong Agricultural University, Tai’an 271018,China; 3 Hospital of Shandong Agricultural University, Tai’an 271018, China; *Corresponding author: Tongjie Chai, Professor. Dr., Director of the Institute for Microbiology; Email:[email protected] ABSTRACT The biodiversity and concentration of airborne fungi in chicken house were investigated. The air samples were collected by means of 6-stage Andersen sampler and common fungal counting media. 78 fungal species were identified from air samplings after mycological examination. they are mainly mitosporic fungi. Cladosporium, Penicillium, Aspergillus, Candida, Alternaria and Fusarium were the predominant fungal genera, including ten species of avian pathogenic fungi, such as A. flavus, A. fumigatus, A. niger and F. sporotrichioides et al. The average concentration of airborne fungi in the chicken house was 2.3×103 CFU/m3. The concentrations of A. flavus, A. fumigatus and A. niger were relatively higher in the air of chicken house. The distribution of airborne fungi in the chicken house shows normal logarithm, the spores of Cladosporium, Penicillium and Aspergillus were mainly distributed within C and D stages (3.0–6.0µm), while stage A and B (>6.0µm) as well as E and F stage (<3.0µm) relatively less. On the other hand, C. albicans, Histoplasma capsulatum, Cryptococcus neoformans and Coccidioides immitis, which occur uncommonly but pose potential threat to public health. -

Toward a Novel Multilocus Phylogenetic Taxonomy for the Dermatophytes
Mycopathologia DOI 10.1007/s11046-016-0073-9 Toward a Novel Multilocus Phylogenetic Taxonomy for the Dermatophytes G. Sybren de Hoog . Karolina Dukik . Michel Monod . Ann Packeu . Dirk Stubbe . Marijke Hendrickx . Christiane Kupsch . J. Benjamin Stielow . Joanna Freeke . Markus Go¨ker . Ali Rezaei-Matehkolaei . Hossein Mirhendi . Yvonne Gra¨ser Received: 1 July 2016 / Accepted: 28 September 2016 Ó The Author(s) 2016. This article is published with open access at Springerlink.com Abstract Type and reference strains of members of anthropophilic dermatophytes in Trichophyton and the onygenalean family Arthrodermataceae have been Epidermophyton, along with some zoophilic species sequenced for rDNA ITS and partial LSU, the riboso- that regularly infect humans. Microsporum is restricted mal 60S protein, and fragments of b-tubulin and to some species around M. canis, while the geophilic translation elongation factor 3. The resulting phyloge- species and zoophilic species that are more remote netic trees showed a large degree of correspondence, from the human sphere are divided over Arthroderma, and topologies matched those of earlier published Lophophyton and Nannizzia. A new genus Guar- phylogenies demonstrating that the phylogenetic rep- romyces is proposed for Keratinomyces ceretanicus. resentation of dermatophytes and dermatophyte-like Thirteen new combinations are proposed; in an over- fungi has reached an acceptable level of stability. All view of all described species it is noted that the largest trees showed Trichophyton to be polyphyletic. In the number of novelties was introduced during the decades present paper, Trichophyton is restricted to mainly the 1920–1940, when morphological characters were used derived clade, resulting in classification of nearly all in addition to clinical features.