Quickstudy.Com
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List: Bones & Bone Markings of Appendicular Skeleton and Knee
List: Bones & Bone markings of Appendicular skeleton and Knee joint Lab: Handout 4 Superior Appendicular Skeleton I. Clavicle (Left or Right?) A. Acromial End B. Conoid Tubercle C. Shaft D. Sternal End II. Scapula (Left or Right?) A. Superior border (superior margin) B. Medial border (vertebral margin) C. Lateral border (axillary margin) D. Scapular notch (suprascapular notch) E. Acromion Process F. Coracoid Process G. Glenoid Fossa (cavity) H. Infraglenoid tubercle I. Subscapular fossa J. Superior & Inferior Angle K. Scapular Spine L. Supraspinous Fossa M. Infraspinous Fossa III. Humerus (Left or Right?) A. Head of Humerus B. Anatomical Neck C. Surgical Neck D. Greater Tubercle E. Lesser Tubercle F. Intertubercular fossa (bicipital groove) G. Deltoid Tuberosity H. Radial Groove (groove for radial nerve) I. Lateral Epicondyle J. Medial Epicondyle K. Radial Fossa L. Coronoid Fossa M. Capitulum N. Trochlea O. Olecranon Fossa IV. Radius (Left or Right?) A. Head of Radius B. Neck C. Radial Tuberosity D. Styloid Process of radius E. Ulnar Notch of radius V. Ulna (Left or Right?) A. Olecranon Process B. Coronoid Process of ulna C. Trochlear Notch of ulna Human Anatomy List: Bones & Bone markings of Appendicular skeleton and Knee joint Lab: Handout 4 D. Radial Notch of ulna E. Head of Ulna F. Styloid Process VI. Carpals (8) A. Proximal row (4): Scaphoid, Lunate, Triquetrum, Pisiform B. Distal row (4): Trapezium, Trapezoid, Capitate, Hamate VII. Metacarpals: Numbered 1-5 A. Base B. Shaft C. Head VIII. Phalanges A. Proximal Phalanx B. Middle Phalanx C. Distal Phalanx ============================================================================= Inferior Appendicular Skeleton IX. Os Coxae (Innominate bone) (Left or Right?) A. -

Elbow Checklist
Workbook Musculoskeletal Ultrasound September 26, 2013 Shoulder Checklist Long biceps tendon Patient position: Facing the examiner Shoulder in slight medial rotation; elbow in flexion and supination Plane/ region: Transverse (axial): from a) intraarticular portion to b) myotendinous junction (at level of the pectoralis major tendon). What you will see: Long head of the biceps tendon Supraspinatus tendon Transverse humeral ligament Subscapularis tendon Lesser tuberosity Greater tuberosity Short head of the biceps Long head of the biceps (musculotendinous junction) Humeral shaft Pectoralis major tendon Plane/ region: Logitudinal (sagittal): What you will see: Long head of biceps; fibrillar structure Lesser tuberosity Long head of the biceps tendon Notes: Subscapularis muscle and tendon Patient position: Facing the examiner Shoulder in lateral rotation; elbow in flexion/ supination Plane/ region: longitudinal (axial): full vertical width of tendon. What you will see: Subscapularis muscle, tendon, and insertion Supraspinatus tendon Coracoid process Deltoid Greater tuberosity Lesser tuberosity Notes: Do passive medial/ lateral rotation while examining Plane/ region: Transverse (sagittal): What you will see: Lesser tuberosity Fascicles of subscapularis tendon Supraspinatus tendon Patient position: Lateral to examiner Shoulder in extension and medial rotation Hand on ipsilateral buttock Plane/ region: Longitudinal (oblique sagittal) Identify the intra-articular portion of biceps LH in the transverse plane; then -

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Structure of the Human Body
STRUCTURE OF THE HUMAN BODY Vertebral Levels 2011 - 2012 Landmarks and internal structures found at various vertebral levels. Vertebral Landmark Internal Significance Level • Bifurcation of common carotid artery. C3 Hyoid bone Superior border of thyroid C4 cartilage • Larynx ends; trachea begins • Pharynx ends; esophagus begins • Inferior thyroid A crosses posterior to carotid sheath. • Middle cervical sympathetic ganglion C6 Cricoid cartilage behind inf. thyroid a. • Inferior laryngeal nerve enters the larynx. • Vertebral a. enters the transverse. Foramen of C 6. • Thoracic duct reaches its greatest height C7 Vertebra prominens • Isthmus of thyroid gland Sternoclavicular joint (it is a • Highest point of apex of lung. T1 finger's breadth below the bismuth of the thyroid gland T1-2 Superior angle of the scapula T2 Jugular notch T3 Base of spine of scapula • Division between superior and inferior mediastinum • Ascending aorta ends T4 Sternal angle (of Louis) • Arch of aorta begins & ends. • Trachea ends; primary bronchi begin • Heart T5-9 Body of sternum T7 Inferior angle of scapula • Inferior vena cava passes through T8 diaphragm T9 Xiphisternal junction • Costal slips of diaphragm T9-L3 Costal margin • Esophagus through diaphragm T10 • Aorta through diaphragm • Thoracic duct through diaphragm T12 • Azygos V. through diaphragm • Pyloris of stomach immediately above and to the right of the midline. • Duodenojejunal flexure to the left of midline and immediately below it Tran pyloric plane: Found at the • Pancreas on a line with it L1 midpoint between the jugular • Origin of Superior Mesenteric artery notch and the pubic symphysis • Hilum of kidneys: left is above and right is below. • Celiac a. -
Scapular Dyskinesis
Scapular Dyskinesis Presented by: Scott Sevinsky MSPT Presented by: Scott Sevinsky SPT 1 What is Scapular Dyskinesis? Alteration in the normal static or dynamic position or motion of the scapula during coupled scapulohumeral movements. Other names given to this catch-all phrase include: “floating scapula” and “lateral scapular slide”.1, 2 1 Alterations in scapular position and motion occur in 68 – 100% of patients with shoulder injuries. Scapular Dyskinesis Classification System 1, 3 Pattern Definitions Inferior angle At rest, the inferior medial scapular border may be prominent dorsally. During arm motion, the inferior (type I) angle tilts dorsally and the acromion tilts ventrally over the top of the thorax. The axis of the rotation is in the horizontal plane. Medial border At rest, the entire medial border may be prominent dorsally. During arm motion, the medial scapular (type II) border tilts dorsally off the thorax. The axis of the rotation is vertical in the frontal plane. Superior border At rest, the superior border of the scapula may be elevated and the scapula can also be anteriorly (type III) displaced. During arm motion, a shoulder shrug initiates movement without significant winging of the scapula occurring. The axis of this motion occurs in the sagittal plane. Symmetric At rest, the position of both scapula are relatively symmetrical, taking into account that the dominant scapulohumeral arm may be slightly lower. During arm motion, the scapulae rotate symmetrically upward such that the (type IV) inferior angles translate laterally away from the midline and the scapular medial border remains flush against the thoracic wall. The reverse occurs during lowering of the arm. -

The Appendicular Skeleton Appendicular Skeleton
THE SKELETAL SYSTEM: THE APPENDICULAR SKELETON APPENDICULAR SKELETON The primary function is movement It includes bones of the upper and lower limbs Girdles attach the limbs to the axial skeleton SKELETON OF THE UPPER LIMB Each upper limb has 32 bones Two separate regions 1. The pectoral (shoulder) girdle (2 bones) 2. The free part (30 bones) THE PECTORAL (OR SHOULDER) GIRDLE UPPER LIMB The pectoral girdle consists of two bones, the scapula and the clavicle The free part has 30 bones 1 humerus (arm) 1 ulna (forearm) 1 radius (forearm) 8 carpals (wrist) 19 metacarpal and phalanges (hand) PECTORAL GIRDLE - CLAVICLE The clavicle is “S” shaped The medial end articulates with the manubrium of the sternum forming the sternoclavicular joint The lateral end articulates with the acromion forming the acromioclavicular joint THE CLAVICLE PECTORAL GIRDLE - CLAVICLE The clavicle is convex in shape anteriorly near the sternal junction The clavicle is concave anteriorly on its lateral edge near the acromion CLINICAL CONNECTION - FRACTURED CLAVICLE A fall on an outstretched arm (F.O.O.S.H.) injury can lead to a fractured clavicle The clavicle is weakest at the junction of the two curves Forces are generated through the upper limb to the trunk during a fall Therefore, most breaks occur approximately in the middle of the clavicle PECTORAL GIRDLE - SCAPULA Also called the shoulder blade Triangular in shape Most notable features include the spine, acromion, coracoid process and the glenoid cavity FEATURES ON THE SCAPULA Spine - -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -
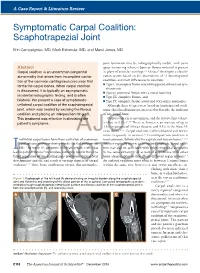
Symptomatic Carpal Coalition: Scaphotrapezial Joint
A Case Report & Literature Review E. Campaigniac et al Symptomatic Carpal Coalition: Scaphotrapezial Joint Erin Campaigniac, MD, Mark Eskander, MD, and Marci Jones, MD joint formation may be radiographically visible, with joint Abstract space narrowing wherein bone or fibrous material is present Carpal coalition is an uncommon congenital in place of articular cartilage.2,4 Minaar8 developed a classifi- abnormality that arises from incomplete cavita- cation system based on his observations of 12 lunotriquetral tion of the common cartilaginous precursor that coalitions and their differences in coalition: ◾ Type I, incomplete fusion resembling pseudarthrosis or syn- forms the carpal bones. When carpal coalition chondrosis is discovered, it is typically an asymptomatic ◾ Type II, proximal fusion with a distal notching incidental radiographic finding, and is often ◾ Type III, complete fusion, and bilateral. We present a case of symptomatic ◾ Type IV, complete fusion associated with other anomalies. unilateral carpal coalition of the scaphotrapezial Although these 4 types were based on lunotriquetral coali- joint, which was treated by excising the fibrous tions, this classification system is used to describe the coalition coalition and placing an interposition fat graft. of any carpal bone. This treatment was effective in alleviating the Carpal coalition is uncommon, and the reported prevalence 2,5,6,9 patient’s symptoms. is close to 0.1%. There is, however, an increase of up to 1.5% in patients of African descent, and 9.5% in the West Af- rican -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Parts of the Body 1) Head – Caput, Capitus 2) Skull- Cranium Cephalic- Toward the Skull Caudal- Toward the Tail Rostral- Toward the Nose 3) Collum (Pl
BIO 3330 Advanced Human Cadaver Anatomy Instructor: Dr. Jeff Simpson Department of Biology Metropolitan State College of Denver 1 PARTS OF THE BODY 1) HEAD – CAPUT, CAPITUS 2) SKULL- CRANIUM CEPHALIC- TOWARD THE SKULL CAUDAL- TOWARD THE TAIL ROSTRAL- TOWARD THE NOSE 3) COLLUM (PL. COLLI), CERVIX 4) TRUNK- THORAX, CHEST 5) ABDOMEN- AREA BETWEEN THE DIAPHRAGM AND THE HIP BONES 6) PELVIS- AREA BETWEEN OS COXAS EXTREMITIES -UPPER 1) SHOULDER GIRDLE - SCAPULA, CLAVICLE 2) BRACHIUM - ARM 3) ANTEBRACHIUM -FOREARM 4) CUBITAL FOSSA 6) METACARPALS 7) PHALANGES 2 Lower Extremities Pelvis Os Coxae (2) Inominant Bones Sacrum Coccyx Terms of Position and Direction Anatomical Position Body Erect, head, eyes and toes facing forward. Limbs at side, palms facing forward Anterior-ventral Posterior-dorsal Superficial Deep Internal/external Vertical & horizontal- refer to the body in the standing position Lateral/ medial Superior/inferior Ipsilateral Contralateral Planes of the Body Median-cuts the body into left and right halves Sagittal- parallel to median Frontal (Coronal)- divides the body into front and back halves 3 Horizontal(transverse)- cuts the body into upper and lower portions Positions of the Body Proximal Distal Limbs Radial Ulnar Tibial Fibular Foot Dorsum Plantar Hallicus HAND Dorsum- back of hand Palmar (volar)- palm side Pollicus Index finger Middle finger Ring finger Pinky finger TERMS OF MOVEMENT 1) FLEXION: DECREASE ANGLE BETWEEN TWO BONES OF A JOINT 2) EXTENSION: INCREASE ANGLE BETWEEN TWO BONES OF A JOINT 3) ADDUCTION: TOWARDS MIDLINE -

The Painful Shoulder Part II: Common Acute & Chronic Disorders
The Painful Shoulder Part II: Common Acute & Chronic Disorders © Jackson Orthopaedic Foundation www.jacksonortho.org Presenters AJ Benham, DNP, FNP, ONC Kathleen Geier, DNP, FNP, ONC Jackson Orthopedic Foundation 3317 Elm Street - Suite 102 Oakland, CA 94609 [email protected] [email protected] http://www.orthoprimarycare.info/ Conflict Of Interest Disclosures We hereby certify that, to the best of our knowledge, no aspect of our current personal or professional situation might reasonably be expected to affect significantly our views on the subject on which we are presenting. Objectives • 1. Differentiate among common conditions associated with shoulder pain based on history and physical exam • 2. Formulate plans for imaging and treatment of specific shoulder conditions according to evidence based guidelines. • 3. Discuss indications & appropriate communication techniques for referral of patients with shoulder conditions to services including PT, surgery, etc. Common Sites of Shoulder Pain A A good place for a chart ACUTE CHRONIC • Fractures • Impingement Syndrome Humerus • Frozen Shoulder Clavicle Adhesive capsulitis Scapula • Biceps Tendonitis • *Dislocations • Labral Injury Humerus SLAP Tear AC Joint • Osteoarthritis SC Joint Glenohumeral • *Rotator Cuff Tear Acromioclavicular S.I.T.S. Muscles • Osteolysis Distal clavicle Shoulder Landmarks A A good place for a chart More Shoulder Landmarks A A good place for a chart Musculoskeletal Exam • Inspection • Palpation * • Range of Motion • Resisted Strength • Sensation • Provocative Testing * One joint above; one below www.jacksonortho.org ACUTE CHRONIC • Fractures • Impingement Syndrome Clavicle • Frozen Shoulder Humerus Adhesive capsulitis Scapula • Biceps Tendonitis • *Dislocations • Labral Injury Humerus SLAP Tear AC Joint • Osteoarthritis SC Joint Glenohumeral • *Rotator Cuff Tear Acromioclavicular S.I.T.S. -

Periprosthetic Fractures
Periprosthetic Fractures SRS 2017 Stephen R Smith Orthopaedic Surgeon Northeast Nebraska Orthopaedics P C Norfolk Nebraska SRS 2017 Periprosthetic Fractures Fractures around Joint Replacements Mostly Lower Limb Knee Arthroplasty 700,000/ yr. Hip Arthroplasty 350,000/yr. Shoulder Arthroplasty ? 60,000/yr. Elbow Arthroplasty ? 20,000/yr. Periprosthetic Fractures Incidence Increasing due Increasing Demand and High Demands of Older Patients Projections 2025 2,000,000 (2 million) Knee Replacements 750,000 Total Hip Replacements Periprosthetic Fractures Risk Factors Mechanical Patient Factors Implant Loosening Rheumatoid Arthritis Chronic Steroid Use Neurologic Osteolysis Disease/Disorders Osteoporosis Osteopenia Femoral Notching Female Gender (Above TKA) Increasing Age SRS 2017 Periprosthetic Fractures Incidence Hip Intraoperative Acetabulum Cemented 0.2% Uncemented 0.4% During Impaction Under reaming> 2mm, Osteoporosis, Dysplasia Radiation Periprosthetic Fractures Incidence Hip Intraoperative Primary 0.1-5% Classification Osteoporosis,Cementless, Technique, Revision, Minimally Invasive, Revision 3-21% Periprosthetic Fractures Risk Factors DON’T FALL Remove Loose Rugs Minimize Stair Use Rail Stay Home in Bad Weather!!! Use Common Sense SRS 2017 Periprosthetic Fractures Risk Factors This Is Ice DON’T FALL Remove Loose Rugs Minimize Stair Use Rail Stay Home in Bad Weather!!! Use Common Sense SRS 2017 Periprosthetic Fractures Incidence Knee Intraoperative ?? Occasional Medial Femoral Condyle Often Tibial Crack after Stem Impaction Postoperative