Healthcare Tourism in India
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
How Does Eye Care Seeking Behaviour Change with Increasing Age and Visual Impairment? Intersectional Analysis of Older Adults In
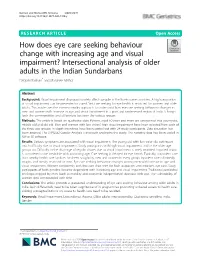
Barman and Mishra BMC Geriatrics (2020) 20:71 https://doi.org/10.1186/s12877-020-1438-y RESEARCH ARTICLE Open Access How does eye care seeking behaviour change with increasing age and visual impairment? Intersectional analysis of older adults in the Indian Sundarbans Debjani Barman* and Manasee Mishra Abstract Background: Visual impairment disproportionately affects people in the low-income countries. A high proportion of visual impairment can be prevented or cured. Yet, care seeking for eye health is restricted for women and older adults. This article uses the intersectionality approach to understand how eye care seeking behaviour changes in men and women with increase in age and visual impairment in a poor and underserved region of India. It brings forth the commonalities and differences between the various groups. Methods: The article is based on qualitative data. Persons aged 50 years and more are categorized into young-old, middle-old and old-old. Men and women with low vision/ high visual impairment have been selected from each of the three age groups. In-depth interviews have been carried out with 24 study participants. Data saturation has been attained. The JHPIEGO Gender Analysis Framework underpins the study. The narrative data has been coded in NVivo 10 software. Results: Various symptoms are associated with visual impairment. The young-old with low vision do not report much difficulty due to visual impairment. Study participants with high visual impairment, and in the older age groups do. Difficulty in the discharge of regular chores due to visual impairment is rarely reported. Impaired vision is considered to be inevitable with advancing age. -

India's Health Under Modi: Agenda for the Next Two Years
India’s Health Under Modi: Agenda for the Next Two Years Aparna Pande November 2016 Husain Haqqani Briefing Paper South Asia Program India's Health Under Modi: Agenda for the next Two Years Aparna Pande, Director, India Initiative Husain Haqqani, Director, South and Central Asia South Asia Program © 2016 Hudson Institute, Inc. All rights reserved. For more information about obtaining additional copies of this or other Hudson Institute publications, please visit Hudson’s website, www.hudson.org ABOUT HUDSON INSTITUTE Hudson Institute is a research organization promoting American leadership and global engagement for a secure, free, and prosperous future. Founded in 1961 by strategist Herman Kahn, Hudson Institute challenges conventional thinking and helps manage strategic transitions to the future through interdisciplinary studies in defense, international relations, economics, health care, technology, culture, and law. Hudson seeks to guide public policy makers and global leaders in government and business through a vigorous program of publications, conferences, policy briefings and recommendations. Visit www.hudson.org for more information. Hudson Institute 1201 Pennsylvania Avenue, N.W. Suite 400 Washington, D.C. 20004 P: 202.974.2400 [email protected] www.hudson.org Table of Contents Overview 5 India’s Healthcare Trends 8 India’s Statistical Healthcare Profile 8 India’s Health Compared with Other Nations 13 Modi Government’s Two Year Performance 25 National Health Policy 25 Swaach Bharat (Clean India) 28 Infrastructure and Services 32 The Private Sector 34 Challenges & Opportunities: The Next Two Years 37 Accessibility 37 Affordability and Innovation 40 Challenges and Opportunities 43 India’s Health Under Modi 4 India’s Health Under Modi Overview rime Minister Narendra Modi came to power in May 2014 promising changes in a number of areas, including healthcare. -

Sustainable Strategies for a Healthy India: Imperatives for Consolidating the Healthcare Management Ecosystem
Sustainable Strategies for a Healthy India: Imperatives for Consolidating the Healthcare Management Ecosystem For private circulation only June 2013 www.deloitte.com/in Contents Health in India 1 Emerging trends and imperatives 3 Collaborate to Innovate 6 Creating and facilitating a collaborative environment 13 References 14 Contacts 16 2 Health in India – Status and successes India rightly brands itself as incredible. in-patient treatment, possibly making The country’s remarkable political, quality healthcare and private sector economic and cultural transformation facilities accessible to the poor. over the past few decades has made it a geopolitical force. Healthcare is However, these exciting opportunities one of the industries that marks this often mask certain urgent predicaments. strengthened global presence. The healthcare sector in India is As per industry reports, healthcare is currently at a cusp. Issues of access, poised to grow at an estimated annual affordability, quality of care and rate of 19 per cent to reach USD efficiency remain significant. A number 280 billion by 20201 with India being of reports have been published about recognized as a destination for world the poor health status of India, class healthcare. During the last decade compared to its Low and Middle the private sector grew to become the Income Country (LMIC) peers. In terms major provider of healthcare services. of vital statistics like infant mortality Its share of beds increased from 49 (IMR) and maternal mortality, India has per cent in 2002 to 63 per cent in lagged behind significantly. Even life 20102. As per NSSO 2008, the private expectancy, at 62 years, is three years sector accounted for 60 percent of all below the LMIC average. -

Report on Mapping of Healthcare Sector in India
Report on Mapping of Healthcare Sector in India SWECARE AND SWEDISH TRADE COUNCIL, INDIA 2012 This page has been intentionally left blank Page 2 of 294 Table of Contents 1. EXECUTIVE SUMMARY ......................................................................................................................... 8 1.1. OVERVIEW - HEALTH SITUATION IN INDIA .................................................................................................... 8 1.2. SHORTLISTED SECTORS AND MAJOR BUSINESS OPPORTUNITIES............................................................... 11 1.3. PERCEPTION REGARDING SWEDISH TECHNOLOGIES AND SOLUTIONS ........................................................ 22 2. HEALTHCARE SECTOR IN INDIA ....................................................................................................... 24 2.1. OVERVIEW ............................................................................................................................................. 24 3. MAJOR HEALTHCARE PROGRAMS .................................................................................................. 33 3.1. NATIONAL RURAL HEALTH MISSION ......................................................................................................... 34 3.2. NATIONAL URBAN HEALTH MISSION ......................................................................................................... 39 3.3. NATIONAL VECTOR BORNE DISEASE CONTROL PROGRAM ........................................................................ 42 3.4. REVISED -

International Profiles of Health Care Systems
EDITED BY Elias Mossialos and Ana Djordjevic London School of Economics and Political Science MAY 2017 MAY Robin Osborn and Dana Sarnak The Commonwealth Fund International Profiles of Health Care Systems Australia, Canada, China, Denmark, England, France, Germany, India, Israel, Italy, Japan, the Netherlands, New Zealand, Norway, Singapore, Sweden, Switzerland, Taiwan, and the United States THE COMMONWEALTH FUND is a private foundation that promotes a high performance health care system providing better access, improved quality, and greater efficiency. The Fund’s work focuses particularly on society’s most vulnerable, including low-income people, the uninsured, minority Americans, young children, and elderly adults. The Fund carries out this mandate by supporting independent research on health care issues and making grants to improve health care practice and policy. An international program in health policy is designed to stimulate innovative policies and practices in the United States and other industrialized countries. MAY 2017 International Profiles of Health Care Systems Australia EDITED BY Canada Elias Mossialos and Ana Djordjevic London School of Economics and Political Science China Denmark Robin Osborn and Dana Sarnak The Commonwealth Fund England France To learn more about new publications when they become available, Germany visit the Fund’s website and register to receive email alerts. India Israel Italy Japan The Netherlands New Zealand Norway Singapore Sweden Switzerland Taiwan United States CONTENTS Table 1. Health Care System Financing and Coverage in 19 Countries . 6 Table 2. Selected Health Care System Indicators for 18 Countries . 7 Table 3. Selected Health System Performance Indicators for 17 Countries. 8 Table 4. Provider Organization and Payment in 19 Countries . -

District Health Society Begusarai
DISTRICT HEALTH ACTION PLAN 2012-2013 DISTRICT HEALTH SOCIETY BEGUSARAI-1- Foreword This District Health Action Plan (DHAP) is one of the key instruments to achieve NRHM goals. This plan is based on health needs of the district and recognizing the importance of Health in the process of economic and social development and improving the quality of life of our citizens, the Government of India has resolved to launch the National Rural Health Mission to carry out necessary architectural correction in the basic health care delivery system. After a thorough situation analysis of district health scenario this document has been prepared. In the plan, it is addressing health care needs of rural poor especially women and children, the teams have analyzed the coverage of poor women and children with preventive and primitive interventions, barriers in access to health care and spread of human resources catering health needs in the district. The focus has also been given on current availability of health care infrastructure in public/NGO/private sector, availability of wide range of providers. This DHAP has been evolved through a participatory and consultative process, wherein community and other stakeholders have participated and ascertained their specific health needs in villages, problems in accessing health services, especially poor women and children at local level. The goals of the Mission are to improve the availability of and access to quality health care by people, especially for those residing in rural areas, the poor, women and children. I need to congratulate the department of Health and Family Welfare and State Health Society of Bihar for their dynamic leadership of the health sector reform programme and we look forward to a rigorous and analytic documentation of their experiences so that we can learn from them and replicate successful strategies. -
Artificial Intelligence and Healthcare in India
CSD Working Paper Series: Towards a New Indian Model of Information and Communications Technology-Led Growth and Development Artificial Intelligence and Healthcare in India ICT India Working Paper #43 Nirupam Bajpai and Manisha Wadhwa January 2020 CSD Working Paper Series – Artificial Intelligence and Healthcare in India Abstract Artificial Intelligence (AI), also referred to as the new electricity, is the emerging focus area in India. AI refers to the ability of machines to perform cognitive tasks like thinking, perceiving, learning, problem solving and decision making. Most of the AI systems rely on historical large datasets for predicting future trends and outcomes at a pace which humans would not be able to match. The development of AI in India is in the initial stages and there is no regulatory body focused solely on AI. However, recently, Government of India has taken various initiatives related to AI such as establishment of Artificial Intelligence Task Force, formulation of NITI Aayog's National Strategy for Artificial Intelligence #AIFORALL, setting up of four Committees for AI under Ministry of Electronics and Information technology etc. Some of India’s state governments have also taken few initiatives, such as establishment of Centre of Excellence for Data Science and Artificial Intelligence (CoE-DS&AI) by Karnataka, Safe and Ethical Artificial Intelligence Policy 2020 and Face Recognition Attendance System by Tamil Nadu, AI-Powered System for monitoring driving behaviour by West Bengal, AI System to fight agricultural risks by Maharashtra etc. As with any other technology, AI brings with it a span of opportunities and challenges. In healthcare, AI could be beneficial in mining medical records; designing treatment plans; forecasting health events; assisting repetitive jobs; doing online consultations; assisting in clinical decision making; medication management; drug creation; making healthier choices and decisions; and solving public health problems etc. -

India and the Global Economy
India and the Global Economy A collection of essays presented at the Hudson Institute-Observer Research Foundation Roundtable on “India’s Economic Engagements with the World,” New Delhi, India, March 25-26, 2014 Edited by Husain Haqqani July 2014 India and the Global Economy A collection of essays presented at the Hudson Institute-Observer Research Foundation Roundtable on “India’s Economic Engagements with the World” held in New Delhi, India on March 25-26, 2014 Edited by Husain Haqqani © 2014 Hudson Institute, Inc. All rights reserved. For more information about obtaining additional copies of this or other Hudson Institute publications, please visit Hudson’s website, www.hudson.org ABOUT HUDSON INSTITUTE Hudson Institute is an independent research organization promoting new ideas for the advancement of global security, prosperity and freedom. Founded in 1961 by strategist Herman Kahn, Hudson Institute challenges conventional thinking and helps manage strategic transitions to the future through interdisciplinary studies in defense, international relations, economics, health care, technology, culture, and law. Hudson seeks to guide public policy makers and global leaders in government and business through a vigorous program of publications, conferences, policy briefings and recommendations. Visit www.hudson.org for more information. Hudson Institute 1015 15th Street, N.W. Sixth Floor Washington, D.C. 20005 P: 202.974.2400 [email protected] www.hudson.org Table of Contents Introduction India’s Reform Agenda Husain Haqqani 1 Innovation, Intellectual -

India: Medical and Healthcare Provision
Country Policy and Information Note India: Medical and healthcare provision Version 1.0 October 2020 Preface Purpose and use This note provides country of origin information (COI) for decision makers handling cases where a person claims that to remove them from the UK would be a breach of Articles 3 and/or 8 of the European Convention on Human Rights (ECHR) because of an ongoing health condition. It is not intended to be an exhaustive survey of healthcare in India. Country of origin information The country information in this note has been carefully selected in accordance with the general principles of COI research as set out in the Common EU [European Union] Guidelines for Processing Country of Origin Information (COI), dated April 2008, and the Austrian Centre for Country of Origin and Asylum Research and Documentation’s (ACCORD), Researching Country Origin Information – Training Manual, 2013. Namely, taking into account the COI’s relevance, reliability, accuracy, balance, currency, transparency and traceability. The structure and content of the country information section follows a terms of reference which sets out the general and specific topics relevant to this note. All information included in the note was published or made publicly available on or before the ‘cut-off’ date in the country information section. Any event taking place or report/article published after this date is not included. All information is publicly accessible or can be made publicly available, and is from generally reliable sources. Sources and the information they provide are carefully considered before inclusion. Factors relevant to the assessment of the reliability of the sources and information include: x the motivation, purpose, knowledge and experience of the source x how the information was obtained, including specific methodologies used x the currency and detail of information, and x whether the COI is consistent with and/or corroborated by other sources. -

Public Hospital Governance in India: a Study of All India Institute of Medical Sciences, New Delhi Asia Pacific Observatory
Public Hospital Governance in India _________________ A study of All India Institute of Medical Sciences (AIIMS), New Delhi • Dr Shakti Kumar Gupta, Head, Department of Hospital Administration and Medical Superintendent, All India Institute of Medical Sciences, New Delhi, India • Dr Angel Rajan Singh, Senior Resident Administrator, Department of Hospital Administration, All India Institute of Medical Sciences, New Delhi, India • Dr Arunachalam Gunasekar, Technical Officer (Universal Health Coverage), WHO Country Office for India • Dr Parmeshwar Kumar, Senior Resident Administrator, Department of Hospital Administration, All India Institute of Medical Sciences, New Delhi, India • Dr Chandrakant Lahariya, Routine Immunization and New Vaccines focal person, WHO Country Office for India • Mr Kamal Gulati, Project Manager, Department of Hospital Administration, All India Institute of Medical Sciences, New Delhi, India • Dr Antonio Duran, Chief Executive Officer, Tecnicas de Salud, Spain Methodology • Review of existing literature and data sources • Supplemented by key informant interviews • The case study used both explicit and tacit knowledge as evidence, the later coming from the participation of senior hospital managers and other national experts as key informants during focused group discussion and / or individual interviews (loosely structured, in-depth discussions). • Draft discussion guides & topic points were shared across the working group members to enhance comparability of the case studies’ findings. • Conceptual framework given -

Financing Healthcare for All in India: Towards a Common Goal
Financing Healthcare for all in India: Towards a Common Goal Oommen C. Kurian a ACKNOWLEDGEMENTS Author: Oommen C. Kurian Inputs: Indranil Mukhopadhyay, Anant Phadke, VR Raman, Shabareesh Pillai, Sadanand Nadkarni, Chandrakant Lahariya, Katie Malouf Bous (Oxfam International), Nicolas Mombrial (Oxfam International), Deepak Xavier(Oxfam India), Pallavi Gupta(Oxfam India), and Pooja Parvati (Oxfam India). A draft of this paper was circulated for comments and feedback at the first ever Universal Health Coverage Day commemorative event jointly organised by the World Health Organisation, Public Health Foundation of India, Rockefeller Foundation and Oxfam India. The event was held on the 12th December 2014 at New Delhi, India. © Oxfam India May, 2015 This publication is copyright but the text may be used free of charge for the purposes of advocacy, campaigning, education, and research, provided that the source is acknowledged in full. The copyright holder requests that all such use be registered with them for impact assessment purposes. For copying in any other circumstances, permission must be secured. E-mail: [email protected]/ PUBLISHED BY Oxfam India: 4th and 5th Floor, Shriram Bharatiya Kala Kendra, 1, Copernicus Marg, New Delhi 110001 Tel: +91 (0) 11 4653 8000 www.oxfamindia.org Oxfam India Oxfam India, a fully independent Indian organization, is a member of an international confederation of 17 organisations. The Oxfams are rights- based organizations, which fight poverty and injustice by linking grassroots interventions, to local, national, and global policy developments. For further information please write to: [email protected], or visit our website: www.oxfamindia.org. Photographs by: Srikanth Kolari Oxfam India Working Paper Series disseminates findings of its work in progress to encourage the exchange of ideas about development issues. -

Critical Analysis of Policy Gaps in the Indian Healthcare Delivery
Health Infrastructure in India: Critical Analysis of Policy Gaps in the Indian Healthcare Delivery Occasional Paper July - 2012 Health Infrastructure in India: Critical Analysis of Policy Gaps in the Indian Healthcare Delivery 2 of 32 About the Authors Avneesh Kumar and Saurav Gupta are studying in the fifth year of B.A.LL.B.(Hons.) course at Dr. Ram Manohar Lohiya National Law University, Lucknow, India. Both the authors are research analysts who write on wide variety of subjects relevant to India’s national interests and objectives. http://www.vifindia.org © Vivekananda International Foundation Health Infrastructure in India: Critical Analysis of Policy Gaps in the Indian Healthcare Delivery 3 of 32 Health Infrastructure in India: Critical Analysis of Policy Gaps in the Indian Healthcare Delivery Abstract Today the health infrastructure of India is in pathetic condition, it needs radical reforms to deal with new emerging challenges. On the one hand the role of private players is continuously increasing in healthcare sector, but simultaneously healthcare facilities are getting costly, and becoming non-accessible for the poor. The government hospitals are facing the problem of lack of resources and infrastructure; there are inadequate number of beds, rooms, and medicines. In this research paper the authors have discussed the present scenario of healthcare facilities and personnel. On the part of government there is lack of monitoring of the funds and resources, which are devoted towards the improvement of healthcare sector. The authors have suggested a model healthcare plan which devolves around preparing a long term strategy for qualitative as well as quantitative improvements in our healthcare infrastructure by focusing on workforce capacity and competency, information and data systems, and organizational capacity.