Identifying Disease-Associated Genes Based on Artificial Intelligence
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Whole Exome Sequencing in Families at High Risk for Hodgkin Lymphoma: Identification of a Predisposing Mutation in the KDR Gene
Hodgkin Lymphoma SUPPLEMENTARY APPENDIX Whole exome sequencing in families at high risk for Hodgkin lymphoma: identification of a predisposing mutation in the KDR gene Melissa Rotunno, 1 Mary L. McMaster, 1 Joseph Boland, 2 Sara Bass, 2 Xijun Zhang, 2 Laurie Burdett, 2 Belynda Hicks, 2 Sarangan Ravichandran, 3 Brian T. Luke, 3 Meredith Yeager, 2 Laura Fontaine, 4 Paula L. Hyland, 1 Alisa M. Goldstein, 1 NCI DCEG Cancer Sequencing Working Group, NCI DCEG Cancer Genomics Research Laboratory, Stephen J. Chanock, 5 Neil E. Caporaso, 1 Margaret A. Tucker, 6 and Lynn R. Goldin 1 1Genetic Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 2Cancer Genomics Research Laboratory, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 3Ad - vanced Biomedical Computing Center, Leidos Biomedical Research Inc.; Frederick National Laboratory for Cancer Research, Frederick, MD; 4Westat, Inc., Rockville MD; 5Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; and 6Human Genetics Program, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD, USA ©2016 Ferrata Storti Foundation. This is an open-access paper. doi:10.3324/haematol.2015.135475 Received: August 19, 2015. Accepted: January 7, 2016. Pre-published: June 13, 2016. Correspondence: [email protected] Supplemental Author Information: NCI DCEG Cancer Sequencing Working Group: Mark H. Greene, Allan Hildesheim, Nan Hu, Maria Theresa Landi, Jennifer Loud, Phuong Mai, Lisa Mirabello, Lindsay Morton, Dilys Parry, Anand Pathak, Douglas R. Stewart, Philip R. Taylor, Geoffrey S. Tobias, Xiaohong R. Yang, Guoqin Yu NCI DCEG Cancer Genomics Research Laboratory: Salma Chowdhury, Michael Cullen, Casey Dagnall, Herbert Higson, Amy A. -
Supplementary Data
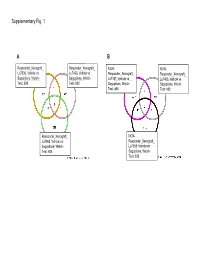
Supplementary Fig. 1 A B Responder_Xenograft_ Responder_Xenograft_ NON- NON- Lu7336, Vehicle vs Lu7466, Vehicle vs Responder_Xenograft_ Responder_Xenograft_ Sagopilone, Welch- Sagopilone, Welch- Lu7187, Vehicle vs Lu7406, Vehicle vs Test: 638 Test: 600 Sagopilone, Welch- Sagopilone, Welch- Test: 468 Test: 482 Responder_Xenograft_ NON- Lu7860, Vehicle vs Responder_Xenograft_ Sagopilone, Welch - Lu7558, Vehicle vs Test: 605 Sagopilone, Welch- Test: 333 Supplementary Fig. 2 Supplementary Fig. 3 Supplementary Figure S1. Venn diagrams comparing probe sets regulated by Sagopilone treatment (10mg/kg for 24h) between individual models (Welsh Test ellipse p-value<0.001 or 5-fold change). A Sagopilone responder models, B Sagopilone non-responder models. Supplementary Figure S2. Pathway analysis of genes regulated by Sagopilone treatment in responder xenograft models 24h after Sagopilone treatment by GeneGo Metacore; the most significant pathway map representing cell cycle/spindle assembly and chromosome separation is shown, genes upregulated by Sagopilone treatment are marked with red thermometers. Supplementary Figure S3. GeneGo Metacore pathway analysis of genes differentially expressed between Sagopilone Responder and Non-Responder models displaying –log(p-Values) of most significant pathway maps. Supplementary Tables Supplementary Table 1. Response and activity in 22 non-small-cell lung cancer (NSCLC) xenograft models after treatment with Sagopilone and other cytotoxic agents commonly used in the management of NSCLC Tumor Model Response type -

Mccartney, Karen M. (2015)
THE ROLE OF PEROXISOME PROLIFERATOR ACTIVATED RECEPTOR ALPHA (PPARα) IN THE EFFECT OF PIROXICAM ON COLON CANCER KAREN MARIE McCARTNEY BSc. (Hons), MSc. Thesis submitted to the University of Nottingham for the degree of Doctor of Philosophy April 2015 Abstract Studies with APCMin/+ mice and APCMin/+ PPARα-/- mice were undertaken to investigate whether polyp development in the mouse gut was mediated by PPARα. Additionally, the effect of piroxicam treatment dependency on PPARα was assessed. Results showed the number of polyps in the colon was significantly higher in APCMin/+ PPARα-/- mice than in APCMin/+ mice, whilst in the small bowel the difference was not significant. Analysis of gene expression in the colon with Affymetrix® microarrays demonstrated the largest source of variation was between tumour and normal tissue. Deletion of PPARα had little effect on gene expression in normal tissue but appeared to have more effect in tumour tissue. Ingenuity pathway analysis of these data showed the top biological processes were growth & proliferation and colorectal cancer. Collectively, these data may indicate that deletion of PPARα exacerbates the existing APCMin/+ mutation to promote tumorigenesis in the colon. 95 genes from Affymetrix® microarray data were selected for further analysis on Taqman® low density arrays. There was good correlation of expression levels between the two array types. Expression data of two genes proved particularly interesting; Onecut homeobox 2 (Onecut2) and Apolipoprotein B DNA dC dU - editing enzyme, catalytic polypeptide 3 (Apobec3). Onecut2 was highly up-regulated in tumour tissue. Apobec3 was up-regulated in APCMin/+ PPARα-/- mice only; suggesting expression was mediated via PPARα. There was a striking increase in survival accompanied by a marked reduction in small intestinal polyp numbers in mice of either genotype that received piroxicam. -

Molecular Correlates of Metastasis by Systematic Pan-Cancer Analysis Across the Cancer Genome Atlas
Author Manuscript Published OnlineFirst on November 6, 2018; DOI: 10.1158/1541-7786.MCR-18-0601 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Molecular correlates of metastasis by systematic pan-cancer analysis across The Cancer Genome Atlas Fengju Chen1*, Yiqun Zhang1*, Sooryanarayana Varambally2,3, Chad J. Creighton1,4,5,6 1. Dan L. Duncan Comprehensive Cancer Center Division of Biostatistics, Baylor College of Medicine, Houston, TX, USA. 2. Comprehensive Cancer Center, University of Alabama at Birmingham, Birmingham, AL 35233, USA 3. Molecular and Cellular Pathology, Department of Pathology, University of Alabama at Birmingham, Birmingham, AL 35233, USA 4. Department of Bioinformatics and Computational Biology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA 5. Human Genome Sequencing Center, Baylor College of Medicine, Houston, TX 77030, USA 6. Department of Medicine, Baylor College of Medicine, Houston, TX, USA * co-first authors Running title: Pan-cancer metastasis correlates Abbreviations: TCGA, The Cancer Genome Atlas; RNA-seq, RNA sequencing; RPPA, reverse- phase protein arrays Correspondence to: Chad J. Creighton ([email protected]) One Baylor Plaza, MS305 Houston, TX 77030 Disclosure of potential conflicts of interest: The authors have no conflicts of interest. 1 Downloaded from mcr.aacrjournals.org on September 28, 2021. © 2018 American Association for Cancer Research. Author Manuscript Published OnlineFirst on November 6, 2018; DOI: 10.1158/1541-7786.MCR-18-0601 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Abstract Tumor metastasis is a major contributor to cancer patient mortality, but the process remains poorly understood. -

Characterizing Genomic Duplication in Autism Spectrum Disorder by Edward James Higginbotham a Thesis Submitted in Conformity
Characterizing Genomic Duplication in Autism Spectrum Disorder by Edward James Higginbotham A thesis submitted in conformity with the requirements for the degree of Master of Science Graduate Department of Molecular Genetics University of Toronto © Copyright by Edward James Higginbotham 2020 i Abstract Characterizing Genomic Duplication in Autism Spectrum Disorder Edward James Higginbotham Master of Science Graduate Department of Molecular Genetics University of Toronto 2020 Duplication, the gain of additional copies of genomic material relative to its ancestral diploid state is yet to achieve full appreciation for its role in human traits and disease. Challenges include accurately genotyping, annotating, and characterizing the properties of duplications, and resolving duplication mechanisms. Whole genome sequencing, in principle, should enable accurate detection of duplications in a single experiment. This thesis makes use of the technology to catalogue disease relevant duplications in the genomes of 2,739 individuals with Autism Spectrum Disorder (ASD) who enrolled in the Autism Speaks MSSNG Project. Fine-mapping the breakpoint junctions of 259 ASD-relevant duplications identified 34 (13.1%) variants with complex genomic structures as well as tandem (193/259, 74.5%) and NAHR- mediated (6/259, 2.3%) duplications. As whole genome sequencing-based studies expand in scale and reach, a continued focus on generating high-quality, standardized duplication data will be prerequisite to addressing their associated biological mechanisms. ii Acknowledgements I thank Dr. Stephen Scherer for his leadership par excellence, his generosity, and for giving me a chance. I am grateful for his investment and the opportunities afforded me, from which I have learned and benefited. I would next thank Drs. -

Canine Polydactyl Mutations with Heterogeneous Origin in the Conserved Intronic Sequence of LMBR1 Kiyun Park*, Joohyun Kang*, Kr
Genetics: Published Articles Ahead of Print, published on August 9, 2008 as 10.1534/genetics.108.087114 Canine polydactyl mutations with heterogeneous origin in the conserved intronic sequence of LMBR1 Kiyun Park*, Joohyun Kang*, Krishna Pd. Subedi*, Ji-Hong Ha†, and Chankyu Park*1 * Department of Biological Sciences, Korea Advanced Institute of Science and Technology, Yuseong-gu, Daejon 305-701, Republic of Korea †Department of Genetic Engineering, College of Natural Sciences, Kyungpook National University,1370 Sankyuk-dong, Daegu 702-701, Republic of Korea 1 Running title: LMBR1 and canine polydactyly Keywords: Polydactyly; canine breed; linkage analysis; C7orf2/LMBR1; multi-species conserved sequence 1Corresponding author: Chankyu Park Department of Biological Sciences, Korea Advanced Institute of Science and Technology, Yuseong- gu, Daejon 305-701, Republic of Korea.E-mail: [email protected], Phone: 82-42-869-2629 2 ABSTRACT Canine preaxial polydactyly (PPD) in the hind limb is a developmental trait that restores the first digit lost during canine evolution. Using a linkage analysis, we demonstrated previously that the affected gene in a Korean breed is located on canine chromosome 16. The candidate locus was further limited to a linkage disequilibrium (LD) block of less than 213 kb comprising the single gene, LMBR1, by LD mapping with single-nucleotide polymorphisms (SNPs) for affected individuals from both Korean and Western breeds. The ZPA regulatory sequence (ZRS) in intron 5 of LMBR1 was implicated in mammalian polydactyly. An analysis of the LD haplotypes around the ZRS for various dog breeds revealed that only a subset is assigned to Western breeds. Furthermore, two distinct affected haplotypes for Asian and Western breeds were found, each containing different single-base changes in the upstream sequence (pZRS) of the ZRS. -

Molecular Targeting and Enhancing Anticancer Efficacy of Oncolytic HSV-1 to Midkine Expressing Tumors
University of Cincinnati Date: 12/20/2010 I, Arturo R Maldonado , hereby submit this original work as part of the requirements for the degree of Doctor of Philosophy in Developmental Biology. It is entitled: Molecular Targeting and Enhancing Anticancer Efficacy of Oncolytic HSV-1 to Midkine Expressing Tumors Student's name: Arturo R Maldonado This work and its defense approved by: Committee chair: Jeffrey Whitsett Committee member: Timothy Crombleholme, MD Committee member: Dan Wiginton, PhD Committee member: Rhonda Cardin, PhD Committee member: Tim Cripe 1297 Last Printed:1/11/2011 Document Of Defense Form Molecular Targeting and Enhancing Anticancer Efficacy of Oncolytic HSV-1 to Midkine Expressing Tumors A dissertation submitted to the Graduate School of the University of Cincinnati College of Medicine in partial fulfillment of the requirements for the degree of DOCTORATE OF PHILOSOPHY (PH.D.) in the Division of Molecular & Developmental Biology 2010 By Arturo Rafael Maldonado B.A., University of Miami, Coral Gables, Florida June 1993 M.D., New Jersey Medical School, Newark, New Jersey June 1999 Committee Chair: Jeffrey A. Whitsett, M.D. Advisor: Timothy M. Crombleholme, M.D. Timothy P. Cripe, M.D. Ph.D. Dan Wiginton, Ph.D. Rhonda D. Cardin, Ph.D. ABSTRACT Since 1999, cancer has surpassed heart disease as the number one cause of death in the US for people under the age of 85. Malignant Peripheral Nerve Sheath Tumor (MPNST), a common malignancy in patients with Neurofibromatosis, and colorectal cancer are midkine- producing tumors with high mortality rates. In vitro and preclinical xenograft models of MPNST were utilized in this dissertation to study the role of midkine (MDK), a tumor-specific gene over- expressed in these tumors and to test the efficacy of a MDK-transcriptionally targeted oncolytic HSV-1 (oHSV). -

A 1.35 Mb DNA Fragment Is Inserted Into the DHMN1 Locus on Chromosome 7Q34–Q36.2
Hum Genet (2016) 135:1269–1278 DOI 10.1007/s00439-016-1720-4 ORIGINAL INVESTIGATION A 1.35 Mb DNA fragment is inserted into the DHMN1 locus on chromosome 7q34–q36.2 Alexander P. Drew1 · Anthony N. Cutrupi1,3 · Megan H. Brewer1,3 · Garth A. Nicholson1,2,3 · Marina L. Kennerson1,2,3 Received: 5 April 2016 / Accepted: 25 July 2016 / Published online: 3 August 2016 © Springer-Verlag Berlin Heidelberg 2016 Abstract Distal hereditary motor neuropathies predomi- for hereditary motor neuropathies and highlights the grow- nantly affect the motor neurons of the peripheral nervous ing importance of interrogating the non-coding genome for system leading to chronic disability. Using whole genome SV mutations in families which have been excluded for sequencing (WGS) we have identified a novel structural genome wide coding mutations. variation (SV) within the distal hereditary motor neuropa- thy locus on chromosome 7q34–q36.2 (DHMN1). The SV involves the insertion of a 1.35 Mb DNA fragment Introduction into the DHMN1 disease locus. The source of the inserted sequence is 2.3 Mb distal to the disease locus at chromo- The distal hereditary motor neuropathies (dHMN) are a some 7q36.3. The insertion involves the duplication of five group of progressive neurodegenerative disorders that pri- genes (LOC389602, RNF32, LMBR1, NOM1, MNX1) and marily affect the motor neurons of distal limbs without partial duplication of UBE3C. The genomic structure of affecting sensory neurons. The disorder is a length depend- genes within the DHMN1 locus are not disrupted by the ant neuropathy in which the longest nerves are initially insertion and no disease causing point mutations within affected. -
Mapping the Shh Long-Range Regulatory Domain
Edinburgh Research Explorer Mapping the Shh long-range regulatory domain Citation for published version: Anderson, E, Devenney, PS, Hill, RE & Lettice, LA 2014, 'Mapping the Shh long-range regulatory domain', Development, vol. 141, no. 20, pp. 3934-3943. https://doi.org/10.1242/dev.108480 Digital Object Identifier (DOI): 10.1242/dev.108480 Link: Link to publication record in Edinburgh Research Explorer Document Version: Publisher's PDF, also known as Version of record Published In: Development Publisher Rights Statement: This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution and reproduction in any medium provided that the original work is properly attributed. General rights Copyright for the publications made accessible via the Edinburgh Research Explorer is retained by the author(s) and / or other copyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associated with these rights. Take down policy The University of Edinburgh has made every reasonable effort to ensure that Edinburgh Research Explorer content complies with UK legislation. If you believe that the public display of this file breaches copyright please contact [email protected] providing details, and we will remove access to the work immediately and investigate your claim. Download date: 04. Oct. 2021 Development ePress. Posted online 24 September 2014 © 2014. Published by The Company of Biologists Ltd | Development (2014) 141, 1-10 doi:10.1242/dev.108480 RESEARCH ARTICLE Mapping the Shh long-range regulatory domain Eve Anderson, Paul S. -

Mapping the Shh Long-Range Regulatory Domain Eve Anderson, Paul S
© 2014. Published by The Company of Biologists Ltd | Development (2014) 141, 3934-3943 doi:10.1242/dev.108480 RESEARCH ARTICLE Mapping the Shh long-range regulatory domain Eve Anderson, Paul S. Devenney, Robert E. Hill* and Laura A. Lettice ABSTRACT spatiotemporal pattern of expression. With the coding region lying Coordinated gene expression controlled by long-distance enhancers is adjacent to a large gene desert, the expression is controlled by a cis orchestrated by DNA regulatory sequences involving transcription group of -regulators, many of which were identified by mouse factors and layers of control mechanisms. The Shh gene and well- transgenic reporter assays. Epstein et al. (1999) identified two ∼ established regulators are an example of genomic composition in intronic enhancers and one outside the gene, lying 9 kb upstream Shh Shh lacZ which enhancers reside in a large desert extending into neighbouring of . These potential enhancers of activate reporter genes to control the spatiotemporal pattern of expression. Exploiting expression within the ventral midline of the spinal cord and the local hopping activity of the Sleeping Beauty transposon, the hindbrain and the ventral midbrain and caudal region of the lacZ reporter gene was dispersed throughout the Shh region to diencephalon. A further study, using comparative sequence analysis systematically map the genomic features responsible for expression and mouse reporter assays, uncovered three forebrain enhancers Shh activity. We found that enhancer activities are retained inside a located 300-450 kb upstream of (Jeong et al., 2006). genomic region that corresponds to the topological associated domain Comparative genomics was also used to identify another more cis (TAD) defined by Hi-C. -

Milger Et Al. Pulmonary CCR2+CD4+ T Cells Are Immune Regulatory And
Milger et al. Pulmonary CCR2+CD4+ T cells are immune regulatory and attenuate lung fibrosis development Supplemental Table S1 List of significantly regulated mRNAs between CCR2+ and CCR2- CD4+ Tcells on Affymetrix Mouse Gene ST 1.0 array. Genewise testing for differential expression by limma t-test and Benjamini-Hochberg multiple testing correction (FDR < 10%). Ratio, significant FDR<10% Probeset Gene symbol or ID Gene Title Entrez rawp BH (1680) 10590631 Ccr2 chemokine (C-C motif) receptor 2 12772 3.27E-09 1.33E-05 9.72 10547590 Klrg1 killer cell lectin-like receptor subfamily G, member 1 50928 1.17E-07 1.23E-04 6.57 10450154 H2-Aa histocompatibility 2, class II antigen A, alpha 14960 2.83E-07 1.71E-04 6.31 10590628 Ccr3 chemokine (C-C motif) receptor 3 12771 1.46E-07 1.30E-04 5.93 10519983 Fgl2 fibrinogen-like protein 2 14190 9.18E-08 1.09E-04 5.49 10349603 Il10 interleukin 10 16153 7.67E-06 1.29E-03 5.28 10590635 Ccr5 chemokine (C-C motif) receptor 5 /// chemokine (C-C motif) receptor 2 12774 5.64E-08 7.64E-05 5.02 10598013 Ccr5 chemokine (C-C motif) receptor 5 /// chemokine (C-C motif) receptor 2 12774 5.64E-08 7.64E-05 5.02 10475517 AA467197 expressed sequence AA467197 /// microRNA 147 433470 7.32E-04 2.68E-02 4.96 10503098 Lyn Yamaguchi sarcoma viral (v-yes-1) oncogene homolog 17096 3.98E-08 6.65E-05 4.89 10345791 Il1rl1 interleukin 1 receptor-like 1 17082 6.25E-08 8.08E-05 4.78 10580077 Rln3 relaxin 3 212108 7.77E-04 2.81E-02 4.77 10523156 Cxcl2 chemokine (C-X-C motif) ligand 2 20310 6.00E-04 2.35E-02 4.55 10456005 Cd74 CD74 antigen -

Cross-Species Alcohol Dependence-Associated Gene Networks: Co-Analysis Of
bioRxiv preprint doi: https://doi.org/10.1101/380584; this version posted July 30, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 1 1 Cross-species alcohol dependence-associated gene networks: Co-analysis of 2 mouse brain gene expression and human genome-wide association data 3 4 Short Title: Cross-species analysis reveals alcohol dependence-associated gene networks 5 6 Kristin M. Mignogna2,3,4, Silviu A. Bacanu2,3, Brien P. Riley2,3, Aaron R. Wolen5, Michael F. 7 Miles1,3* 8 9 1 Department of Pharmacology and Toxicology, Virginia Commonwealth University, Richmond, 10 Virginia, United States of America 11 2 Virginia Institute for Psychiatric and Behavioral Genetics, Virginia Commonwealth University, 12 Richmond, Virginia, United States of America 13 3 VCU Alcohol Research Center, Virginia Commonwealth University, Richmond, Virginia, 14 United States of America 15 4 VCU Center for Clinical & Translational Research, Virginia Commonwealth University, 16 Richmond, Virginia, United States of America 17 5Department of Human and Molecular Genetics, Virginia Commonwealth University, Richmond, 18 Virginia, United States of America 19 20 * Corresponding author 21 E-mail: [email protected] bioRxiv preprint doi: https://doi.org/10.1101/380584; this version posted July 30, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license.