Photobarr, INN-Porfimer Sodium
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(12) Patent Application Publication (10) Pub. No.: US 2012/0190743 A1 Bain Et Al
US 2012O190743A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2012/0190743 A1 Bain et al. (43) Pub. Date: Jul. 26, 2012 (54) COMPOUNDS FOR TREATING DISORDERS Publication Classification OR DISEASES ASSOCATED WITH (51) Int. Cl NEUROKININ 2 RECEPTORACTIVITY A6II 3L/23 (2006.01) (75) Inventors: Jerald Bain, Toronto (CA); Joel CD7C 69/30 (2006.01) Sadavoy, Toronto (CA); Hao Chen, 39t. ii; C Columbia, MD (US); Xiaoyu Shen, ( .01) Columbia, MD (US) A6IPI/00 (2006.01) s A6IP 29/00 (2006.01) (73) Assignee: UNITED PARAGON A6IP II/00 (2006.01) ASSOCIATES INC., Guelph, ON A6IPI3/10 (2006.01) (CA) A6IP 5/00 (2006.01) A6IP 25/00 (2006.01) (21) Appl. No.: 13/394,067 A6IP 25/30 (2006.01) A6IP5/00 (2006.01) (22) PCT Filed: Sep. 7, 2010 A6IP3/00 (2006.01) CI2N 5/071 (2010.01) (86). PCT No.: PCT/US 10/48OO6 CD7C 69/33 (2006.01) S371 (c)(1) (52) U.S. Cl. .......................... 514/552; 554/227; 435/375 (2), (4) Date: Apr. 12, 2012 (57) ABSTRACT Related U.S. Application Data Compounds, pharmaceutical compositions and methods of (60) Provisional application No. 61/240,014, filed on Sep. treating a disorder or disease associated with neurokinin 2 4, 2009. (NK) receptor activity. Patent Application Publication Jul. 26, 2012 Sheet 1 of 12 US 2012/O190743 A1 LU 1750 15OO 1250 OOO 750 500 250 O O 20 3O 40 min SampleName: EM2OO617 Patent Application Publication Jul. 26, 2012 Sheet 2 of 12 US 2012/O190743 A1 kixto CFUgan <tro CFUgan FIG.2 Patent Application Publication Jul. -

FROM MELANCHOLIA to DEPRESSION a HISTORY of DIAGNOSIS and TREATMENT Thomas A
1 FROM MELANCHOLIA TO DEPRESSION A HISTORY OF DIAGNOSIS AND TREATMENT Thomas A. Ban International Network for the History of Neuropsychopharmacology 2014 2 From Melancholia to Depression A History of Diagnosis and Treatment1 TABLE OF CONTENTS Introduction 2 Diagnosis and classifications of melancholia and depression 7 From Galen to Robert Burton 7 From Boissier de Sauvages to Karl Kahlbaum 8 From Emil Kraepelin to Karl Leonhard 12 From Adolf Meyer to the DSM-IV 17 Treatment of melancholia and depression 20 From opium to chlorpromazine 21 Monoamine Oxidase Inhibitors 22 Monoamine Re-uptake Inhibitors 24 Antidepressants in clinical use 26 Clinical psychopharmacology of antidepressants 30 Composite Diagnostic Evaluation of Depressive Disorders 32 The CODE System 32 CODE –DD 33 Genetics, neuropsychopharmacology and CODE-DD 36 Conclusions 37 References 37 INTRODUCTION Descriptions of what we now call melancholia or depression can be found in many ancient documents including The Old Testament, The Book of Job, and Homer's Iliad, but there is virtually 1 The text of this E-Book was prepared in 2002 for a presentation in Mexico City. The manuscript was not updated. 3 no reliable information on the frequency of “melancholia” until the mid-20th century (Kaplan and Saddock 1988). Between 1938 and 1955 several reports indicated that the prevalence of depression in the general population was below 1%. Comparing these figures, as shown in table 1, with figures in the 1960s and ‘70s reveals that even the lowest figures in the psychopharmacological era (from the 1960s) are 7 to 10 times greater than the highest figures before the introduction of antidepressant drugs (Silverman 1968). -

PHOTOSTENT-02: Porfimer Sodium Photodynamic Therapy Plus Stenting Versus Stenting Alone in Patients with Locally Advanced Or Metastatic Biliary Tract Cancer
Open access Original research ESMO Open: first published as 10.1136/esmoopen-2018-000379 on 23 July 2018. Downloaded from PHOTOSTENT-02: porfimer sodium photodynamic therapy plus stenting versus stenting alone in patients with locally advanced or metastatic biliary tract cancer Stephen P Pereira,1,2 Mark Jitlal,3 Marian Duggan,3 Emma Lawrie,3 Sandy Beare,3 Pam O'Donoghue,4 Harpreet S Wasan,5 Juan W Valle,6 John Bridgewater,7 on behalf of the PHOTOSTENT-02 investigators To cite: Pereira SP, ABSTRACT Key questions Jitlal M, Duggan M, et al. Background Endobiliary stenting is standard practice for PHOTOSTENT-02: porfimer palliation of obstructive jaundice due to biliary tract cancer sodium photodynamic therapy What is already known about this subject? (BTC). Photodynamic therapy (PDT) may also improve plus stenting versus stenting In patients with obstructive jaundice due to unre- biliary drainage and previous small studies suggested ► alone in patients with locally sectable cholangiocarcinoma, small studies have survival benefit. advanced or metastatic biliary suggested that photodynamic therapy (PDT) may Aims To assess the difference in outcome between tract cancer. ESMO Open improve biliary drainage and patient survival. 2018;3:e000379. doi:10.1136/ patients with BTC undergoing palliative stenting plus PDT esmoopen-2018-000379 versus stenting alone. What does this study add? Methods 92 patients with confirmed locally advanced ► We conducted a large randomised controlled trial or metastatic BTC, ECOG performance status 0–3 and of porfimer sodium PDT in patients with confirmed JWV and JB contributed equally. adequate biliary drainage were randomised (46 per locally advanced or metastatic biliary tract cancer. -
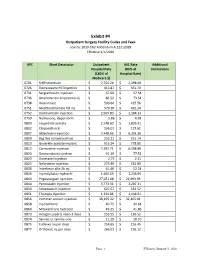
Exhibit #4 Outpatient Surgery Facility Codes and Fees Source: 2019 CN2 Addendum A.12212018 Effective 1/1/2020
Exhibit #4 Outpatient Surgery Facility Codes and Fees source: 2019 CN2 Addendum A.12212018 Effective 1/1/2020 APC Short Descriptor Outpatient ASC Rate Additional Hospital Rate (85% of Instructions (180% of Hospital Rate) Medicare $) 0701 Sr89 strontium $ 2,704.24 $ 2,298.60 0726 Dexrazoxane HCl injection $ 413.87 $ 351.79 0731 Sargramostim injection $ 67.69 $ 57.54 0736 Amphotericin b liposome inj $ 86.52 $ 73.54 0738 Rasburicase $ 500.66 $ 425.56 0751 Mechlorethamine hcl inj $ 579.10 $ 492.24 0752 Dactinomycin injection $ 2,569.80 $ 2,184.33 0759 Naltrexone, depot form $ 5.86 $ 4.98 0800 Leuprolide acetate $ 2,148.60 $ 1,826.31 0802 Etoposide oral $ 136.01 $ 115.61 0807 Aldesleukin injection $ 7,448.66 $ 6,331.36 0809 Bcg live intravesical vac $ 253.11 $ 215.14 0810 Goserelin acetate implant $ 916.24 $ 778.80 0812 Carmustine injection $ 7,292.71 $ 6,198.80 0820 Daunorubicin injection $ 91.19 $ 77.51 0823 Docetaxel injection $ 2.72 $ 2.31 0825 Nelarabine injection $ 273.99 $ 232.89 0836 Interferon alfa-2b inj $ 61.46 $ 52.24 0840 Inj melphalan hydrochl $ 1,466.65 $ 1,246.65 0843 Pegaspargase injection $ 27,051.68 $ 22,993.93 0844 Pentostatin injection $ 3,773.31 $ 3,207.31 0850 Streptozocin injection $ 627.67 $ 533.52 0851 Thiotepa injection $ 1,334.84 $ 1,134.61 0856 Porfimer sodium injection $ 38,195.22 $ 32,465.94 0858 Inj cladribine $ 40.75 $ 34.64 0864 Mitoxantrone hydrochl $ 49.25 $ 41.86 0873 Hyalgan supartz visco-3 dose $ 153.55 $ 130.52 0874 Synvisc or synvisc-one $ 21.29 $ 18.10 0875 Euflexxa inj per dose $ 254.65 $ 216.45 0877 -

Oregon Health Authority Division of Medical Assistance Programs Addendum a - Final OPPS Apcs for CY 2012 Effective October 1, 2012
Oregon Health Authority Division of Medical Assistance Programs Addendum A - Final OPPS APCs for CY 2012 Effective October 1, 2012 Relative APC Group Title SI Weight 0001 Level I Photochemotherapy S 0.5042 0002 Fine Needle Biopsy/Aspiration T 1.6115 0003 Bone Marrow Biopsy/Aspiration T 3.5702 0004 Level I Needle Biopsy/ Aspiration Except Bone Marrow T 4.5746 0005 Level II Needle Biopsy/Aspiration Except Bone Marrow T 8.1566 0006 Level I Incision & Drainage T 1.4206 0007 Level II Incision & Drainage T 13.1250 0008 Level III Incision and Drainage T 20.5648 0012 Level I Debridement & Destruction T 0.3878 0013 Level II Debridement & Destruction T 0.8785 0015 Level III Debridement & Destruction T 1.4989 0016 Level IV Debridement & Destruction T 2.7592 0017 Level V Debridement & Destruction T 21.6661 0019 Level I Excision/ Biopsy T 4.4238 0020 Level II Excision/ Biopsy T 8.2746 0021 Level III Excision/ Biopsy T 17.0074 0022 Level IV Excision/ Biopsy T 23.2662 0028 Level I Breast Surgery T 25.5054 0029 Level II Breast Surgery T 33.4070 0030 Level III Breast Surgery T 44.8999 0031 Smoking Cessation Services X 0.2997 0034 Mental Health Services Composite S 2.7295 0035 Vascular Puncture and Minor Diagnostic Procedures X 0.2691 0037 Level IV Needle Biopsy/Aspiration Except Bone Marrow T 15.3499 0039 Level I Implantation of Neurostimulator Generator S 216.7598 0040 Level I Implantation/Revision/Replacement of Neurostimulator Electrodes S 63.7616 0041 Level I Arthroscopy T 29.6568 0042 Level II Arthroscopy T 57.0137 0045 Bone/Joint Manipulation Under -

Original New Drug Applications
New Drugs Reviewed by CPG January 23, 2017 (Original New Drug Applications: FDA) Generic Name Trade Name Indication(s) CPG Action Immune globulin Cuvitru Biologic and In accordance with subcutaneous Immunological the SCA [human] 20% solution Agents/Immune Globulins/ Immune Globulin (Human) subcutaneous. Indicated as replacement for primary humoral immunodeficiency in adult and pediatric patients age two and older. eteplirsen Exondys 51 Central Nervous System In accordance with Agents/Antisense the SCA Oligonucleotides. Treatment of patients who have a confirmed mutation of the dystrophin gene amenable to exon 51 skipping. First drug approved for reatment of patients with Duchenne muscular dystrophy. levonorgestrel- Kyleena Endocrine and May prescribe releasing intrauterine Metabolic Agents/sex system 19.5 mg homones/contraceptive Hormones. Prevention of pregnancy for up to five years. **Phentermine Lomaira Central Nervous System In accordance with hydrochloride 8 mg Agents/ the SCA anorexiants/sympathomi metic anorexiants. Short term use weight reduction in adults with **(new formulation at an initial BMI of 30 or lower dosage) more or 27 with at least one weight-related condition. 1 New Drugs January 2017 canaglifozin/ Invokamet XR Endocrine and May prescribe metformin HCL Metabolic Agents/ extended-release antidiabetic agents/antidiabetic combination products. Treatment of adults with type 2 diabetes as an adjunct to diet and exercise. Adalimumab-atto Amjevita Biologic and In accordance with Immunological Agents/ the SCA Immunologic Agents/Immunomodulat ors/Tumor necrosis Factor-Alpha Blockers. Indicated for treatment of adults with: rheumatoid arthritis, psoriatic arthritis,ankylosing spondylitis, Crohn disease, ulcerative colitis, and plaque psoriasis. Also indicated for juvenile idiopathic arthritis in pts age 4 years and older. -

Patent Application Publication ( 10 ) Pub . No . : US 2019 / 0192440 A1
US 20190192440A1 (19 ) United States (12 ) Patent Application Publication ( 10) Pub . No. : US 2019 /0192440 A1 LI (43 ) Pub . Date : Jun . 27 , 2019 ( 54 ) ORAL DRUG DOSAGE FORM COMPRISING Publication Classification DRUG IN THE FORM OF NANOPARTICLES (51 ) Int . CI. A61K 9 / 20 (2006 .01 ) ( 71 ) Applicant: Triastek , Inc. , Nanjing ( CN ) A61K 9 /00 ( 2006 . 01) A61K 31/ 192 ( 2006 .01 ) (72 ) Inventor : Xiaoling LI , Dublin , CA (US ) A61K 9 / 24 ( 2006 .01 ) ( 52 ) U . S . CI. ( 21 ) Appl. No. : 16 /289 ,499 CPC . .. .. A61K 9 /2031 (2013 . 01 ) ; A61K 9 /0065 ( 22 ) Filed : Feb . 28 , 2019 (2013 .01 ) ; A61K 9 / 209 ( 2013 .01 ) ; A61K 9 /2027 ( 2013 .01 ) ; A61K 31/ 192 ( 2013. 01 ) ; Related U . S . Application Data A61K 9 /2072 ( 2013 .01 ) (63 ) Continuation of application No. 16 /028 ,305 , filed on Jul. 5 , 2018 , now Pat . No . 10 , 258 ,575 , which is a (57 ) ABSTRACT continuation of application No . 15 / 173 ,596 , filed on The present disclosure provides a stable solid pharmaceuti Jun . 3 , 2016 . cal dosage form for oral administration . The dosage form (60 ) Provisional application No . 62 /313 ,092 , filed on Mar. includes a substrate that forms at least one compartment and 24 , 2016 , provisional application No . 62 / 296 , 087 , a drug content loaded into the compartment. The dosage filed on Feb . 17 , 2016 , provisional application No . form is so designed that the active pharmaceutical ingredient 62 / 170, 645 , filed on Jun . 3 , 2015 . of the drug content is released in a controlled manner. Patent Application Publication Jun . 27 , 2019 Sheet 1 of 20 US 2019 /0192440 A1 FIG . -

Prevalence and Safety of Off-Label Use of Chemotherapeutic Agents in Older Patients with Breast Cancer: Estimates from SEER-Medicare Data
Supplemental online content for: Prevalence and Safety of Off-Label Use of Chemotherapeutic Agents in Older Patients With Breast Cancer: Estimates From SEER-Medicare Data Anne A. Eaton, MS; Camelia S. Sima, MD, MS; and Katherine S. Panageas, DrPH J Natl Compr Canc Netw 2016;14(1):57–65 • eAppendix 1: J-Codes Representing Intravenous Chemotherapy • eAppendix 2: Established Sequential Adjuvant Chemotherapy Regimens for Breast Cancer • eTable 1: Patient Characteristics © JNCCN—Journal of the National Comprehensive Cancer Network | Volume 14 Number 1 | January 2016 Eaton et al - 1 eAppendix 1: J-Codes Representing Intravenous Chemotherapy J-Code Agent J-Code Agent J9000 Injection, doxorubicin HCl, 10 mg J9165 Injection, diethylstilbestrol diphosphate, 250 J9001 Injection, doxorubicin HCl, all lipid mg formulations, 10 mg J9170 Injection, docetaxel, 20 mg J9010 Injection, alemtuzumab, 10 mg J9171 Injection, docetaxel, 1 mg J9015 Injection, aldesleukin, per single use vial J9175 Injection, Elliotts’ B solution, 1 ml J9017 Injection, arsenic trioxide, 1 mg J9178 Injection, epirubicin HCl, 2 mg J9020 Injection, asparaginase, 10,000 units J9179 Injection, eribulin mesylate, 0.1 mg J9025 Injection, azacitidine, 1 mg J9180 Epirubicin HCl, 50 mg J9027 Injection, clofarabine, 1 mg J9181 Injection, etoposide, 10 mg J9031 BCG (intravesical) per instillation J9182 Etoposide, 100 mg J9033 Injection, bendamustine HCl, 1 mg J9185 Injection, fludarabine phosphate, 50 mg J9035 Injection, bevacizumab, 10 mg J9190 Injection, fluorouracil, 500 mg J9040 Injection, -

Standard Oncology Criteria C16154-A
Prior Authorization Criteria Standard Oncology Criteria Policy Number: C16154-A CRITERIA EFFECTIVE DATES: ORIGINAL EFFECTIVE DATE LAST REVIEWED DATE NEXT REVIEW DATE DUE BEFORE 03/2016 12/2/2020 1/26/2022 HCPCS CODING TYPE OF CRITERIA LAST P&T APPROVAL/VERSION N/A RxPA Q1 2021 20210127C16154-A PRODUCTS AFFECTED: See dosage forms DRUG CLASS: Antineoplastic ROUTE OF ADMINISTRATION: Variable per drug PLACE OF SERVICE: Retail Pharmacy, Specialty Pharmacy, Buy and Bill- please refer to specialty pharmacy list by drug AVAILABLE DOSAGE FORMS: Abraxane (paclitaxel protein-bound) Cabometyx (cabozantinib) Erwinaze (asparaginase) Actimmune (interferon gamma-1b) Calquence (acalbrutinib) Erwinia (chrysantemi) Adriamycin (doxorubicin) Campath (alemtuzumab) Ethyol (amifostine) Adrucil (fluorouracil) Camptosar (irinotecan) Etopophos (etoposide phosphate) Afinitor (everolimus) Caprelsa (vandetanib) Evomela (melphalan) Alecensa (alectinib) Casodex (bicalutamide) Fareston (toremifene) Alimta (pemetrexed disodium) Cerubidine (danorubicin) Farydak (panbinostat) Aliqopa (copanlisib) Clolar (clofarabine) Faslodex (fulvestrant) Alkeran (melphalan) Cometriq (cabozantinib) Femara (letrozole) Alunbrig (brigatinib) Copiktra (duvelisib) Firmagon (degarelix) Arimidex (anastrozole) Cosmegen (dactinomycin) Floxuridine Aromasin (exemestane) Cotellic (cobimetinib) Fludara (fludarbine) Arranon (nelarabine) Cyramza (ramucirumab) Folotyn (pralatrexate) Arzerra (ofatumumab) Cytosar-U (cytarabine) Fusilev (levoleucovorin) Asparlas (calaspargase pegol-mknl Cytoxan (cyclophosphamide) -

Lee County Environmental Health
Lee County Environmental Health LICENSING OF TANNING FACILITIES CHAPTER 64E-17 The 1991 Florida Legislature passed a law which requires the licensing and monitoring of tanning facilities. The Florida Department of Health, through its County Health Departments, is responsible for licensing and monitoring these facilities for compliance with the law. Further information and downloads can be found at http://lee.floridahealth.gov/programs-and- services/environmental-health/tanning/index.html The following documents must be provided to the local Health Department prior to issuance of a tanning facility license. 1. Application for Tanning Facility License 2. Tanning Facility Equipment Information 3. Site-Plan (Review checklist attached; Site-Plan required with application). 4. Approved Tanning Certification (a list of approved training is provided and available on the DOH website) 5. Applicant Certification Form 6. Copy of Facility’s Operating and Safety Procedures 7. Certificate of insurance that provides liability insurance including limits of liability 8. Check in the amount due shown on the application or invoice should be made payable to: Florida Department of Health. Payment is due at time of application Please be reminded that the operation of your tanning facility without a current state license is a violation of Florida Administrative Code and that you are responsible for renewing your license annually as notified by this department. The deadline for license renewal is October 1st each year. If you have any questions regarding this matter, please do not hesitate to contact the Florida Department of Health in Lee County at 239-690-2100. 2295 Victoria Avenue, #206 Fort Myers, FL 33901 Phone: 239-690-2100 Fax: 239-690-2101 License Number HEALTH STATE OF FLORIDA DEPARTMENT OF HEALTH APPLICATION FOR TANNING FACILITY LICENSE AUTHORITY: SECTION 381 .89, Florida Statutes INSTRUCTIONS 1. -

PHOTOFRIN® Sterile Porfimer Sodium for Injection For
PHOTOFRIN® Sterile Porfimer Sodium for Injection For Intravenous Use Antineoplastic Photosensitizing Agent Concordia Laboratories Inc. DATE OF PREPARATION: 5 Canewood Industrial Park October 27, 2014 St. Michael, St. Michael, Barbados BB11005 CONTROL # 178591 PHOTOFRIN® Product Monograph PRODUCT MONOGRAPH PHOTOFRIN® Sterile Porfimer Sodium for Injection For Intravenous Use ANTINEOPLASTIC PHOTOSENSITIZING AGENT CAUTION: PHOTOFRIN® IS AN INJECTABLE PHOTOSENSITIZING DRUG FOR USE IN PHOTODYNAMIC THERAPY (PDT) FOR TREATMENT OF CANCER AND PRE-MALIGNANT CONDITIONS (E.G., HIGH-GRADE DYSPLASIA IN BARRETT'S ESOPHAGUS). PHOTODYNAMIC THERAPY IS A PHOTOCHEMICAL PROCESS REQUIRING SPECIFIC LASERS AND FIBER OPTICS. PHOTODYNAMIC THERAPY WITH PHOTOFRIN® SHOULD ONLY BE APPLIED BY PHYSICIANS TRAINED IN THE ENDOSCOPIC USE OF PDT WITH PHOTOFRIN® AND ONLY IN THOSE FACILITIES PROPERLY EQUIPPED FOR THE PROCEDURE. PHOTOFRIN® MAY CAUSE RESIDUAL PHOTOSENSITIVITY FOR 30 DAYS OR MORE RESULTING IN ERYTHEMA AND BLISTERING OF THE SKIN WHEN IT IS EXPOSED TO DIRECT SUNLIGHT OR BRIGHTLY FOCUSED INDOOR LIGHT (E.G., FROM EXAMINATION 2 PHOTOFRIN® Product Monograph LAMPS, OPERATING ROOM LAMPS, FLOODLIGHTS, HALOGEN LAMPS, ETC.). ACTION & CLINICAL PHARMACOLOGY Pharmacodynamics The cytotoxic and antitumor actions of PHOTOFRIN® (porfimer sodium) are light and oxygen dependent. Photodynamic therapy (PDT) with PHOTOFRIN® is a 2-stage process. The first stage is the intravenous injection of PHOTOFRIN®. Clearance from a variety of tissues occurs over 40-72 hours; but tumor, skin, and organs of the reticuloendothelial system (including liver and spleen) retain PHOTOFRIN® for a longer period. Illumination with 630 nm wavelength laser light constitutes the second and final stage of therapy. Tumor selectivity in treatment occurs through a combination of selective retention of PHOTOFRIN® and selective delivery of light. -

9458 Federal Register / Vol
9458 Federal Register / Vol. 71, No. 37 / Friday, February 24, 2006 / Rules and Regulations paragraph (b) of this section. Other parameter monitoring plan for the It also revised Medicare Part B acceptable monitoring approaches affected unit, as specified in § 60.334(g). payment and related policies regarding: include periodic testing approved by * * * * * Physician work, practice expense and EPA or the State or local permitting [FR Doc. 06–1743 Filed 2–23–06; 8:45 am] malpractice relative value units (RVUs); authority or continuous parameter BILLING CODE 6560–50–P Medicare telehealth services; multiple monitoring as described in paragraph (f) diagnostic imaging procedures; covered of this section. outpatient drugs and biologicals; supplemental payments to Federally (f) The owner or operator of a new DEPARTMENT OF HEALTH AND Qualified Health Centers (FQHCs); renal turbine that commences construction HUMAN SERVICES after July 8, 2004, which does not use dialysis services; coverage for glaucoma screening services; National Coverage water or steam injection to control NOX Centers for Medicare & Medicaid emissions may, but is not required to, Services Decision (NCD) timeframes; and perform continuous parameter physician referrals for nuclear medicine monitoring as follows: 42 CFR Parts 405, 410, 411, 413, 414, services and supplies to health care 424 and 426 entities with which physicians have * * * * * financial relationships. (2) For any lean premix stationary [CMS–1502–F2 and CMS–1325–F] In addition, the rule finalized the combustion turbine, the owner or RIN 0938–AN84 and 098–AN58 interim RVUs for CY 2005 and issued operator shall continuously monitor the interim RVUs for new and revised appropriate parameters to determine Medicare Program; Revisions to procedure codes for CY 2006.