Applying a General Systems Theory Framework in Mental Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Hellenic Culture Centre Athens & Santorini Island, Greece
ERASMUS STUDENT PLACEMENTS THE HELLENIC CULTURE CENTRE ATHENS & SANTORINI ISLAND, GREECE WHO/ WHERE: A. The Hellenic Culture Centre www.hcc.edu.gr , founded in 1995, is one of the first non formal education institutions that offered Greek as a foreign/second language courses. It has an expertise in Language Teacher Training programmes. The aims of the institution are to promote language learning and language teaching and to contribute to adult education and intercultural education methodology. Has been involved in different national and EU projects on intercultural education, teacher training, cultural exchanges, e-learning. The Hellenic Culture Centre offers four internship posts for Erasmus students, for its offices in Athens and Santorini island, Greece: 1. Marketing coordinator To coordinate and implement a Marketing programme for new students recruitment, especially through the Internet, to work on the website, to upload materials and create newsletters, to translate texts into her/ his mother tongue 2. EU funding assistant To assist in developing proposals for EU funded projects under the Life Long Learning Programme, and to assist in implement projects that are on the way (monitor printing and production of materials, monitor on time implementation of events, monitor on time delivery of products/ deliverables, monitor expenses according to budget), to evaluate proposals and provide feedback. 3. E-learning expert To develop the e-learning platform of HCC. To coordinate the social networks of HCC. To create didactic materials for e-learning. To work on e-learning projects and develop new projects 4. Cultural Officer To develop a cultural programme in Athens & in Santorini complementary to the language programme, to develop training materials for cultural presentations (in English), to accompany students to cultural visits. -
NEW EOT-English:Layout 1
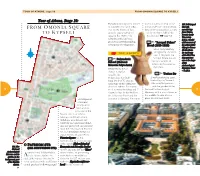
TOUR OF ATHENS, stage 10 FROM OMONIA SQUARE TO KYPSELI Tour of Athens, Stage 10: Papadiamantis Square), former- umental staircases lead to the 107. Bell-shaped FROM MONIA QUARE ly a garden city (with villas, Ionian style four-column propy- idol with O S two-storey blocks of flats, laea of the ground floor, a copy movable legs TO K YPSELI densely vegetated) devel- of the northern hall of the from Thebes, oped in the 1920’s - the Erechteion ( page 13). Boeotia (early 7th century suburban style has been B.C.), a model preserved notwithstanding 1.2 ¢ “Acropol Palace” of the mascot of subsequent development. Hotel (1925-1926) the Athens 2004 Olympic Games A five-story building (In the photo designed by the archi- THE SIGHTS: an exact copy tect I. Mayiasis, the of the idol. You may purchase 1.1 ¢Polytechnic Acropol Palace is a dis- tinctive example of one at the shops School (National Athens Art Nouveau ar- of the Metsovio Polytechnic) Archaeological chitecture. Designed by the ar- Resources Fund – T.A.P.). chitect L. Kaftan - 1.3 tzoglou, the ¢Tositsa Str Polytechnic was built A wide pedestrian zone, from 1861-1876. It is an flanked by the National archetype of the urban tra- Metsovio Polytechnic dition of Athens. It compris- and the garden of the 72 es of a central building and T- National Archaeological 73 shaped wings facing Patision Museum, with a row of trees in Str. It has two floors and the the middle, Tositsa Str is a development, entrance is elevated. Two mon- place to relax and stroll. -

So, Here You Are in Athens
So, here you are in Athens! New city… new people… new places… a new way of living! Have no anxiety about this completely new way of living! Here is a simple guide to help you turn your residence in Athens into an unforgetable experience! Description of the Guide The following guide refers to clubs, bars, cafes, restaurants in Athens which are recommended because of their decoration, environment, prices or the different experiences they offer! Where it is possible, there is an estimation about the cost per person or a reference to the actual prices. Don’t worry…there are recommendations for every mood, budget or preference! Clubbing Guide Dance Stages : From progressive to techno BIOS BASEMENT _ Pireos Str. 8, Athens, tel. : 210 3425335 YES _ Mavrimichali & Gravias Str. 10, Pireaus, tel.: 6946 760798. Open only on Friday and Saturday. YOU (Playback by Pierro’’s) _ Dekeleon Str. 26, tel.: 210 3452220, 6947 745816 Massive Clubs BAROC’ E _ Stadiou square 5 & Agras Str., Kallimarmaro, tel.: 210 7565007 – 8. Freestyle and mainstream music. BIANCO NERO _ Vafeiochoriou Str. 65 (after Evelpidon), Polygono, tel.: 210 6465326 CAMEL CLUB _ Erakleidon Str. 74, Thiseio, tel.: 210 3476847, www.camelclub.gr DEXX CLUB _ Alexandras Avenue 87 & Drosi Str. 1 , Gyzi, tel. : 210 6465290 EGOIST _ Panepistimiou Str. 10, Athens, tel.: 210 3638201. Bottle of whisky €100, drink €10 HARD ROCK CAFÉ _ Fillelinon Str. 18, tel.: 210 3252742. Rock and mainstream music. American kitchen. The first shop of the famous brand in Athens. Open from 12 a.m. to very late every night. -

THE RUSSIAN ORTHODOX CHURCH Department for External Church Relations
THE RUSSIAN ORTHODOX CHURCH Department for External Church Relations List of Orthodox Church of Greece dioceses undesirable to be visited by pilgrims of the Russian Orthodox Church In response to inquiries coming to the Department for External Church Relations of the Moscow Patriarchate, the department clarifies that, in keeping with the Holy Synod Statement of October 17, 2019 (Minutes No. 125), no blessing is given upon the Russian Orthodox Church’s pilgrims’ visits to the following dioceses of the Orthodox Church of Greece, whose ruling bishops have entered in church communion with the Ukrainian schismatics: 1. Metropolis of Athens headed by Archbishop Ieronimus II of Athens and All Greece, under whose direct authority are the following districts of the Greek capital city: the center of Athens, Ano Petralona, Koukaki, Kato Petralona, Tavros, Keramikos, Votanikos. Akadimia Platonas, Kolokinthous, Skouze, Aharnes, Patisia, Sepolia, Kato Patisia, Ano Patisia, Galanchi, Kypseli, Kuzi, Ambelokipi, Goudi, Zografou, Pankration, Ilissos, Agios Dimitrios, Ilioupoli, Kallithea, Moschato, Ginzifies, Papagou, Psychiko, Chalandri, Vrilissia, Cholargos, Agia Paraskevi, Kato Chalandri. The major churches in the Archdiocese of Athens are the Cathedral of the Annunciation, the Church of St. Dionysius the Areopagite, and the Church of the Holy Protomartyr Panteleimon Acharnai. These restrictions do not involve dioceses that include suburban parts and districts of Athens and the whole region of Attica. These are the Metropolises of Piraeus, Mesogeia, Ilion, Peristeri, Kythira, New Smyrna, Kifissia, Kessariani, Glyfada, Nicaea, Megara, Hydra, and Philadelphia. 2. Diocese of Langada; ruling bishop – Metropolitan Ioannis of Langada; 3. Diocese of Veria; ruling bishop – Metropolitan Panteleimon of Veria, Naoussa and Campania; 4. -
Erasmus Experience Is So Much More Than Just an Exchange Program
Erasmus experience is so much more than just an exchange program. It’s a lifestyle, it’s a party, it’s a celebration, it’s a Hollywood movie and you are starring!!! And this is a guide to help you explore the setting: Athens!!!! RELEASE DATE: June 2015 AllAboutAthensT.H.E.N.S. We start with a little bit of history…so, what do you know about Athens? Long before it became a great city and the birthplace of democracy, the area of Athens must have been a beautiful place- otherwise it would be impossible to explain why the most powerful ancient gods duelled to give their name to the city.In the end it was Poseidon, the god of the sea, and Athena, the goddess of wisdom, who reached the final round. Zeus, out of whose head Athena was born, in order to avoid a violent encounter between the two gods, declared that each should make an offer to the new city and the city would be named after the god whose offer would be accepted by the citizens. Poseidon, who was Zeus' brother, came first and struck the rock of the Acropolis, opening a spring of water. This meant that Poseidon was offering the new city success at sea. Then Athena came forward and dropped a seed to the ground that immediately turned into an olive tree. This was meant to indicate that the goddess was offering the new city the peace and wisdom, which the citizens accepted and named their city Athens, while the owl, the bird associated with Athena and signified wisdom, became the sacred animal of the Athenians Athens Step by Step So now that you know this story, if you want to discover Athens, you will have get active! We have prepared a nice walk for you that you can take more than once both with your national or international friends!! Acropolis, Makrygianni, Thissio • You can start your walk by getting off at the Acropolis metro station (red line). -

Perceived and Lived Space in the Modern City. a Case Study for Akadimia Platonos Neighborhood, Athens, Greece
European Journal of Geography Volume 11, Issue 4, pp. 064 - 092 Article Info: Accepted: 16/12/2020 Corresponding Author: *[email protected] https://doi.org/10.48088/ejg.g.lam.11.4.64.92 Special Issue: “Selected Papers from 12th International Conference of the Hellenic Geographical Society (ICHGS): Innovative Geographies II, 2019” Perceived and lived space in the modern city. A case study for Akadimia Platonos neighborhood, Athens, Greece Georgios D. LAMPROPOULOS1*, 1 National Technical University of Athens, Greece Yorgos N. PHOTIS1, Maria PIGAKI1 Keywords: Abstract spatial practices, The main objective of this paper is to perform a spatial analysis of everyday representational life experiences by enriching a socio-spatial approach within the boundaries spaces, of Akadimia Platonos neighborhood, in the city of Athens. It investigates the perceived space, convergences and divergences that are observed between two different lived space, space syntax, manifestations of space, as they have been approached through Henri Akadimia Platonos, Lefebvre’s social theory of space, the perceived space and the lived space. ICHGS-2019 Mainly, the designed-geometric space, enhanced with all those relationships programmed for social reproduction, creates an experience for its users. Does this lived experience, that is expected to be experienced, actually correspond to reality? In the methodological framework proposed, perceived space (as spatial practices) is examined through the space syntax analysis of the study area, while lived space (as representational spaces) is accessed through questionnaire interviews, which examine the space perception of residents, workers, visitors, passers-by, using it. The publication of the European Journal of Geography (EJG) is based on the European Association of Geographers’ goal to make European Geography a worldwide reference and standard. -

Pocket Athens 3 Preview
ATHENS TOP SIGHTS • LOCAL LIFE • MADE EASY Alexis Averbuck 00--title-contents-pk-ath3.inddtitle-contents-pk-ath3.indd 1 99/10/2015/10/2015 111:09:261:09:26 AM In This Book 16 Need to Know 17 18 Neighbourhoods 19 Before You Go Arriving in Athens Getting Around National Archaeo- logical Museum & Ancient Agora, Athens Exarhia (p000) Need to Your Daily Budget Most visitors arrive at Athens’ Eleftherios Athens has an extensive and inexpensive Monastiraki & Discover the treasures Venizelos International Airport at Spata, integrated public-transport network of buses, Psyrri (p000) Budget less than €100 27km east of the city centre. Most ferries and metro, trolleybuses and trams. Pick up maps at the world's foremost Know Neighbourhoods The ancient Athenian X Dorm beds €25, pension doubles from €65 cruises arrive at the port of Piraeus. and timetables at the EOT tourist office, collection of Greek art civic centre spills into Benaki Museum & QuickStart (p165) the airport or online at www.oasa.gr. and antiquities, then X Eat at souvlaki shops and tavernas the modern city's For more information, A From Eleftherios Venizelos soak up the vibe in Kolonaki (p000) The metro (www.amel.gr) is the best way central shopping hub – see Survival Guide (p157). X Save euros in the shoulder or low season International Airport Consistently fashionable to get around town. Conveniently, all public E# National bohemian Exarhia. a heady mix of eclectic Archaeological E and loaded with popular Destination Best Transport transport operates under the same ticketing shops, restaurants and Top Sights Currency Midrange €100–200 Museum boutiques, cafes and system. -
Bank of Subsistence Goods Assistance
Bank of Subsistence Goods Assistance 1. Home of Elderly Welfare Holy Church of Agios Spyridon 2. “The White Cottage Day Care” Nursery 3. Ilion Special Lyceum 4. Athens Special High School and Special Lyceum 5. 1st and 2nd Keratsini Primary School 6. 2nd and 8th Keratsini Kindergarten 7. Tumulus Marathon Primary School 8. Action Aid of Greece 9. Charities of the Parish of St. Spyridon 10. The Smile of the Child (Kareas) 11. Piraeus Society for the Protection of Children 12. Youth Training Centre Taurus 13. Child Protection Society “Smyrna St. Polycarp” 14. Open Therapeutic Community “Diadromi” 15. Foundation for Social Responsibility Municipality Zografou “The House of Solidarity” 16. Kapandriti.Community Elderly Club 17. Greek-Arab Association for Taking Care of the Child 18. National School of Public Health / Sociology Section 19. Orphanage “St. Nektarios” (Chania) 20. United Nations High Commissioner for Refugees 21. Hellenic Committee of Cooperation with UNICEF 22. Amnesty International / Greek Section 23. Ukrainian Diaspora Community in Greece “Land of the Stork” 24. Hospital, Orphanage, Nursing Home Guinea-Bissau 25. Social Reintegration of Excluded Individuals / Barka Foundation (Switzerland) 26. Psychogiriatriki Company “Nestor” 27. Hellenic Association of People with Thalassemia 28. Zanzibar Poorhouse and Orphanage 29. Kenya Youth Training 30. Large Families Support “Theofilos” 31. Attica Earthquake Victims 32. Achaea Flood victims 33. Georgia Elderly Homogeneous 34. Romvis Charities Fund 35. Milina Holy Temple of the Dormition of the Virgin Mary (Poorhouse) 36. Rethymno 4th High School 37. Association of Large Families Kalavryton 38. Paros Poor Families 39. Fire Victims (Ilia, Messinia, Arcadia, Laconia) 40. Association of Rehabilitation Addicted People “The Return” 41. -

List of Bank Branches by Branch Name 31/12/2014
LIST OF BANK BRANCHES BY BRANCH NAME 31/12/2014 PIRAEUS BANK S.A. BRANCH NAMEHEBIC AREA ADDRESS TELEPHONE NUMBER / FAX 1866 SQUARE, CHANIA0172758 CHANIA 70, Chatzimichali Giannari str., 731 35 CHANIA tel.: 2821029100, fax: 2821050710 25TH AVGOUSTOU, HERAKLIO0172751 HERAKLEIO 39, 25th Avgoustou str., 712 02 HERAKLEIO tel.: 2810247610, fax: 2810228324 3RD SEPTEMVRIOU, OMONIA 0172039 ATHENS 28, 3rd Septemvriou & Kapodistriou str., 104 32 ATHENS BRANCH tel.: 2105205100, fax: 2105235138 62 MARTIRON HERAKLIOU0172761 HERAKLEIO 97, 62 Martiron Ave. & 1, Dionysiou Fragiadaki str., 713 04 HERAKLEIO tel.: 2810264330, fax: 2810255997 ABELONAS0171393 AMPELONAS 1, Goltsiou & 5, Thermopylon str., 404 00 AMPELONAS tel.: 2492306000, fax: 2492031402 ACHARNON0172058 ATHENS 421, Acharnon str., 111 43 ATHENS tel.: 2102588070, fax: 2102520490 ACHARNON STR.0171592 ATHENS 205, Acharnon & Niovis str.s., 104 46 ATHENS tel.: 2166008310, fax: 2168003817 AEGINA BRANCH0172124 AEGINA Dimokratias Coastal Ave. & Leonardou Lada str., 180 10 AEGINA tel.: 2297029890, fax: 2297028882 AG. ACHILLIOU0171563 LARISSA 146, El. Venizelou str., 412 22 LARISSA tel.: 2416000160, fax: 2416007111 AG. ANTONIOU, PERISTERI0172048 PERISTERI 33, Ethnarchou Makariou str., 121 31 PERISTERI tel.: 2105783020, fax: 2105773224 AG. DIMITRIOS0171555 AGIOS DIMITRIOS 266, Vouliagmenis Ave., 173 43 AGIOS DIMITRIOS tel.: 2160005020, fax: 2109765714 AG. DIMITRIOU0172085 AGIOS DIMITRIOS 173, Ag. Dimitriou Ave., 173 43 AGIOS DIMITRIOS tel.: 2109758170, fax: 2109764036 AG. DIMITRIOU, THESSALONIKI0172203 THESSALONIKI 77, Ag. Dimitriou str., 546 33 THESSALONIKI tel.: 2310254860, fax: 2310223843 AG. IOANNI RENTI SQ. BRANCH0172136 AG. I. RENTIS 4, Konstantinou Palaiologou str., Ag. I. Renti sq., 182 33 AG. I. RENTIS tel.: 2104838120, fax: 2104832389 AG. IOANNOU, AG. PARASKEVI0172010 AGIA PARASKEVI 40, Ag. Ioannou str., 153 42 AGIA PARASKEVI tel.: 2106085800, fax: 2106011128 AG. -

Refugee Crisis Are Not Immediately Visible
Living for Years in a Transitory Home A Case Study of Refugees in Towns Athens, Greece Katerina Voutsina, DA, and SA* September 2019 Contents Location ..................................................................................................................................................... 3 Introduction ............................................................................................................................................... 4 Refugee and Host Experiences in Athens ............................................................................................. 5 Conclusion............................................................................................................................................... 13 References ............................................................................................................................................... 13 Appendix A: Methods ............................................................................................................................. 15 Appendix B: Background on Refugees in Greece .............................................................................. 16 Appendix C: Background on Refugees in Athens .............................................................................. 17 About the RIT Project ............................................................................................................................. 20 About the Authors ................................................................................................................................. -

Case of Athens, Greece Social and Spatial Segregation of Municipality of Athens and Possible Solutions
“Trapped” in a new future: Case of Athens, Greece Social and spatial segregation of municipality of Athens and possible solutions Aliona Cerednicenco Urban studies Masters (Two-Years) 30 credits Supervisor Defne Kadioglu Spring Semester 2020 Abstract The mass displacement of people is a global phenomenon, inherent in human nature and the need for survival. Over the last 30 years, Greece became a destination country for different populations. Although the last wave of displacement people, starting from 2015, found Greece in an unstable economic situation due to the economic crisis. Since 2015, Greece has been facing the two types of crises: economic and refugee. The refugee crisis found Greece, like many other EU countries, unprepared for the number of people that they received. From that perspective Greece refugee crisis can be viewed as a crisis of legitimacy and strategies. During the last five years, Greece made significant steps in the regulation of the refugee situation, especially after the EU-Turkey agreement in March 2016, when Greece officially became a country of destination from a transit country. However, the laws and ministerial decisions instead of decreasing the residential segregation led to an increase of social segregation. This paradox can be observed in the case of the Athenian municipality. This paradox defined the starting point of this thesis and aimed for the investigation of spatial and social segregation in the center of Athens. To study this theme qualitative data were collected for analysis, including, semi-structured interviews, analysis of official documents and observation. The funding of this thesis illustrates that Greece never lost its status as a transit country. -

Athens Constituted the Cradle of Western Civilisation
GREECE thens, having been inhabited since the Neolithic age, is considered Europe’s historical capital. During its long, Aeverlasting and fascinating history the city reached its zenith in the 5th century B.C (the “Golden Age of Pericles”), when its values and civilisation acquired a universal significance and glory. Political thought, theatre, the arts, philosophy, science, architecture, among other forms of intellectual thought, reached an epic acme, in a period of intellectual consummation unique in world history. Therefore, Athens constituted the cradle of western civilisation. A host of Greek words and ideas, such as democracy, harmony, music, mathematics, art, gastronomy, architecture, logic, Eros, eu- phoria and many others, enriched a multitude of lan- guages, and inspired civilisations. Over the years, a multitude of conque - rors occupied the city and erected splendid monuments of great signifi- cance, thus creating a rare historical palimpsest. Driven by the echo of its classical past, in 1834 the city became the capital of the modern Greek state. During the two centuries that elapsed however, it developed into an attractive, modern metropolis with unrivalled charm and great interest. Today, it offers visitors a unique experience. A “journey” in its 6,000-year history, including the chance to see renowned monu- ments and masterpieces of art of the antiquity and the Middle Ages, and the architectural heritage of the 19th and 20th cen- turies. You get an uplifting, embracing feeling in the brilliant light of the attic sky, surveying the charming landscape in the environs of the city (the indented coastline, beaches and mountains), and enjoying the modern infrastructure of the city and unique verve of the Athenians.