Petitions Committee Public Document Pack
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PEMBROKESHIRE © Lonelyplanetpublications Biggest Megalithicmonumentinwales
© Lonely Planet Publications 162 lonelyplanet.com PEMBROKESHIRE COAST NATIONAL PARK •• Information 163 porpoises and whales are frequently spotted PEMBROKESHIRE COAST in coastal waters. Pembrokeshire The park is also a focus for activities, from NATIONAL PARK hiking and bird-watching to high-adrenaline sports such as surfing, coasteering, sea kayak- The Pembrokeshire Coast National Park (Parc ing and rock climbing. Cenedlaethol Arfordir Sir Benfro), established in 1952, takes in almost the entire coast of INFORMATION Like a little corner of California transplanted to Wales, Pembrokeshire is where the west Pembrokeshire and its offshore islands, as There are three national park visitor centres – meets the sea in a welter of surf and golden sand, a scenic extravaganza of spectacular sea well as the moorland hills of Mynydd Preseli in Tenby, St David’s and Newport – and a cliffs, seal-haunted islands and beautiful beaches. in the north. Its many attractions include a dozen tourist offices scattered across Pembro- scenic coastline of rugged cliffs with fantas- keshire. Pick up a copy of Coast to Coast (on- Among the top-three sunniest places in the UK, this wave-lashed western promontory is tically folded rock formations interspersed line at www.visitpembrokeshirecoast.com), one of the most popular holiday destinations in the country. Traditional bucket-and-spade with some of the best beaches in Wales, and the park’s free annual newspaper, which has seaside resorts like Tenby and Broad Haven alternate with picturesque harbour villages a profusion of wildlife – Pembrokeshire’s lots of information on park attractions, a cal- sea cliffs and islands support huge breeding endar of events and details of park-organised such as Solva and Porthgain, interspersed with long stretches of remote, roadless coastline populations of sea birds, while seals, dolphins, activities, including guided walks, themed frequented only by walkers and wildlife. -

Contents Urdd Gobaith Cymru Annual Report 2015–16 3
URDD ANNUAL 3 GOBAITH REPORT CYMRU 2015–16 CONTENTS This Year in Brief 4–5 Chief Executive’s Report 6 Chair’s Report 7 Case Study 1 – Megan Elias 8–9 Community Activities 10 Communications Department 10 Eisteddfod and the Arts Department 11 Sports Department 11 Case Study 2 – 12–13 Outdoor Activity Service Gwersyll Llangrannog 14 Gwersyll Glan-llyn 14 Gwersyll Caerdydd 15 Case Study 3 – Sian Elin Williams 16–17 Treasurer’s Report 18 Sponsors 19 External Funding Sources 20–21 Financial Information 22–26 urdd.cymru Over 60% of those THE YEAR attending sports IN BRIEF clubs are girls Over 43,000 have 98 new clubs have stayed in our been developed over Residential Centres the year Over 90,000 visited the Eisteddfod Turnover of 11,000 activities £9.6 million were organised in the community 2.2 million Twitter 273 members accounts have seen of staff #urdd2016 more at 53,318 members urdd.cymru URDD ANNUAL 6 URDD ANNUAL 7 GOBAITH REPORT GOBAITH REPORT CYMRU 2015–16 CYMRU 2015–16 ChieF EXecutiVE’S Report Chair’S Report Sioned Hughes Tudur Dylan Jones I knew that I had made one of the As Chair of the Urdd, it gives me great best decisions of my life coming to pleasure to report that over 53,000 work for the Urdd when I heard for children and young people became the first time the stamping of feet members of this unique organisation and children’s laughter in the corridors over the last year. The Flintshire Urdd of the Centre in Cardiff. -

Garw Valley Community Sports Hubs – Feasibility Study
GARW VALLEY COMMUNITY SPORTS HUBS – FEASIBILITY STUDY A REPORT BY JANUARY 2018 CONTENTS Page Section 1 – Introduction and Background 1 Section 2 – Need Analysis 3 Section 3 – Community Hub Options and Financial 12 Projections Section 4 – Conclusions and Way Forward 27 APPENDICES Appendix A – Market Segmentation Appendix B – Facility Audit Appendix C – Facility Analysis Appendix D – Management Options Appendix E – Financial Projections Appendix F – Stakeholder Workshop Attendees Appendix G – Project Plan SECTION 1 – INTRODUCTION AND BACKGROUND Introduction 1.1 Bridgend County Borough Council (the Council) as lead body for Reach (the Rural Development Programme for Bridgend) is currently seeking to explore the potential for the development of one or more sports based community sports hubs in the Garw Valley. 1.2 As a result RPT Consulting has been appointed to develop a feasibility study for community sports hubs based in the Garw Valley, which will seek to address the needs of the local population and key stakeholders. Background 1.3 Currently in the Garw Valley as with all other areas in Bridgend, sports and community groups are considering the transfer of sports and community venues and assets from the Council, through the Community Asset Transfer (CAT) process. 1.4 Some of the assets within the Garw Valley are in a poor state of repair and well below an acceptable standard. The cost of repairing and maintaining these assets is beyond the reach of many of the sport and community groups and therefore a potential solution is being sought to ensure that sporting and community activities are not lost. 1.5 To support the CAT process, Reach has already produced a ‘Rural Community Asset Transfer Toolkit’ which provides groups with a step by step guide to asset transfer and also commissioned a report ‘Review of Sustainable Community Venues and Assets in Bridgend County Borough’, which provides a detailed understanding of the issues faced by groups who both currently are or are considering managing/owning/leasing community facilities. -

Table Tennis Wales Tenis Bwrdd Cymru Butterfly CARDIFF GRAND PRIX
Table Tennis Wales Tenis Bwrdd Cymru Presents Butterfly CARDIFF GRAND PRIX A Table Tennis England Satellite Grand Prix Tournament Supported by Sports Wales th th 17 /18 December 2016 Referee: Tournament Organiser: Steve Smith (NR) Ron Davies Sport Wales National Deputy Referee: Assistant Organiser: Centre, Ron Davies Marian Davies Sophia Gardens, Cathedral Road, Referee’s Assistant: Organising Committee: Cardiff, Phil Avery National Competitions Committee. CF11 9SW TOURNAMENT REGULATIONS (to be retained) 1. Every entrant must be affiliated as a player member to Table Tennis England or be a member of another national association in membership of the ITTF. 2. Table Tennis England Tournament Regulations apply to this tournament including Regulation R (Regulations banning use of certain adhesives and restricting “gluing-up”). ITTF Regulations for International Competition apply except those relating to matters covered by items marked (x) in this entry form. 3. Completion and submission of this entry form signifies agreement by the entrant to the conditions of the competition including the variations from the ITTF requirements. 4. All competitors will be required to umpire. 5. All matches will be the best of 5 games. Play throughout will be on a knockout basis, with the exception of the preliminary rounds in all singles and doubles events, which will be in groups of four (except for banded singles events where there are less than 20 tables which will be in groups of three) with the first two players Closing Date: 05/12/16 qualifying. The final order in a group shall be determined as per ITTF regulation 3.7.5 for group competitions except that where a player concedes a match he/she shall receive -3 group points (x). -
Climbing Higher Equality Impact Assessment , File Type
Inclusive Policy Making Detailed Assessment Report Title: Climbing Higher Creating an Active Wales Department/Division: Department of Public Health and Health Professions Lead Official: Chris Tudor-Smith Introduction: In response to the National Assembly for Wales Audit Committee’s report; Increasing Physical Activity in Wales the Chief Medical Officer was given responsibility to lead the co-ordination of a cross departmental work on physical activity and to develop a physical activity action plan. Development of the Strategy To ensure that the cross cutting nature of the plan was recognised an internal stakeholders group was established which consisted of representation from the following Departments: Department for Children, Education, Lifelong Learning and Skills Department for Constitutional Affairs, Equality and Communications Department for Economy and Transport Department for Environment, Sustainability and Housing Department for Health and Social Services Department for Public Health and Health Professions Department for Rural Affairs and Heritage Department for Social Justice and Local Government An external stakeholder group was also established and consisted of the following organisations: Chief Leisure Officers Federation of Disability Sport Wales Governing Bodies of Sport Outdoor Education Advisory Panel Sport Council for Wales Welsh Sports Association Wales Centre for Health Welsh Council for Voluntary Action National Public Health Newport City Council/ Local Health Service Board Sustrans Welsh Local Government Association Countryside Council for British Universities and College Sport Wales British Waterways Play Wales Association of School and College Skills Active Lecturers In addition meetings were held with other external bodies including Disability Wales Minority Ethnic Women’s Network Lead official in Sport Council for Equality Funky Dragon Healthy Schools co-ordinators In addition a wider stakeholders consultation was held in December 2008. -

Affinity-Brands.Pdf
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z # A A & L COMPANY CARD A & L MONEYBACK INSTANT A & L PREMIER MONEYBACK A & L YOUNG WORKER AA ABBEY CASH BACK ABBEY STUDENTS ABERDEEN COLLEGE ABERDEEN F.C. ABN AMRO PRIVATE BANKING ACCA ACORN CHILDRENS HOSPICE ACORN COMPUTERS ACTION FOR CHILDREN ADMIRAL INSURANCE ADMIRAL INSURANCE SERVICES LTD ADVANCED MOBILE COMMUNICATIONS AFC BOURNEMOUTH AFFINITY INSURANCE MARKETING AFFINITY PUBLISHING AGRICREDIT LTD AIRCRAFT OWNERS/PILOTS ASSOC.UK ALFA ROMEO ALLIANCE AND LEICESTER CARD ALLIED DUNBAR ASSURANCE PLC AMAZON.CO.UK AMBASSADOR THEATRE AMBER CREDIT AMBULANCE SERVICE BENEVOL FUND AMERICAN AIRLINES AMERICAN AUTO ASSOC AMEX CERTIFICATION FOR INSOURCING AMP BANK AMSPAR AMWAY (UK) LTD ANGLIA MOTOR INSURANCE ANGLIAN WINDOWS LIMITED ANGLO ASIAN ODONTOLOGICAL GRP AOL BERTELSMANN ONLINE APOLLO LEISURE VIP ENTERTAINMENT CARD APPLE ARCHITECTS & ENGINEERS ARMY AIR CORPS ASSOC ARSENAL ARTHRITIS CARE ASPECT WEALTH LIMITED ASSOC ACCOUNTING TECHNICIANS ASSOC BRIT DISPENSING OPTICIANS ASSOC CARAVAN/CAMP EXEMP ORGN ASSOC OF BRITISH TRAVEL AGENTS ASSOC OF BUILDINGS ENGINEERS ASSOC OF FST DIV CIVIL SERVANTS ASSOC OF INT'L CANCER RESEARCH ASSOC OF MANAGERS IN PRACTICE ASSOC OF OPERATING DEPT. PRACT ASSOC OF OPTOMETRISTS ASSOC OF TAXATION TECHNICIANS ASSOC PROF AMBULANCE PERSONNEL ASSOC RETIRED PERSONS OVER ASSOCIATION FOR SCIENCE EDUCATION ASSOCIATION OF ACCOUNTING TECHNICIANS ASSOCIATION OF BRITISH ORCHESTRAS ASSOCIATION OF MBA'S ASSOCIATION OF ROYAL NAVY OFFICERS ASTON MARTIN OWNERS CLUB LIMITED ASTON VILLA -

I Gwrdd  Gwasanaeth T1
Aberystwyth - Llanbedr Pont Steffan/Lampeter; T1 Llanbedr Pont Steffan/Lampeter - Caerfyrddin/Carmarthen drwy/via Llanrhystud - Aberaeron - Llanybydder - Pencader Yn weithredol/Effective from 22/02/2015 Dydd Llun i ddydd Sadwrn • Monday to Saturday First Cymru am/pm am am am am am am am pm pm pm pm pm pm pm pm pm Aberystwyth, Gorsaf Fysiau/Bus Station ... 6.40 7.40 8.40 9.40 10.40 11.40 12.40 1.40 2.40 3.40 4.40 5.40 6.40 7.45R 9.40 Aberystwyth, Morrisons ... 6.45 7.45 8.45 9.45 10.45 11.45 12.45 1.45 2.45 3.45 4.45 5.45 6.45 7.50R 9.45 Llanfarian, Pentre-bont ... 6.51 7.51 8.51 9.51 10.51 11.51 12.51 1.51 2.51 3.51 4.51 5.51 6.51 7.56R 9.51 Blaenplwyf, Capel/Chapel ... 6.55 7.55 8.55 9.55 10.55 11.55 12.55 1.55 2.55 3.55 4.55 5.55 6.55 8.00R 9.55 Llanrhystud, gyf Y Llew Du/opp Black Lion ... 7.03 8.03 9.03 10.03 11.03 12.03 1.03 2.03 3.03 4.03 5.03 6.03 7.03 8.08R 10.03 Llanon, Central Hotel ... 7.07 8.07 9.07 10.07 11.07 12.07 1.07 2.07 3.07 4.07 5.07 6.07 7.07 8.12R 10.07 Aberaeron, Sgwâr Alban Square cyr/arr .. -

South Wales Calendar 2018-19 UPDATED
Sytner MINI Tennis Competitions South Wales - Winter 2018/19 WHAT ARE SYTNER MINI EVENTS? Local, fun tennis competitions! A perfect introduction into playing matches whilst having fun with friends (and making new ones). They’ll be an element of team competition and the children will get plenty of help with how to play a match. Sytner MINI events are ideal for a child’s FIRST EVER TOURNAMENT experience. You’ll find the calendar of events and & the entry form on the next few pages We look forward to seeing you and your child at a Sytner MINI Fun Tennis Competition soon! @SytnerTennis Tennis Wales How To Enter It’s quick and easy to sign up for the Sytner MINI Competitions Option 1 - drop an email to [email protected] with either a scanned copy or photo of the completed entry form. Option 2 - fill in the entry form below and, if the event is at your club hand it into the coaching team and they’ll make sure you’re included in the event. PLEASE MAKE SURE YOU REGISTER FOR ALL THE EVENTS YOU’D LIKE TO PLAY so the organiser can include your child in their plans and contact you in the event of bad weather etc. The entry fee is just £5-£8 per player per event depending on the venue PAY THE ORGANISER ON THE DAY WHICH EVENTS SHOULD I ENTER? MINI red - aimed at children aged 6, 7 & 8 years old - lots of fun and a chance to learn practice playing matches. We’ll use mini red balls, mini red courts and simple scoring formats. -

Annual Report 2005 – 2006
This watermark does not appear in the registered version - http://www.clicktoconvert.com North Pembrokeshire Transport Forum Fforwm Trafnidiaeth Gogledd Penfro ANNUAL REPORT 2005 – 2006 Introduction The Forum works for the provision of an effective integrated transport system in the North Pembrokeshire area, promotes the benefits of public transport and works towards greater use of public transport systems. Its activities involve conducting research and gathering data with regard to all aspects of transport; providing an advice and assistance service to the travelling public; actively promoting its aims to and through governmental, quasi-governmental and advisory bodies; and working with bodies with similar aims. The Forum has been taking stock of the transport scene in North Pembrokeshire as it comes to the end of its three-year grant from the Sustainable Development Fund and its first six years of work. With regard to the provision of transport we have seen many improvements in bus, cycle and community transport services and facilities in North Pembrokeshire during the past six years. In contrast, there have been no improvements in train services. The following report provides more detail with regard to transport developments and the work of the Forum during the past year. Buses Service improvements: · Pembrokeshire County Council (PCC) is subsidising extra services between Fishguard and Haverfordwest on Friday and Saturday evenings in response to a request from POINT, the Fishguard young people’s drop-in centre. · In consultation with the community, PCC has arranged improved bus services for Spittal, with the addition of a Wednesday service and a shorter journey added to the existing Friday service. -
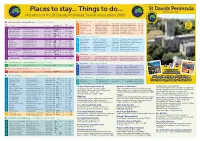
Pdf Version of the Broadsheet
ds Pen vi in a s Grove Hotel St Davids The Waterings B&B St Davids Holiday Cottages Treginnis Cottage Y Bwthyn St. Bride’s Bay Cottages D u l t a Places to stay... Things to do... S High Street, St Davids SA62 6SB Anchor Drive, High St, St Davids, SA62 6QH Glowty & Ty Draw, Treleddyd Fawr SA62 6PP Treginnis Uchaf, St Davids SA62 6RS Felin Isaf, St Davids SA62 6QB Tel: 01437 720027 T Tel: 01437 720341 Tel: 01437 720876 Tel: 01437 720808 Tel: 07791 903221 Tel: 01437 720853 o n A small selection of quality cottages around the beautiful u o r ti Perfectly located for exploring the famous City of St. Davids and Beautifully presented rooms with TV, beverage tray and 'Step off the world' and stay in our beautifully restored and Relax and revitalize in a comfortable farm cottage Exquisitely refurbished medieval barn downstream from Lleoedd i aros... Pethau i wneud... is a coastline of Solva and St Davids. Free colour brochure. t i Assoc the stunning Pembrokeshire coast. Eat, sleep, drink and relax en-suite bathroom - some also with private sitting room. furnished stone barns set in 20 acres. Stunning views - dogs on the St Davids Peninsula. Cathedral half mile from the sea. In idyllic wild valley. Short breaks available. Pets welcome. with us at The Grove St Davids. Tranquil, landscaped grounds. Private parking. welcome - free Wi-Fi Picturesque coastal walks a few minutes away. A secluded paradise awaits. [email protected] Members of the St Davids Peninsula Tourist Association email: [email protected] [email protected] -

Bangor University DOCTOR of PHILOSOPHY the History of the Jewish Diaspora in Wales Parry-Jones
Bangor University DOCTOR OF PHILOSOPHY The history of the Jewish diaspora in Wales Parry-Jones, Cai Award date: 2014 Awarding institution: Bangor University Link to publication General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ? Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Download date: 07. Oct. 2021 Contents Abstract ii Acknowledgments iii List of Abbreviations v Map of Jewish communities established in Wales between 1768 and 1996 vii Introduction 1 1. The Growth and Development of Welsh Jewry 36 2. Patterns of Religious and Communal Life in Wales’ Orthodox Jewish 75 Communities 3. Jewish Refugees, Evacuees and the Second World War 123 4. A Tolerant Nation?: An Exploration of Jewish and Non-Jewish Relations 165 in Nineteenth and Twentieth Century Wales 5. Being Jewish in Wales: Exploring Jewish Encounters with Welshness 221 6. The Decline and Endurance of Wales’ Jewish Communities in the 265 Twentieth and Twenty-first Centuries Conclusion 302 Appendix A: Photographs and Etchings of a Number of Wales’ Synagogues 318 Appendix B: Images from Newspapers and Periodicals 331 Appendix C: Figures for the Size of the Communities Drawn from the 332 Jewish Year Book, 1896-2013 Glossary 347 Bibliography 353 i Abstract This thesis examines the history of Jewish communities and individuals in Wales. -

The Sports Council for Wales and Sports Council for Wales Trust 1 April 2016 – 31 March 2017
Y Pwyllgor Cyfrifon Cyhoeddus / Public Accounts Committee PAC(5)-25-17 P1 SPORT WALES CHWARAEON CYMRU ANNUAL REPORT AND ACCOUNTS 2016- 2017 1 THE SPORTS COUNCIL FOR WALES AND SPORTS COUNCIL FOR WALES TRUST 1 APRIL 2016 – 31 MARCH 2017 ANNUAL REPORT AND ACCOUNTS The Annual Report incorporates the Performance Report including the Sustainability Report, and the Accountability Report including Remuneration Report. The Sports Council for Wales has adopted International Financial Reporting Standards (IFRS). Sport Wales is a Sole Trustee of the Sports Council for Wales Trust. HISTORY AND STATUTORY BACKGROUND The Sports Council for Wales (known by its trade name Sport Wales) was established by Royal Charter dated 4 February 1972, with the objectives of "fostering the knowledge and practice of sport and physical recreation among the public at large in Wales and the provision of facilities thereto". It is financed by annual funding from the Welsh Government and from income generated from its activities. These Statements of Account are prepared pursuant to Article 15 of the Royal Charter for the Sports Council for Wales (Sport Wales) in a form determined by the Welsh Government with the approval of HM Treasury. A copy of the Accounts Direction is available for public inspection at Sport Wales offices at Sophia Gardens in Cardiff. The Sports Council for Wales Trust was constituted on 16 May 1972 and is registered as a charity with the Charity Commissioners in England and Wales, with the charitable objectives of: 1. preserving and safeguarding the physical and mental health of the community through physical recreation (including sport) and the education in relation thereto; 2.