Candidate Information Pack
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Provincial Patter the Quarterly Newsletter of the Province of Ross and Cromarty Issue No 74 February 2013
Provincial Patter The Quarterly Newsletter of the Province of Ross and Cromarty Issue No 74 February 2013 Editorial Provincial Grand Lodge: th Our next meeting of Provincial Grand Lodge Welcome to the 74 edition of the Patter. will be held within Robertson’s Lodge No 134 th This Quarter I’d like to use the editorial to bring in Cromarty on Wednesday 13 February 2013, everyone up to date with the work of the Scottish commencing at 8.00pm. All Masters and Masonic Materials Group who are working hard on two Wardens have a duty to represent their main projects at the present time. First, is the Masonic respective Lodges at these Quarterly War Memorial project - please ensure that if you have a Communications and likewise a good Masonic War Memorial in or near your Lodge that the attendance of Provincial Office–bearers would details are passed on via the following web-site: - be appreciated. All Master Masons in good www.grand-lodge.net/asp/mwmform.asp standing are also welcome to attend these meetings. There is a facility on the web page to check whether or not your own Lodge information has been submitted. A It was my pleasure to attend the Installation of comprehensive list and an accompanying article will the Grand Master Mason in Grand Hall followed appear in the 2014 Grand Lodge Year Book. by the Festival of St Andrew in the Edinburgh Corn Exchange where the “star performance” The second project is the Oral History project. It is hoped was the Address to the Haggis superbly narrated to secure Lottery Funding to enable equipments and by Brother Ramsay McGhee. -
Emergency Department Activity
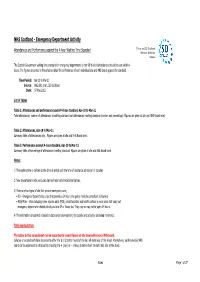
NHS Scotland - Emergency Department Activity Attendances and Performance against the 4-hour Waiting Time Standard This is an ISD Scotland National Statistics release. The Scottish Government waiting time standard for emergency departments is that 98 % of all attendances should be seen within 4 hours. The figures presented in these tables detail the performance of each individual site and NHS board against the standard. Time Period: Apr-10 to Mar-11 Source: A&E data mart, ISD Scotland Date: 07 May 2012 List of Tables Table 1: Attendances and performance against 4-hour standard, Apr-10 to Mar-11 Total attendances, number of attendances breaching standard and attendances meeting standard (number and percentage). Figures are given at site and NHS Board level. Table 2: Attendances, Apr-10 to Mar-11 Summary table of attendances only. Figures are given at site and NHS Board level. Table 3: Performance against 4-hour standard, Apr-10 to Mar-11 Summary table of percentage of attendances meeting standard. Figures are given at site and NHS Board level. Notes: 1) The waiting time is defined as the time of arrival until the time of discharge, admission or transfer. 2) New presentations only; excludes planned return and recall attendances. 3) There are two types of site that provide emergency care; • ED - Emergency Departments; sites that provide a 24 hour emergency medicine consultant led service • MIU/Other - sites including minor injuries units (MIU), small hospitals and health centres in rural areas that carry out emergency department related activity and are GP or Nurse led. They may or may not be open 24 hours. -

Accident and Emergency: Performance Update
Accident and Emergency Performance update Prepared by Audit Scotland May 2014 Auditor General for Scotland The Auditor General’s role is to: • appoint auditors to Scotland’s central government and NHS bodies • examine how public bodies spend public money • help them to manage their finances to the highest standards • check whether they achieve value for money. The Auditor General is independent and reports to the Scottish Parliament on the performance of: • directorates of the Scottish Government • government agencies, eg the Scottish Prison Service, Historic Scotland • NHS bodies • further education colleges • Scottish Water • NDPBs and others, eg Scottish Police Authority, Scottish Fire and Rescue Service. You can find out more about the work of the Auditor General on our website: www.audit-scotland.gov.uk/about/ags Audit Scotland is a statutory body set up in April 2000 under the Public Finance and Accountability (Scotland) Act 2000. We help the Auditor General for Scotland and the Accounts Commission check that organisations spending public money use it properly, efficiently and effectively. Accident and Emergency | 3 Contents Summary 4 Key messages 7 Part 1. A&E waiting times 9 Part 2. Reasons for delays in A&E 20 Part 3. Action by the Scottish Government 37 Endnotes 41 Appendix 1. NHS Scotland A&E departments and minor injury units 43 Appendix 2. National context for A&E and unscheduled care, 2004 to 2014 45 Exhibit data When viewing this report online, you can access background data by clicking on the graph icon. The data file will -

Emergency Departments
ED Site List 220711 v2.xls NHS Scotland - Emergency Departments Table 1: NHS Scotland - list of sites providing emergency care File NHS Board Site Type Location Name Location Address Comments Type Ayrshire & Arran ED Ayr Hospital DALMELLINGTON ROAD, AYR, KA6 6DX E Crosshouse Hospital KILMARNOCK ROAD, KILMARNOCK, AYRSHIRE, KA2 0BE E MIU/Other Arran War Memorial Hospital LAMLASH, ISLE OF ARRAN, KA27 8LF A Davidson Cottage Hospital THE AVENUE, GIRVAN, KA26 9DS A Closed from May-10 Girvan Community Hospital BRIDGEMILL, GIRVAN, AYRSHIRE, KA26 9HQ A Opened from May-10 Lady Margaret Hospital COLLEGE ST, MILLPORT, ISLE OF CUMBRAE, KA28 0HF A Opened from Oct-07 Borders ED Borders General Hospital MELROSE, TD6 9BS E MIU/Other Hawick Cottage Hospital VICTORIA ROAD, HAWICK, TD9 7AH A Hay Lodge Hospital NEIDPATH ROAD, PEEBLES, EH45 8JG A Kelso Hospital INCH ROAD, KELSO, TD5 7JP A Knoll Hospital STATION ROAD, DUNS, TD11 3EL A Dumfries & Galloway ED Dumfries & Galloway Royal Infirmary BANKEND ROAD, DUMFRIES, DG1 4AP E Galloway Community Hospital DALRYMPLE STREET, STRANRAER, DG9 7DQ E MIU/Other Castle Douglas Hospital ACADEMY STREET, CASTLE DOUGLAS, DG7 1EE A Kirkcudbright Hospital TOWNEND, KIRKCUDBRIGHT, DG6 4BE A Moffat Hospital HOLMEND, MOFFAT, DG10 9JY A Newton Stewart Hospital NEWTON STEWART, DG8 6LZ A Fife ED Victoria Hospital HAYFIELD ROAD, KIRKCALDY, KY2 5AH E MIU/Other Adamson Hospital BANK STREET, CUPAR, KY15 4JG A Queen Margaret Hospital WHITEFIELD ROAD, DUNFERMLINE, KY12 0SU E St Andrews Memorial Hospital ABBEY WALK, ST ANDREWS, KY16 9LG -

North & West Operational Unit Integrated Team Leads, Advanced
North & West Operational Unit Integrated Team Leads, Advanced Practitioners and Health & Social Care Co-ordinators North – Caithness & Sutherland Districts East Caithness West Caithness Covering East & West Caithness Integrated Team Lead Integrated Team Lead Advanced Practitioner, SW Teresa Green Nikki MacKenzie Eugene McGowan Base: Wick Medical Centre Base: Dunbar Hospital Base: Dunbeath Medical Practice 01955 606915 / 07930 487157 01847 893263 / 07972 854095 07825 086882 [email protected] [email protected] [email protected] DN Professional Lead/Advanced DN Advanced Practitioner/ Prof Lead Health & Social Care Co-ordinator Practitioner Carena MacIvor Julie Calder Jenny Forbes Base: Thurso Health Centre Base: Caithness General Hospital Base: Wick Medical Centre 01847 893442 / 07789746139 01955 880219 / 07805 490742 01955 603784 / 07789 746295 [email protected] [email protected] [email protected] East Sutherland N&W Sutherland Covering whole of Sutherland Integrated Team Lead Integrated Team Lead (N&W) Advanced Practitioner, SW Heather Taylor Post vacant Roddy MacSween Base: Base: Lawson Memorial Hospital [email protected] Advanced Practitioner, Nursing (N) 01408 664077 / 07795 120615 Post vacant [email protected] Advanced Practitioner, Nursing Janice Macrae Advanced Practitioner, Nursing (W) Health & Social Care Co-ordinator Base: Brora/Helmsdale Health Centre Sandra MacFarlane Irene Anderson 07748 761739 Base: Assynt Health Centre Base: Lawson Memorial Hospital [email protected] 01571 844452 -

Northern Pathways
NORTHERN PATHWAYS A Guide to Services for the Armed Forces Community in the North of Scotland Foreword By Keith Brown MSP I am pleased to support the launch of the first resource guide for the Armed Forces community in the North of Scotland. This guide has been developed by the team at Poppyscotland Inverness ably supported by members of the local Armed Forces Community Covenant Partners’ groups, and will serve as a vital reference point for members of the Armed Forces community in the North of Scotland. The Highlands of Scotland and the surrounding areas have always been a strong recruiting ground for the Armed Forces. The area has also been home to a significant number of large military bases which has seen many servicemen and women who have been based at them resettle in the areas where they once served. Recent research suggests that the North of Scotland is home to approximately 20% of Scotland’s Armed Forces community. It is, therefore, essential that we empower these individuals with the knowledge of the support that is available to them and I firmly believe that this guide achieves this. The Scottish Government places great importance on our Armed Forces community, most recently set out in our “Renewing Our Commitments” strategy. Consistent with this strategy and the values of the Armed Forces Covenant, I am clear that the whole nation has a moral obligation to members of the Armed Forces and their families. They should suffer no disadvantage as a result of their service and deserve the best possible support, when needed. -

Emergency Departments
ED-site-list NHS Scotland - Emergency Departments Table 1: NHS Scotland - list of sites providing emergency care NHS Board Site Type Location Name Location Address File Type Comments Ayrshire & Arran ED Ayr Hospital DALMELLINGTON ROAD, AYR, KA6 6DX E Crosshouse Hospital KILMARNOCK ROAD, KILMARNOCK, AYRSHIRE, KA2 0BE E MIU/Other Arran War Memorial Hospital LAMLASH, ISLE OF ARRAN, KA27 8LF A Davidson Cottage Hospital THE AVENUE, GIRVAN, KA26 9DS A Closed from May-10 Girvan Community Hospital BRIDGEMILL, GIRVAN, AYRSHIRE, KA26 9HQ A Opened from May-10 Lady Margaret Hospital COLLEGE ST, MILLPORT, ISLE OF CUMBRAE, KA28 0HF A Opened from Oct-07 Borders ED Borders General Hospital MELROSE, TD6 9BS E MIU/Other Hawick Cottage Hospital VICTORIA ROAD, HAWICK, TD9 7AH A Hay Lodge Hospital NEIDPATH ROAD, PEEBLES, EH45 8JG A Kelso Hospital INCH ROAD, KELSO, TD5 7JP A Knoll Hospital STATION ROAD, DUNS, TD11 3EL A Dumfries & Galloway ED Dumfries & Galloway Royal Infirmary BANKEND ROAD, DUMFRIES, DG1 4AP E Galloway Community Hospital DALRYMPLE STREET, STRANRAER, DG9 7DQ E MIU/Other Castle Douglas Hospital ACADEMY STREET, CASTLE DOUGLAS, DG7 1EE A Kirkcudbright Hospital TOWNEND, KIRKCUDBRIGHT, DG6 4BE A Moffat Hospital HOLMEND, MOFFAT, DG10 9JY A Newton Stewart Hospital NEWTON STEWART, DG8 6LZ A Fife ED Queen Margaret Hospital WHITEFIELD ROAD, DUNFERMLINE, KY12 0SU E Victoria Hospital HAYFIELD ROAD, KIRKCALDY, KY2 5AH E MIU/Other Adamson Hospital BANK STREET, CUPAR, KY15 4JG A St Andrews Memorial Hospital ABBEY WALK, ST ANDREWS, KY16 9LG A Forth Valley -

Business Bulletin Iris Ghnothaichean
Friday 27 October 2017 Business Bulletin Iris Ghnothaichean Today's Business Meeting of the Parliament Committee Meetings There are no meetings today. There are no meetings today. Friday 27 October 2017 1 Today's Business Future Business Motions & Questions Legislation Other Gnothaichean an-diugh Gnothaichean ri teachd Gluasadan agus Ceistean Reachdas Eile Chamber | Seòmar Meeting of the Parliament There are no meetings today. Friday 27 October 2017 2 Today's Business Future Business Motions & Questions Legislation Other Gnothaichean an-diugh Gnothaichean ri teachd Gluasadan agus Ceistean Reachdas Eile Committees | Comataidhean Committee Meetings There are no meetings today. Friday 27 October 2017 3 Today's Business Future Business Motions & Questions Legislation Other Gnothaichean an-diugh Gnothaichean ri teachd Gluasadan agus Ceistean Reachdas Eile Chamber | Seòmar Future Meetings of the Parliament Business Programme agreed by the Parliament on 25 October 2017 Tuesday 31 October 2017 2:00 pm Time for Reflection - Reverend Eileen M Ross, BD MTh, Minister, Linwood Parish Church, Linwood, Renfrewshire followed by Parliamentary Bureau Motions followed by Topical Questions (if selected) followed by Ministerial Statement: Scottish Greenhouse Gas Emissions Annual Target Report for 2015 followed by Scottish Government Debate: The Promotion of Walking and Cycling as Active Travel in Scotland followed by Business Motions followed by Parliamentary Bureau Motions 5:00 pm Decision Time followed by Members' Business — S5M-08226 Ben Macpherson: Unfair -
Guidelines for Learning Disabilities Nov 2013
Guidelines working with pregnant women and new mothers with learning disabilities Guidelines for practitioners working with pregnant women and new mothers with learning disabilities Warning – Document uncontrolled when printed Policy Reference: 041113 Date of Issue: November 2013 Prepared by: Sandra Harrington Date of Review: November Midwifery Development Officer 2015 Lead Reviewer: Sandra Harrington Version: 2 Midwifery Development Officer Authorised by: NMAHP Date: 1st November 2013 Ratification Group EQIA undertaken: Yes Date: September 2013 Distribution NHS Highland Highland Health & Social Care Board Nurse Director Head of Health Head of Midwifery Principal Officer Nursing Lead Midwives Principal Officer AHPs Lead Nurses Lead Officer Child Protection Midwives Child Protection Advisors Supervisors of Midwives Area & District Managers NMAHP Leadership Committee Health Visitors GPs & GP sub group Integrated Services Coordinators Consultant Nurse Learning Disabilities Integrated Services Officers Adult Learning Disabilities Teams Children & Family Social Work Teams Third Sector Children’s Learning Disabilities Action for Children/Home Start/Family Teams First/Children Housing Team 1st/CALA/Barnados/Calman/Cairn & Albyn Housing Method CD Rom E-mail X Paper Intranet X Warning – Document uncontrolled when printed Version: 2 Date of Issue: November 2013 Page: 1 Date of Review: November 2015 Guidelines working with pregnant women and new mothers with learning disabilities Contents Page no 1. Introduction 3 2. Aim 5 3. Principles of Good Practice 5 3.1 An early response 5 3.2 Needs led support 6 3.3 Assets led model rather than deficit led 7 3.4 Time 7 3.5 Effective support involves a wide range of strategies 7 3.6 Capacity development 8 3.7 Parenting with support 9 3.8 Involving the extended family 9 4. -

NHS Highland, Per Ryan Nelson, Scott Kirby, Lawson Memorial
Agenda 6.12 item Report PLN/042/18 no THE HIGHLAND COUNCIL Committee: North Planning Applications Committee Date: 5 June 2018 Report Title: 18/01067/FUL: Lawson Memorial Hospital, Golspie Report By: Area Planning Manager – North 1. Purpose/Executive Summary 1.1 Applicant: NHS Highland per Ryan Nelson/Scott Kirby Description of development: Installation of 6 LPG tanks Ward: 4 – East Sutherland and Edderton Category: Local Reasons Referred to Committee: Community Council objection All relevant matters have been taken into account when appraising this application. It is considered that the proposal accords with the principles and policies contained within the Development Plan and is acceptable in terms of all other applicable material considerations. 2. Recommendation 2.2 Members are asked to agree the recommendation to Grant as set out in section 11 of the report 3. PROPOSED DEVELOPMENT 3.1 The application seeks full planning permission for the siting of 6 x 1 tonne Liquefied Petroleum Gas (LPG) tanks in two rows within the rear grounds of Lawson Memorial Hospital. The tanks are located 3m from the northern boundary. The proposed tanks would sit on a concrete base, measuring 9.2m x 6m. It is now proposed to erect a 1.8 m timber high fenced around the tanks to create a compound measuring 12m x 8m with two outwards opening gates on non-adjacent sides to help screen the site. 3.2 No formal pre-application was sought in advance of the submission. 3.3 The site is served by the existing access onto the A9 road. 3.4 The application is supported by Tank Screening Information which sets out options that can be used to screen the tanks. -

Delivering Practical Partnerships to Tackle Fuel Poverty and Improve Energy Efficiency Teresa Bray Chief Executive Warm Recovery – the Plan
Inspiring change for people and the environment Delivering practical partnerships to tackle fuel poverty and improve energy efficiency Teresa Bray Chief Executive Warm Recovery – The Plan • Edinburgh and Lothian Health Foundation • 2 Year project supporting patients on discharge from hospital – 2014/16 • Respiratory nurses and discharge staff at Royal Infirmary Edinburgh and Western General • Senior level buy in during development Warm Recovery – Delivery • Minimal Senior support at delivery stage • Busy delivery staff at Discharge Hubs • Requirement for NHS Lothian email address for referrals • Successes through Astley Ainsley and Family Nurse partnership • Local Opportunities for Older People wider Third Sector Support at home • Learnings Home Energy Scotland support • Impartial advice and support supported by the Scottish Government, managed by the Energy Saving Trust and delivered across Scotland • Referrals to Warmer Homes Scotland for heating and insulation • Links in to other organisations NHS Highland Community Hospitals • Regular presence at Raigmore • Following Home Energy Scotland outreach work, Lorraine Coe, NHS Highland Sutherland District Lawson Memorial Hospital Manager driving force. • Referrals at discharge. • Extends reach to very vulnerable households • Data protection challenging Migdale Hospital Outcomes • 45 referrals • 16 home visits • 7 Warmer Homes Scotland referrals • 16 onward referrals and signposting • Currently being rolled out to community health teams in Suhterland, wider roll out being considered • Regular -

Adult Social Care Team Contact Details
Adult Social Care Team Contact Details NORTH Team Manager Address Tel Caithness Eugene McGowan Community Wing, Riverview Medical Practice, Martha Terrace, Wick, KW1 5EL 01955 604134 [email protected] Community Health Centre, Davidson’s Lane, Thurso KW14 7AF 01847 893442 [email protected] Sutherland Roddy MacSween 1st Floor, Lawson Memorial Hospital, Golspie, Sutherland KW10 6SS 01408 664018 [email protected] WEST Team Manager Address Tel West Ross Ian Smith Ullapool Service Point, North Road, Ullapool, IV26 2XL [email protected] Skye & Lochalsh Alan Howson Tigh na Drochaid, Bayfield, Portree IV51 9EW 01471 820174 [email protected] Lochaber Eleanor Barrie Fort William Health Centre, Camaghael, Fort William PH33 7AQ 01397 709873 MID Team Manager Address Tel Mid Ross Shona Knight Dingwall Health Centre, Ferry Road, Dingwall IV15 9QS 01349 860460 [email protected] East Ross Graeme MacKinnon County Community Hospital, Saltburn Road, Invergordon IV18 0JR 01349 853131 [email protected] SOUTH Team Manager Address Tel Inverness East Urban Sheena McLellan Assynt House, Beechwood Park, Inverness, IV2 3BW [email protected] Inverness East Rural Charlie MacKinnon 01463 888333 Inverness West Urban Morag Scott Corbett Centre Inverness. Corbett Centre Coronation Park Inverness IV3 8AD Inverness West Rural Paula Logan [email protected] Nairn Eilidh MacMillan Town & County Hospital, Nairn, Highland 01667 422702 [email protected] Badenoch & Strathspey Alan Barr The Glen Centre, 17 Kinveachy Gardens, Aviemore PH22 1RX 01479 812618 [email protected] Updated 01/02/2017 Updated 01/02/2017 .