Pdf Manual (1.756Mb)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Te2, Part Iii
TERMINOLOGIA EMBRYOLOGICA Second Edition International Embryological Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TE2, PART III Contents Caput V: Organogenesis Chapter 5: Organogenesis (continued) Systema respiratorium Respiratory system Systema urinarium Urinary system Systemata genitalia Genital systems Coeloma Coelom Glandulae endocrinae Endocrine glands Systema cardiovasculare Cardiovascular system Systema lymphoideum Lymphoid system Bibliographic Reference Citation: FIPAT. Terminologia Embryologica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, February 2017 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Embryologica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput V: ORGANOGENESIS Chapter 5: ORGANOGENESIS -

Laparoscopic Extraperitoneal Salpingo-Oophorectomy in Women with Suspicious Ovarian Mass, a Way to Reduce the Risk of Spillage
5 Surgical Technique Page 1 of 5 Laparoscopic extraperitoneal salpingo-oophorectomy in women with suspicious ovarian mass, a way to reduce the risk of spillage Giulio Sozzi, Giulia Zaccaria, Mariano Catello Di Donna, Giuseppina Lo Balbo, Stefania Cannarozzo, Vito Chiantera Department of Gynecologic Oncology, University of Palermo, Piazza Nicola Leotta, Palermo, Italy Correspondence to: Giulio Sozzi, MD. Department of Gynecologic Oncology, University of Palermo, Piazza Nicola Leotta 4, 90127 Palermo, Italy. Email: [email protected]. Abstract: The objective of the present paper is to provide a step by step description of the laparoscopic extraperitoneal salpingo-oophorectomy, a surgical technique useful to reduce the risk of spillage in women with suspected ovarian masses. The patient was a 52-year-old woman with sonographic diagnosis of a multilocular, 5 cm lesion, with Color Score 3 at right ovary. Computed tomography (CT) scan excluded any other localization of disease. Tumor markers were negative, except for Ca 19.9 that was 85 IU/mL. Preliminary diagnostic laparoscopy was performed and peritoneal carcinomatosis was excluded. In order to obtain a histological diagnosis, an extraperitoneal right salpingo-oophorectomy was performed. At frozen section analysis it was diagnosed an ovarian adenocarcinoma. Therefore, a laparoscopic complete surgical staging including total hysterectomy, controlateral salpingo-oophorectomy, infracolic omentectomy, multiple peritoneal biopsies, and pelvic and para-aortic lymphadenectomy, was performed. Operative time was 240 minutes and estimated blood loss was about 50 mL. No intra or post-operative complications were observed, and the patient was discharged 3 days after surgery. Final histology showed the presence of clear cell high grade carcinoma in both ovaries without fallopian tubes infiltration. -

Chapter 28 *Lecture Powepoint
Chapter 28 *Lecture PowePoint The Female Reproductive System *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • The female reproductive system is more complex than the male system because it serves more purposes – Produces and delivers gametes – Provides nutrition and safe harbor for fetal development – Gives birth – Nourishes infant • Female system is more cyclic, and the hormones are secreted in a more complex sequence than the relatively steady secretion in the male 28-2 Sexual Differentiation • The two sexes indistinguishable for first 8 to 10 weeks of development • Female reproductive tract develops from the paramesonephric ducts – Not because of the positive action of any hormone – Because of the absence of testosterone and müllerian-inhibiting factor (MIF) 28-3 Reproductive Anatomy • Expected Learning Outcomes – Describe the structure of the ovary – Trace the female reproductive tract and describe the gross anatomy and histology of each organ – Identify the ligaments that support the female reproductive organs – Describe the blood supply to the female reproductive tract – Identify the external genitalia of the female – Describe the structure of the nonlactating breast 28-4 Sexual Differentiation • Without testosterone: – Causes mesonephric ducts to degenerate – Genital tubercle becomes the glans clitoris – Urogenital folds become the labia minora – Labioscrotal folds -
Oogenesis in Mammals
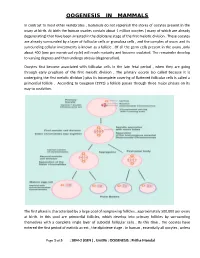
OOGENESIS IN MAMMALS In contrast to most other vertebrates , mammals do not replenish the stores of oocytes present in the ovary at birth. At birth the human ovaries contain about 1 million oocytes ( many of which are already degenerating) that have been arrested in the diplotene stage of the first meiotic division . These oocytes are already surrounded by a layer of follicular cells or granulosa cells , and the complex of ovum and its surrounding cellular investments is known as a follicle . Of all the germ cells present in the ovary ,only about 400 (one per menstrual cycle) will reach maturity and become ovulated. The remainder develop to varying degrees and then undergo atresia (degeneration). Oocytes first become associated with follicular cells in the late fetal period , when they are going through early prophase of the first meiotic division . The primary oocyte (so called because it is undergoing the first meiotic division ) plus its incomplete covering of flattened follicular cells is called a primordial follicle . According to Gougeon (1993) a follicle passes through three major phases on its way to ovulation. The first phase is characterized by a large pool of nongrowing follicles , approximately 500,000 per ovary at birth. In this pool are primordial follicles, which develop into primary follicles by surrounding themselves with a complete single layer of cuboidal follicular cells . By this time , the oocytes have entered the first period of meiotic arrest , the diplotene stage . In human , essentially all oocytes , unless Page 1 of 5 : SEM-2 (GEN ) , Unit#6 : OOGENESIS : Pritha Mondal they degenerate ,remain arrested in the diplotene stage until puberty ; some will not progress past the diplotene stage until the woman’s last reproductive cycle (age 45 to 55 years). -

FEMALE REPRODUCTIVE SYSTEM Female Reproduc�Ve System
Human Anatomy Unit 3 FEMALE REPRODUCTIVE SYSTEM Female Reproducve System • Gonads = ovaries – almond shaped – flank the uterus on either side – aached to the uterus and body wall by ligaments • Gametes = oocytes – released from the ovary during ovulaon – Develop within ovarian follicles Ligaments • Broad ligament – Aaches to walls and floor of pelvic cavity – Connuous with parietal peritoneum • Round ligament – Perpendicular to broad ligament • Ovarian ligament – Lateral surface of uterus ‐ ‐> medial surface of ovary • Suspensory ligament – Lateral surface of ovary ‐ ‐> pelvic wall Ovarian Follicles • Layers of epithelial cells surrounding ova • Primordial follicle – most immature of follicles • Primary follicle – single layer of follicular (granulosa) cells • Secondary – more than one layer and growing cavies • Graafian – Fluid filled antrum – ovum supported by many layers of follicular cells – Ovum surrounded by corona radiata Ovarian Follicles Corpus Luteum • Ovulaon releases the oocyte with the corona radiata • Leaves behind the rest of the Graafian follicle • Follicle becomes corpus luteum • Connues to secrete hormones to support possible pregnancy unl placenta becomes secretory or no implantaon • Becomes corpus albicans when no longer funconal Corpus Luteum and Corpus Albicans Uterine (Fallopian) Tubes • Ciliated tubes – Passage of the ovum to the uterus and – Passage of sperm toward the ovum • Fimbriae – finger like projecons that cover the ovary and sway, drawing the ovum inside aer ovulaon The Uterus • Muscular, hollow organ – supports -

Ovarian Ligament Adenomyoma : a Case Report
Acta chir belg, 2007, 107, 84-85 Ovarian Ligament Adenomyoma : A Case Report L. Choudhrie, N. N. Mahajan, M. V. Solomon, A. Thomas, A. J. Kale, K. Mahajan Padhar Hospital, Padhar, District - Betul, Madhya Pradesh, India. Pin 460005. Key words. Ovarium ; ovarian adenoma ; uterine adenomyoma ; müllerian duct. Abstract. Background : Adenomyoma is a benign tumour composed of smooth muscle and benign endometrium. These tumours typically originate within the uterus. An extra-uterine adenomyoma is a rare entity. Case : We report a case of extra-uterine adenomyoma of the ovarian ligament, which was an incidental finding during a total abdominal hysterectomy and bilateral salpingo-oophorectomy for a benign ovarian tumour in a postmenopausal woman. The mass was round with uterine-type smooth muscle and scattered functional endometrial glands and stroma. Discussion : Only seven other cases of an extra-uterine uterine-like mass are reported in the literature. There have been no cases of adenomyoma in the ovarian ligament reported until now. Conclusion : It is most likely that this uterine-like mass arose from the tissues of the secondary müllerian system. Introduction At laparotomy, a right ovarian tumour measuring 25 ϫ 22 ϫ 24 cm in size was present with a normal sized Extra-uterine adenomyomas may arise from the uterus, uterus and left ovary. A small 0.8 ϫ 0.8 cm nodule, from within the broad ligament, from the fallopian tube, weighing 10gms, was seen on the left ovarian ligament. or from the ovary. Adenomyomas, benign tumours com- Total abdominal hysterectomy with bilateral salpingo- posed of smooth muscle and non-neoplastic endometri- oophorectomy was done. -

Vocabulario De Morfoloxía, Anatomía E Citoloxía Veterinaria
Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) Servizo de Normalización Lingüística Universidade de Santiago de Compostela COLECCIÓN VOCABULARIOS TEMÁTICOS N.º 4 SERVIZO DE NORMALIZACIÓN LINGÜÍSTICA Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) 2008 UNIVERSIDADE DE SANTIAGO DE COMPOSTELA VOCABULARIO de morfoloxía, anatomía e citoloxía veterinaria : (galego-español- inglés) / coordinador Xusto A. Rodríguez Río, Servizo de Normalización Lingüística ; autores Matilde Lombardero Fernández ... [et al.]. – Santiago de Compostela : Universidade de Santiago de Compostela, Servizo de Publicacións e Intercambio Científico, 2008. – 369 p. ; 21 cm. – (Vocabularios temáticos ; 4). - D.L. C 2458-2008. – ISBN 978-84-9887-018-3 1.Medicina �������������������������������������������������������������������������veterinaria-Diccionarios�������������������������������������������������. 2.Galego (Lingua)-Glosarios, vocabularios, etc. políglotas. I.Lombardero Fernández, Matilde. II.Rodríguez Rio, Xusto A. coord. III. Universidade de Santiago de Compostela. Servizo de Normalización Lingüística, coord. IV.Universidade de Santiago de Compostela. Servizo de Publicacións e Intercambio Científico, ed. V.Serie. 591.4(038)=699=60=20 Coordinador Xusto A. Rodríguez Río (Área de Terminoloxía. Servizo de Normalización Lingüística. Universidade de Santiago de Compostela) Autoras/res Matilde Lombardero Fernández (doutora en Veterinaria e profesora do Departamento de Anatomía e Produción Animal. -
Germ Cells …… Do Not Appear …… Until the Sixth Week of Development
Reproductive System Session 1 Origin of the Sexes Lecture 1 Development of Male and Female Reproductive System 1 The genital system LANGMAN”S Medical Embryology Indifferent Embryo • Between week 1 and 6, female and male embryos are phenotypically indistinguishable, even though the genotype (XX or XY) of the embryo is established at fertilization. • By week 12, some female and male characteristics of the external genitalia can be recognized. • By week 20, phenotypic differentiation is complete. 4 Indifferent Embryo • The indifferent gonads develop in a longitudinal elevation or ridge of intermediate mesoderm called the urogenital ridge ❑ Initially…. gonads (as a pair of longitudinal ridges, the genital or gonadal ridges). ❑ Epithelium + Mesenchyme. ❑ Germ cells …… do not appear …… until the sixth week of development. • Primordial germ cells arise from the lining cells in the wall of the yolk sac at weeks 3-4. • At week 4-6, primordial germ cells migrate into the indifferent gonad. ➢ Male germ cells will colonise the medullary region and the cortex region will atrophy. ➢ Female germ cells will colonise the cortex of the primordial gonad so the medullary cords do not develop. 5 6 The genital system 7 8 • Phenotypic differentiation is determined by the SRY gene (sex determining region on Y). • which is located on the short arm of the Y chromosome. The Sry gene encodes for a protein called testes- determining factor (TDF). 1. As the indifferent gonad develops into the testes, Leydig cells and Sertoli cells differentiate to produce Testosterone and Mullerian-inhibiting factor (MIF), respectively. 3. In the presence of TDF, testosterone, and MIF, the indifferent embryo will be directed to a male phenotype. -

Regulation and Roles of the Hyaluronan System in Mammalian Reproduction
REPRODUCTIONREVIEW Regulation and roles of the hyaluronan system in mammalian reproduction Ali A Fouladi-Nashta1, Kabir A Raheem1,2, Waleed F Marei1,3, Fataneh Ghafari1 and Geraldine M Hartshorne4 1Royal Veterinary College, Reproduction Research Group, Hawkshead Campus, Hatfield, UK, 2Department of Veterinary Surgery and Theriogenology, Michael Okpara University of Agriculture, Umudike, Nigeria, 3Department of Theriogenology, Faculty of Veterinary Medicine, Cairo University, Giza, Egypt and 4Warwick Medical School, University of Warwick, Coventry, UK and Centre for Reproductive Medicine, University Hospitals Coventry and Warwickshire NHS Trust, Coventry, UK Correspondence should be addressed to A A Fouladi-Nashta; Email: [email protected] Abstract Hyaluronan (HA) is a non-sulphated glycosaminoglycan polymer naturally occurring in many tissues and fluids of mammals, including the reproductive system. Its biosynthesis by HA synthase (HAS1–3) and catabolism by hyaluronidases (HYALs) are affected by ovarian steroid hormones. Depending upon its molecular size, HA functions both as a structural component of tissues in the form of high-molecular-weight HA or as a signalling molecule in the form of small HA molecules or HA fragments with effects mediated through interaction with its specific cell-membrane receptors. HA is produced by oocytes and embryos and in various segments of the reproductive system. This review provides information about the expression and function of members of the HA system, including HAS, HYALs and HA receptors. We examine their role in various processes from folliculogenesis through oocyte maturation, fertilisation and early embryo development, to pregnancy and cervical dilation, as well as its application in assisted reproduction technologies. Particular emphasis has been placed upon the role of the HA system in pre-implantation embryo development and embryo implantation, for which we propose a hypothetical sequential model. -

Abnormalities and Position-Converted
Medical Academy named after S. I. Georgievsky Chair of obstetrics, gynecology and perinatology # 1 Abnormalities of development and position of the internal female genitalia Livshyts I. V. PhD, Associate Professor • Congenital malformations of the female genital tract are defined as deviations from normal anatomy resulting from embryological maldevelopment of the Mullerian or paramesonephric ducts. • They represent a rather common benign condition with a prevalence of 4–7% • Müllerian malformations are frequently associated with abnormalities of the renal and axial skeletal systems Grimbizis et al., 2001; Saravelos et al., 2008; Chan et al., 2011a Early embryo development • Until 8 weeks' gestation, the human fetus is undifferentiated sexually and contains both male (wolffian) and female (müllerian) genital ducts. • Wolffian structures (in the male fetus) differentiate into the vas deferens, epididymis, and seminal vesicles. Wolffian (mesonephric) duct • In the female fetus, with the absence of testosterone secretion, the Wolffian duct regresses, but inclusions may persist. • The epoophoron and Skene's glands may be present. • Also, lateral to the wall of the vagina a Gartner's duct or cyst could develop as a remnant. Speroff L. et al., 2005 Müllerian (paramesonephric) ducts • Paired ducts of the embryo that run down the lateral sides of the urogenital ridge and terminate at the sinus tubercle in the primitive urogenital sinus. • In the female, without the influence of AMH, they will develop to form the fallopian tubes, uterus, cervix, and the upper one-third of the vagina. • In the absence of testosterone and dihydrotestosterone, the genital tubercle develops into the clitoris, and the labioscrotal folds do not fuse, leaving labia minora and majora. -

Clinical Pelvic Anatomy
SECTION ONE • Fundamentals 1 Clinical pelvic anatomy Introduction 1 Anatomical points for obstetric analgesia 3 Obstetric anatomy 1 Gynaecological anatomy 5 The pelvic organs during pregnancy 1 Anatomy of the lower urinary tract 13 the necks of the femora tends to compress the pelvis Introduction from the sides, reducing the transverse diameters of this part of the pelvis (Fig. 1.1). At an intermediate level, opposite A thorough understanding of pelvic anatomy is essential for the third segment of the sacrum, the canal retains a circular clinical practice. Not only does it facilitate an understanding cross-section. With this picture in mind, the ‘average’ of the process of labour, it also allows an appreciation of diameters of the pelvis at brim, cavity, and outlet levels can the mechanisms of sexual function and reproduction, and be readily understood (Table 1.1). establishes a background to the understanding of gynae- The distortions from a circular cross-section, however, cological pathology. Congenital abnormalities are discussed are very modest. If, in circumstances of malnutrition or in Chapter 3. metabolic bone disease, the consolidation of bone is impaired, more gross distortion of the pelvic shape is liable to occur, and labour is likely to involve mechanical difficulty. Obstetric anatomy This is termed cephalopelvic disproportion. The changing cross-sectional shape of the true pelvis at different levels The bony pelvis – transverse oval at the brim and anteroposterior oval at the outlet – usually determines a fundamental feature of The girdle of bones formed by the sacrum and the two labour, i.e. that the ovoid fetal head enters the brim with its innominate bones has several important functions (Fig. -

Recently Discovered Interstitial Cell Population of Telocytes: Distinguishing Facts from Fiction Regarding Their Role in The
medicina Review Recently Discovered Interstitial Cell Population of Telocytes: Distinguishing Facts from Fiction Regarding Their Role in the Pathogenesis of Diverse Diseases Called “Telocytopathies” Ivan Varga 1,*, Štefan Polák 1,Ján Kyseloviˇc 2, David Kachlík 3 , L’ubošDanišoviˇc 4 and Martin Klein 1 1 Institute of Histology and Embryology, Faculty of Medicine, Comenius University in Bratislava, 813 72 Bratislava, Slovakia; [email protected] (Š.P.); [email protected] (M.K.) 2 Fifth Department of Internal Medicine, Faculty of Medicine, Comenius University in Bratislava, 813 72 Bratislava, Slovakia; [email protected] 3 Institute of Anatomy, Second Faculty of Medicine, Charles University, 128 00 Prague, Czech Republic; [email protected] 4 Institute of Medical Biology, Genetics and Clinical Genetics, Faculty of Medicine, Comenius University in Bratislava, 813 72 Bratislava, Slovakia; [email protected] * Correspondence: [email protected]; Tel.: +421-90119-547 Received: 4 December 2018; Accepted: 11 February 2019; Published: 18 February 2019 Abstract: In recent years, the interstitial cells telocytes, formerly known as interstitial Cajal-like cells, have been described in almost all organs of the human body. Although telocytes were previously thought to be localized predominantly in the organs of the digestive system, as of 2018 they have also been described in the lymphoid tissue, skin, respiratory system, urinary system, meninges and the organs of the male and female genital tracts. Since the time of eminent German pathologist Rudolf Virchow, we have known that many pathological processes originate directly from cellular changes. Even though telocytes are not widely accepted by all scientists as an individual and morphologically and functionally distinct cell population, several articles regarding telocytes have already been published in such prestigious journals as Nature and Annals of the New York Academy of Sciences.