Clinical Pelvic Anatomy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Te2, Part Iii
TERMINOLOGIA EMBRYOLOGICA Second Edition International Embryological Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TE2, PART III Contents Caput V: Organogenesis Chapter 5: Organogenesis (continued) Systema respiratorium Respiratory system Systema urinarium Urinary system Systemata genitalia Genital systems Coeloma Coelom Glandulae endocrinae Endocrine glands Systema cardiovasculare Cardiovascular system Systema lymphoideum Lymphoid system Bibliographic Reference Citation: FIPAT. Terminologia Embryologica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, February 2017 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Embryologica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput V: ORGANOGENESIS Chapter 5: ORGANOGENESIS -

Chapter 28 *Lecture Powepoint
Chapter 28 *Lecture PowePoint The Female Reproductive System *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • The female reproductive system is more complex than the male system because it serves more purposes – Produces and delivers gametes – Provides nutrition and safe harbor for fetal development – Gives birth – Nourishes infant • Female system is more cyclic, and the hormones are secreted in a more complex sequence than the relatively steady secretion in the male 28-2 Sexual Differentiation • The two sexes indistinguishable for first 8 to 10 weeks of development • Female reproductive tract develops from the paramesonephric ducts – Not because of the positive action of any hormone – Because of the absence of testosterone and müllerian-inhibiting factor (MIF) 28-3 Reproductive Anatomy • Expected Learning Outcomes – Describe the structure of the ovary – Trace the female reproductive tract and describe the gross anatomy and histology of each organ – Identify the ligaments that support the female reproductive organs – Describe the blood supply to the female reproductive tract – Identify the external genitalia of the female – Describe the structure of the nonlactating breast 28-4 Sexual Differentiation • Without testosterone: – Causes mesonephric ducts to degenerate – Genital tubercle becomes the glans clitoris – Urogenital folds become the labia minora – Labioscrotal folds -

The Cyclist's Vulva
The Cyclist’s Vulva Dr. Chimsom T. Oleka, MD FACOG Board Certified OBGYN Fellowship Trained Pediatric and Adolescent Gynecologist National Medical Network –USOPC Houston, TX DEPARTMENT NAME DISCLOSURES None [email protected] DEPARTMENT NAME PRONOUNS The use of “female” and “woman” in this talk, as well as in the highlighted studies refer to cis gender females with vulvas DEPARTMENT NAME GOALS To highlight an issue To discuss why this issue matters To inspire future research and exploration To normalize the conversation DEPARTMENT NAME The consensus is that when you first start cycling on your good‐as‐new, unbruised foof, it is going to hurt. After a “breaking‐in” period, the pain‐to‐numbness ratio becomes favourable. As long as you protect against infection, wear padded shorts with a generous layer of chamois cream, no underwear and make regular offerings to the ingrown hair goddess, things are manageable. This is wrong. Hannah Dines British T2 trike rider who competed at the 2016 Summer Paralympics DEPARTMENT NAME MY INTRODUCTION TO CYCLING Childhood Adolescence Adult Life DEPARTMENT NAME THE CYCLIST’S VULVA The Issue Vulva Anatomy Vulva Trauma Prevention DEPARTMENT NAME CYCLING HAS POSITIVE BENEFITS Popular Means of Exercise Has gained popularity among Ideal nonimpact women in the past aerobic exercise decade Increases Lowers all cause cardiorespiratory mortality risks fitness DEPARTMENT NAME Hermans TJN, Wijn RPWF, Winkens B, et al. Urogenital and Sexual complaints in female club cyclists‐a cross‐sectional study. J Sex Med 2016 CYCLING ALSO PREDISPOSES TO VULVAR TRAUMA • Significant decreases in pudendal nerve sensory function in women cyclists • Similar to men, women cyclists suffer from compression injuries that compromise normal function of the main neurovascular bundle of the vulva • Buller et al. -

Female Perineum Doctors Notes Notes/Extra Explanation Please View Our Editing File Before Studying This Lecture to Check for Any Changes
Color Code Important Female Perineum Doctors Notes Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives At the end of the lecture, the student should be able to describe the: ✓ Boundaries of the perineum. ✓ Division of perineum into two triangles. ✓ Boundaries & Contents of anal & urogenital triangles. ✓ Lower part of Anal canal. ✓ Boundaries & contents of Ischiorectal fossa. ✓ Innervation, Blood supply and lymphatic drainage of perineum. Lecture Outline ‰ Introduction: • The trunk is divided into 4 main cavities: thoracic, abdominal, pelvic, and perineal. (see image 1) • The pelvis has an inlet and an outlet. (see image 2) The lowest part of the pelvic outlet is the perineum. • The perineum is separated from the pelvic cavity superiorly by the pelvic floor. • The pelvic floor or pelvic diaphragm is composed of muscle fibers of the levator ani, the coccygeus muscle, and associated connective tissue. (see image 3) We will talk about them more in the next lecture. Image (1) Image (2) Image (3) Note: this image is seen from ABOVE Perineum (In this lecture the boundaries and relations are important) o Perineum is the region of the body below the pelvic diaphragm (The outlet of the pelvis) o It is a diamond shaped area between the thighs. Boundaries: (these are the external or surface boundaries) Anteriorly Laterally Posteriorly Medial surfaces of Intergluteal folds Mons pubis the thighs or cleft Contents: 1. Lower ends of urethra, vagina & anal canal 2. External genitalia 3. Perineal body & Anococcygeal body Extra (we will now talk about these in the next slides) Perineum Extra explanation: The perineal body is an irregular Perineal body fibromuscular mass. -

Vocabulario De Morfoloxía, Anatomía E Citoloxía Veterinaria
Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) Servizo de Normalización Lingüística Universidade de Santiago de Compostela COLECCIÓN VOCABULARIOS TEMÁTICOS N.º 4 SERVIZO DE NORMALIZACIÓN LINGÜÍSTICA Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) 2008 UNIVERSIDADE DE SANTIAGO DE COMPOSTELA VOCABULARIO de morfoloxía, anatomía e citoloxía veterinaria : (galego-español- inglés) / coordinador Xusto A. Rodríguez Río, Servizo de Normalización Lingüística ; autores Matilde Lombardero Fernández ... [et al.]. – Santiago de Compostela : Universidade de Santiago de Compostela, Servizo de Publicacións e Intercambio Científico, 2008. – 369 p. ; 21 cm. – (Vocabularios temáticos ; 4). - D.L. C 2458-2008. – ISBN 978-84-9887-018-3 1.Medicina �������������������������������������������������������������������������veterinaria-Diccionarios�������������������������������������������������. 2.Galego (Lingua)-Glosarios, vocabularios, etc. políglotas. I.Lombardero Fernández, Matilde. II.Rodríguez Rio, Xusto A. coord. III. Universidade de Santiago de Compostela. Servizo de Normalización Lingüística, coord. IV.Universidade de Santiago de Compostela. Servizo de Publicacións e Intercambio Científico, ed. V.Serie. 591.4(038)=699=60=20 Coordinador Xusto A. Rodríguez Río (Área de Terminoloxía. Servizo de Normalización Lingüística. Universidade de Santiago de Compostela) Autoras/res Matilde Lombardero Fernández (doutora en Veterinaria e profesora do Departamento de Anatomía e Produción Animal. -

MR Imaging of Vaginal Morphology, Paravaginal Attachments and Ligaments
MR imaging of vaginal morph:ingynious 05/06/15 10:09 Pagina 53 Original article MR imaging of vaginal morphology, paravaginal attachments and ligaments. Normal features VITTORIO PILONI Iniziativa Medica, Diagnostic Imaging Centre, Monselice (Padova), Italy Abstract: Aim: To define the MR appearance of the intact vaginal and paravaginal anatomy. Method: the pelvic MR examinations achieved with external coil of 25 nulliparous women (group A), mean age 31.3 range 28-35 years without pelvic floor dysfunctions, were compared with those of 8 women who had cesarean delivery (group B), mean age 34.1 range 31-40 years, for evidence of (a) vaginal morphology, length and axis inclination; (b) perineal body’s position with respect to the hymen plane; and (c) visibility of paravaginal attachments and lig- aments. Results: in both groups, axial MR images showed that the upper vagina had an horizontal, linear shape in over 91%; the middle vagi- na an H-shape or W-shape in 74% and 26%, respectively; and the lower vagina a U-shape in 82% of cases. Vaginal length, axis inclination and distance of perineal body to the hymen were not significantly different between the two groups (mean ± SD 77.3 ± 3.2 mm vs 74.3 ± 5.2 mm; 70.1 ± 4.8 degrees vs 74.04 ± 1.6 degrees; and +3.2 ± 2.4 mm vs + 2.4 ± 1.8 mm, in group A and B, respectively, P > 0.05). Overall, the lower third vaginal morphology was the less easily identifiable structure (visibility score, 2); the uterosacral ligaments and the parau- rethral ligaments were the most frequently depicted attachments (visibility score, 3 and 4, respectively); the distance of the perineal body to the hymen was the most consistent reference landmark (mean +3 mm, range -2 to + 5 mm, visibility score 4). -
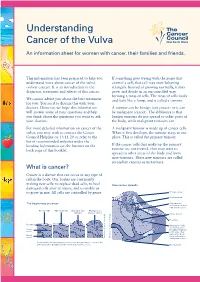
Understanding Cancer of the Vulva
Understanding Cancer of the Vulva An information sheet for women with cancer, their families and friends. This information has been prepared to help you If something goes wrong with the genes that understand more about cancer of the vulva control a cell, that cell may start behaving (vulvar cancer). It is an introduction to the strangely. Instead of growing normally, it may diagnosis, treatment and effects of this cancer. grow and divide in an uncontrolled way, forming a mass of cells. The mass of cells looks We cannot advise you about the best treatment and feels like a lump, and is called a tumour. for you. You need to discuss this with your doctors. However, we hope this information A tumour can be benign (not cancer) or it can will answer some of your questions and help be malignant (cancer). The difference is that you think about the questions you want to ask benign tumours do not spread to other parts of your doctors. the body, while malignant tumours can. For more detailed information on cancer of the A malignant tumour is made up of cancer cells. vulva, you may wish to contact the Cancer When it first develops, the tumour stays in one Council Helpline on 13 11 20 or refer to the place. This is called the primary tumour. list of recommended websites under the heading Information on the Internet on the If the cancer cells that make up the primary back page of this booklet. tumour are not treated, they may start to spread to other areas of the body and form new tumours. -

Femoral Nerve Dimensions at the Inguinal Ligament and Inguinal Crease Levels: Implications for Femoral Nerve Block
Original article http://dx.doi.org/10.4322/jms.062413 Femoral nerve dimensions at the inguinal ligament and inguinal crease levels: implications for femoral nerve block OYEDUN, O. S.1*, RUKEWE, A.2 and FATIREGUN, A.3 1Gross Anatomy Lab, Department of Anatomy, Faculty of Basic Medical Sciences, University of Ibadan, +234 Ibadan, Oyo State, Nigéria 2Anaesthesia Unit, Accident and Emergency Department, University College Hospital, +234 Ibadan, Oyo State, Nigéria 3Department of Epidemiology and Medical Statistics, Faculty of Public Health, University of Ibadan, +234 Ibadan, Oyo State, Nigéria *E-mail: [email protected] Abstract Introduction: Femoral nerve block, when used solely or as a supplement to general anaesthesia, provides anaesthesia and analgesia to the anterior thigh. In spite of its established benefits, femoral nerve block is still underutilized in Nigeria. Our objective was to study the dimensions of femoral nerve at the level of the inguinal ligament and inguinal crease using a cadaveric model; no such data exists in Nigeria. Materials and Methods: Using 7 adult human cadavers (6 males and 1 female), the depth and thickness of the femoral nerve were measured at the levels of inguinal ligament and inguinal crease. The spatial relationship of femoral nerve to the surrounding structures was also observed. Result: The study showed a significantly wider thickness and shorter depth of the femoral nerve at the level of inguinal crease relative to inguinal ligament. Conclusion: We concluded that in centers where ultrasound and neurostimulation techniques for femoral nerve block in Nigerians are unavailable, the inguinal crease level where the femoral nerve is more superficial and wider in thickness would be the landmark of choice compared to the inguinal ligament level. -

Female Inguinal Hernia – Conservatively Treated As Labial Swelling for a Long Time-A Case Report Shabnam Na, Alam Hb, Talukder Mrhc, Humayra Zud, Ahmed Ahmte
Case Report Female Inguinal Hernia – Conservatively Treated as Labial Swelling for a Long Time-A Case Report Shabnam Na, Alam Hb, Talukder MRHc, Humayra ZUd, Ahmed AHMTe Abstract Inguinal hernia in females is quite uncommon compared to males. However, in female it may pose both a diagnostic as well as surgical challenge to the attending surgeon. Awareness of anatomy of the region and all the possible contents is essential to prevent untoward complications. Here we are presenting a case of indirect inguinal hernia in a 25 years old women and how she was diagnosed and ultimately managed. Key words: Inguinal hernia, females (BIRDEM Med J 2018; 8(1): 81-82 ) Introduction Case Report Inguinal hernia in female is relatively uncommon as A 25-year-old female, non obese, mother of one child, compared to males. The incidence of inguinal hernia in delivered vaginal (NVD) presented with a swelling in females is 1.9%1 . Obesity, pregnancy and operative the left groin for 7 years. Initially she presented to procedures have been shown to be risk factors that different gynecologists with labial swelling. They treated commonly contribute to the formation of inguinal her conservatively. As she was not improving, she finally hernia2. Surgical management in women is similar to presented to surgeon. She gave history of left groin swelling extending down to labia majora which initially that in men. However a wide variety of presentations appeared during straining but later on it persisted all may add to the confusion in diagnosing inguinal hernia the time. In lying position, the swelling disappeared. -

Sportsmans Groin: the Inguinal Ligament and the Lloyd Technique
Rennie, WJ and Lloyd, DM. Sportsmans Groin: The Inguinal Ligament and the Lloyd Technique. Journal of the Belgian Society of Radiology. 2017; 101(S2): 16, pp. 1–4. DOI: https://doi.org/10.5334/jbr-btr.1404 OPINION ARTICLE Sportsmans Groin: The Inguinal Ligament and the Lloyd Technique WJ Rennie and DM Lloyd Groin pain is a catch all phrase used to define a common set of symptoms that affect many individuals. It is a common condition affecting sportsmen and women (1, 2) and is often referred to as the sportsman groin (SG). Multiple surgical operations have been developed to treat these symptoms yet no definitive imaging modalities exist to diagnose or predict prognosis. This article aims to discuss the anatomy of the groin, suggest a biomechanical pathophysiology and outline a logical surgical solution to treat the underlying pathology. A systematic clinical and imaging approach with inguinal ligament and pubic specific MRI assessment, can result in accurate selection for intervention. Close correlation with clinical examination and imaging in series is recommended to avoid misinterpretation of chronic changes in athletes. Keywords: Groin pain; Inguinal Ligament; MRI; Surgery; Lloyd release Introduction from SG is due to altered biomechanics, with specific pain Groin pain is a catch all phrase used to define a common symptoms that differ from those caused by inguinal or set of symptoms that affect many individuals. It is a com- femoral hernias. mon condition affecting sportsmen and women [1, 2] and is often referred to as the sportsman groin (SG). Multiple Anatomy of Sportsman’s Groin surgical operations have been developed to treat these The anatomical central structure in the groin is the pubic symptoms, yet no definitive imaging modalities exist to bone. -

Describe the Anatomy of the Inguinal Canal. How May Direct and Indirect Hernias Be Differentiated Anatomically
Describe the anatomy of the inguinal canal. How may direct and indirect hernias be differentiated anatomically. How may they present clinically? Essentially, the function of the inguinal canal is for the passage of the spermatic cord from the scrotum to the abdominal cavity. It would be unreasonable to have a single opening through the abdominal wall, as contents of the abdomen would prolapse through it each time the intraabdominal pressure was raised. To prevent this, the route for passage must be sufficiently tight. This is achieved by passing through the inguinal canal, whose features allow the passage without prolapse under normal conditions. The inguinal canal is approximately 4 cm long and is directed obliquely inferomedially through the inferior part of the anterolateral abdominal wall. The canal lies parallel and 2-4 cm superior to the medial half of the inguinal ligament. This ligament extends from the anterior superior iliac spine to the pubic tubercle. It is the lower free edge of the external oblique aponeurosis. The main occupant of the inguinal canal is the spermatic cord in males and the round ligament of the uterus in females. They are functionally and developmentally distinct structures that happen to occur in the same location. The canal also transmits the blood and lymphatic vessels and the ilioinguinal nerve (L1 collateral) from the lumbar plexus forming within psoas major muscle. The inguinal canal has openings at either end – the deep and superficial inguinal rings. The deep (internal) inguinal ring is the entrance to the inguinal canal. It is the site of an outpouching of the transversalis fascia. -

Female Reproductive System Chapter 28
The Female Reproductive System Chapter 28 • Female Reproductive System Anatomy • Oogenesis and the Sexual Cycle – Ovarian Cycle – Menstrual Cycle Female Reproductive System Functions: • Produce female sex hormones and gametes • Provide nutrition for fetal development • Nourish the infant after birth The Uterus • Thick-walled, pear-shaped, muscular chamber opening into vagina. • Cervix is the rounded opening of the uterus. • Two uterine tubes (also called Fallopian tubes or oviducts) branch off the uterus and terminate near the ovaries. Uterine Tubes • Also called Fallopian Tubes or Oviducts • Open-ended, muscular tube lined with secretory cells and ciliated cells that sweep secretions and peritoneal fluid towards the uterus. • Uterine Tube Regions: – narrow isthmus near the uterus – middle portion is the ampulla – flared distally into infundibulum with fimbriae • Fertilization usually occurs in ampulla or isthmus Epithelium lining the uterine tube consists of ciliated cells, goblet cells and other secretory cells. Cilia move peritoneal fluid and uterine tube secretions towards the uterus. Cervix and Vagina normally have a stratified squamous epithelium Test developed by Dr. G.N. Papanicolaou can detect cervical cancer by identifying transformed squamous cells. normal PAP smear abnormal PAP smear Histology of the Uterus • Perimetrium is the external serosa layer • Myometrium is the middle muscular layer – 1 cm thick in nonpregnant uterus – composed of smooth muscle – produces labor contractions to expel fetus during childbirth • Endometrium – simple columnar epithelium with tubular glands – stratum functionalis is superficial layer that is shed with each menstrual cycle – stratum basalis is deeper layer that regenerates a new stratum functionalis with each menstrual cycle Ovary • Ovaries produce oocytes and female hormones.