Studies of the Function of the Human Pylorus : and Its Role in The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

4L Eosinophilic Granuloma of Gastro-Intestinal Tract Caused by Herring Parasite Eustoma Rotundatum
BsrrmsH 2 May 1964 MEDICAL JOURNAL 1141 4L Eosinophilic Granuloma of Gastro-intestinal Tract Caused by Herring Parasite Eustoma rotundatum B. STERRY ASHBY,* M.B., F.R.C.S.; P. J. APPLETONt M.B., B.S. IAN DAWSON,4 M.D., M.R.C.P. Brit. med.JY., 1964, 1, 1141-1145 For over 25 years sporadic reports have been appearing in the came from many countries in many different parts of the world. literature of cases of eosinophilic granuloma arising in various The essential details of these cases are recorded in Table I parts of the gastro-intestinal tract. Kaiiser (1937) described and Fig. 1. the first cases. In a search of the literature, which although The one feature common to all these case reports is the extensive is not claimed to be exhaustive, 47 papers were microscopical appearance of the lesion. No matter which part found, describing a total of 89 cases. They occurred through- of the alimentary tract is involved, the histological description out the alimentary tract from pharynx to rectum, though the is the same-an oedematous connective-tissue stroma with an majority were in the stomach and small intestine, and they increase of capillaries and lymphatics, and showing a massive diffuse eosinophil-cell infiltration, usually confined to the sub- * Surgical Registrar, Westminster Hospital and Medical School London. the muscularis mucosae and t House-Surgeon, Westminster Hospital and Medical School, Iondon. mucosa but sometimes splitting t Reader in Pathology, Westminster Hospital and Medical School, spreading into the muscle layer. The mucosa is almost always London. intact. -
Nbde Part 2 Decks and Remembed-Arroz Con Mango
ARROZ CON MANGO Dear friends, these are remembered/repeated questions (RQs) and answers I COPIED and PASTED from different discussions on Facebook. I feel sorry because I couldn’t organize the file the way I wanted but I hope it helps. Probably you’ll find some wrong answers in this file, but PLEASE … DO NOT CRITICIZE! Find out the right answer, learn it, share it, PASS your test and BE HAPPY J I wish you all the best GOD BLESS YOU! PAITO 1. All of the following are adverse effects of opioids except? diarrhea and somnolence 2. Advantage of osteogenesis distraction is? less relapse, large movements 3. An investigation that is not accurate but consistent is: reliability 4. Remineralized enamel is rough and cavitation? Dark hard and opaque 5. Characteristics of a child with autism - repetitive action, sensitive to light and noise 6. S,z,che sounds : Teeth barely touching – True 7. Something about bio-transformation, more polar and less lipid soluble? - True 8. How much of he population has herpes? 80% - (65-90% worldwide; 80-85% USA) More than 3.7 billion people under the age of 50 – or 67% of the population – are infected with herpes simplex virus type 1 (HSV-1), according to WHO's first global estimates of HSV-1 infection published today in the journal PLOS ONE. 9. Steps of plaque formation: pellicle, biofilm, materia alba, plaque 10. Dose of hydrocortisone taken per year that will indicate have adrenal insufficiency and need supplement dose for surgery - 20 mg 2 weeks for 2 years 11. Rpd clasp breakage due to what? Work hardening 12. -
Surgical Anatomy of the Infratemporal Fossa Surgical Anatomy of the Infratemporal Fossa
Surgical Anatomy of the Infratemporal Fossa Surgical Anatomy of the Infratemporal Fossa John D.Langdon Professor and Head of Department Department of Oral and Maxillofacial Surgery King’s College London, UK Barry K.B.Berkovitz Reader in Anatomy Division of Anatomy, Cell and Human Biology King’s College London, UK Bernard J.Moxham Professor of Anatomy and Head of Teaching in Biosciences Cardiff School of Biosciences Cardiff University, UK MARTIN DUNITZ © 2003 Martin Dunitz, a member of the Taylor & Francis Group First published in the United Kingdom in 2003 by Martin Dunitz, Taylor & Francis Group plc, 11 New Fetter Lane, London EC4P 4EE Tel.: +44 (0) 20 7583 9855 Fax.: +44 (0) 20 7842 2298 E-mail: [email protected] Website: http://www.dunitz.co.uk This edition published in the Taylor & Francis e-Library, 2005. “To purchase your own copy of this or any of Taylor & Francis or Routledge’s collection of thousands of eBooks please go to www.eBookstore.tandf.co.uk.” All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior permission of the publisher or in accordance with the provisions of the Copyright, Designs and Patents Act 1988 or under the terms of any licence permitting limited copying issued by the Copyright Licensing Agency, 90 Tottenham Court Road, London W1P OLP. Although every effort has been made to ensure that all owners of copyright material have been acknowledged in this publication, we would be glad to acknowledge in subsequent reprints or editions any omissions brought to our attention. -

ODONTOGENTIC INFECTIONS Infection Spread Determinants
ODONTOGENTIC INFECTIONS The Host The Organism The Environment In a state of homeostasis, there is Peter A. Vellis, D.D.S. a balance between the three. PROGRESSION OF ODONTOGENIC Infection Spread Determinants INFECTIONS • Location, location , location 1. Source 2. Bone density 3. Muscle attachment 4. Fascial planes “The Path of Least Resistance” Odontogentic Infections Progression of Odontogenic Infections • Common occurrences • Periapical due primarily to caries • Periodontal and periodontal • Soft tissue involvement disease. – Determined by perforation of the cortical bone in relation to the muscle attachments • Odontogentic infections • Cellulitis‐ acute, painful, diffuse borders can extend to potential • fascial spaces. Abscess‐ chronic, localized pain, fluctuant, well circumscribed. INFECTIONS Severity of the Infection Classic signs and symptoms: • Dolor- Pain Complete Tumor- Swelling History Calor- Warmth – Chief Complaint Rubor- Redness – Onset Loss of function – Duration Trismus – Symptoms Difficulty in breathing, swallowing, chewing Severity of the Infection Physical Examination • Vital Signs • How the patient – Temperature‐ feels‐ Malaise systemic involvement >101 F • Previous treatment – Blood Pressure‐ mild • Self treatment elevation • Past Medical – Pulse‐ >100 History – Increased Respiratory • Review of Systems Rate‐ normal 14‐16 – Lymphadenopathy Fascial Planes/Spaces Fascial Planes/Spaces • Potential spaces for • Primary spaces infectious spread – Canine between loose – Buccal connective tissue – Submandibular – Submental -

GI Motility-I (Deglutition and Motor Functions of Stomach)
Lecture series Gastrointestinal tract Professor Shraddha Singh, Department of Physiology, KGMU, Lucknow GASTROINTESTINAL MOTILITY-1 (Deglutation and motor function of stomach) Mastication (Chewing) - the anterior teeth (incisors) providing a strong cutting action and the posterior teeth (molars), a grinding action – canine tearing - All the jaw muscles working together can close the teeth with a force as great as 25 Kg on the incisors and 90 Kg on the molars. - Most of the muscles of chewing are innervated by the motor branch of the 5th cranial nerve, and the chewing process is controlled by nuclei in the brain stem. - Stimulation of areas in the hypothalamus, amygdala, and even the cerebral cortex near the sensory areas for taste and smell can often cause chewing Chewing Reflex - The presence of a bolus of food in the mouth at first initiates reflex inhibition of the muscles of mastication, which allows the lower jaw to drop. ↓ - The drop in turn initiates a stretch reflex of the jaw muscles that leads to rebound contraction ↓ - raises the jaw to cause closure of the teeth ↓ - compresses the bolus again against the linings of the mouth, which inhibits the jaw muscles once again Chewing Reflex - most fruits and raw vegetables because these have indigestible cellulose membranes around their nutrient portions that must be broken before the food can be digested - Digestive enzymes act only on the surfaces of food particles - grinding the food to a very fine particulate consistency prevents excoriation of the GIT (Stomach) Swallowing (Deglutition) -

The Arrest of Intestinal Epithelial ' Turnover' by the Use of X-Irradiation
Gut, 1962, 3, 26 Gut: first published as 10.1136/gut.3.1.26 on 1 March 1962. Downloaded from The arrest of intestinal epithelial ' turnover' by the use of x-irradiation G. WIERNIK, R. G. SHORTER, AND B. CREAMER From St. Thomas's Hospital and Medical School, London sYNoPsIs Mitotic activity and hence cell turnover has been abolished by x-irradiation with 1,000 r. in segments of the rat's gut. The whole stomach, the ascending colon, and 5 cm. of jejunum and ileum were irradiated and the changes observed histologically up to three days. Cessation of cell turnover in the small intestine is followed by cell death and desquamation within 24 hours, leading to denudation of the epithelium and collapse of villous structure. The pylorus and colon showed similar but less marked changes. In contrast the fundus and body of the stomach were unaffected by the absence of mitosis over a period of three days. It is concluded that cell turnover is, in part, necessary to maintain the mucosal structure, particularly the villous pattern in the small intestine. The gastro-intestinal epithelium is a dynamic METHODS structure. Although it appears an intact and lush Wistar rats of either sex weighing 200 g. were used. The membrane to histological examination, it is being animals were anaesthetized with intraperitoneal pento- continuously replaced and desquamated extremely barbitone sodium B.P. The segment of gut to be irradiated quickly. This replacement ofcells results from intense was delivered through an abdominal incision and its http://gut.bmj.com/ division in the crypts, the cells so formed migrating extent marked by fine silk loops. -

The Gallbladder
The Gallbladder Anatomy of the gallbladder Location: Right cranial abdominal quadrant. In the gallbladder fossa of the liver. o Between the quadrate and right medial liver lobes. Macroscopic: Pear-shaped organ Fundus, body and neck. o Neck attaches, via a short cystic duct, to the common bile duct. Opens into the duodenum via sphincter of Oddi at the major duodenal papilla. Found on the mesenteric margin of orad duodenum. o 3-6 cm aboral to pylorus. 1-2cm of distal common bile duct runs intramural. Species differences: Dogs: o Common bile duct enters at major duodenal papilla. Adjacent to pancreatic duct (no confluence prior to entrance). o Accessory pancreatic duct enters at minor duodenal papilla. ± 2 cm aboral to major duodenal papilla. MAJOR conduit for pancreatic secretions. Cats: o Common bile duct and pancreatic duct converge before opening at major duodenal papilla. Thus, any surgical procedure that affects the major duodenal papilla can affect the exocrine pancreatic secretions in cats. o Accessory pancreatic duct only seen in 20% of cats. 1 Gallbladder wall: 5 histologically distinct layers. From innermost these include: o Epithelium, o Submucosa (consisting of the lamina propria and tunica submucosa), o Tunica muscularis externa, o Tunica serosa (outermost layer covers gallbladder facing away from the liver), o Tunica adventitia (outermost layer covers gallbladder facing towards the liver). Blood supply: Solely by the cystic artery (derived from the left branch of the hepatic artery). o Susceptible to ischaemic necrosis should its vascular supply become compromised. Function: Storage reservoir for bile o Concentrated (up to 10-fold), acidified (through epithelial acid secretions) and modified (by the addition of mucin and immunoglobulins) before being released into the gastrointestinal tract at the major duodenal. -

Effect of Chronic Ethanol Ingestion on Enterocyte Turnover in Rat Small Intestine
Gut: first published as 10.1136/gut.28.1.52 on 1 January 1987. Downloaded from Gut, 1987, 28, 52-55 Effect of chronic ethanol ingestion on enterocyte turnover in rat small intestine R MAZZANTI AND W J JENKINS From the Department of' Medicine, Royal Free Hospital School of Medicine, Rowland Hill Street, Londlon SUMMARY Whether chronic ethanol ingestion significantly damages the small intestine remains controversial. To clarify this we have analysed the morphology of the small intestinal epithelium and quantified its renewal in chronically ethanol fed rats. Twenty adult male rats were pair fed for 28 days a nutritionally adequate liquid diet containing either ethanol as 36% of total calories or an isocaloric diet in which fat substituted for ethanol. Crypt cell production rate was determined in the jejunum and ileum by the metaphase arrest method. Weight gain and small intestinal morphology were similar in ethanol fed and control rats, but enterocyte turnover was significantly reduced in the jejunum (p<O.05) and ileum (p<0.0l) of the ethanol fed rats. This effect of ethanol on the small intestine is probably systemic rather than local, because the changes in jejunum and ileum were similar, and it may contribute to the development of malnutrition in chronic alcoholics. A variety of changes in intestinal function have Methods been reported after acute or habitual alcohol consumption.' Impaired absorption of vitamins,25 ANIMALS sugars6 7 and amino acids8 9 has been shown in Twenty adult male Sprague-Dawley rats, which http://gut.bmj.com/ the presence of ethanol, and the chronic consump- initially weighed between 210 g and 310 g, were tion of ethanol is often associated with malnutrition maintained in single cages on a 12 hour light-dark and diarrhoea, but whether these are caused by cycle at 21 ±1°C room temperature. -
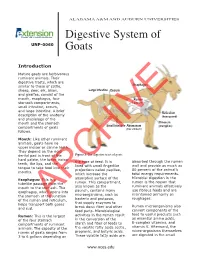
Digestive System of Goats 3 References
ALABAMA A&M AND AUBURN UNIVERSITIES Digestive System of UNP-0060 Goats Introduction Mature goats are herbivorous ruminant animals. Their digestive tracts, which are similar to those of cattle, Esophagus sheep, deer, elk, bison, Large Intestine Cecum and giraffes, consist of the mouth, esophagus, four Rumen stomach compartments, (paunch) small intestine, cecum, and large intestine. A brief Reticulum description of the anatomy (honeycomb) and physiology of the mouth and the stomach Omasum Small Intestine Abomasum (manyplies) compartments of goats (true stomach) follows. Mouth: Like other ruminant animals, goats have no upper incisor or canine teeth. They depend on the rigid dental pad in front of the Figure 1. The digestive tract of goats. hard palate, the lower incisor the type of feed. It is absorbed through the rumen teeth, the lips, and the lined with small fingerlike wall and provide as much as tongue to take food into their projections called papillae, 80 percent of the animal’s mouths. which increase the total energy requirements. Microbial digestion in the Esophagus: This is a absorptive surface of the rumen is the reason that tubelike passage from the rumen. This compartment, ruminant animals effectively mouth to the stomach. The also known as the use fibrous feeds and are esophagus, which opens into paunch, contains many maintained primarily on the stomach at the junction microorganisms, such as roughages. of the rumen and reticulum, bacteria and protozoa, helps transport bothARCHIVE gases that supply enzymes to Rumen microorganisms also and cud. break down fiber and other feed parts. Microbiological convert components of the feed to useful products such Rumen: This is the largest activities in the rumen result as essential amino acids, of the four stomach in the conversion of the B-complex vitamins, and compartments of ruminant starch and fiber of feeds to vitamin K. -

Normal Gastrointestinal Motility and Function Esophagus
Normal Gastrointestinal Motility and Function "Motility" is an unfamiliar word to many people; it is used primarily to describe the contraction of the muscles in the gastrointestinal tract. Because the gastrointestinal tract is a circular tube, when these muscles contract, they close off the tube or make the opening inside smaller - they squeeze. These muscles can contract in a synchronized way to move the food in one direction (usually downstream, but occasionally upstream for short distances); this is called peristalsis. If you looked at the intestine, you would see a ring of contraction that moves along pushing contents ahead of it. At other times, the muscles in adjacent parts of the gastrointestinal tract squeeze more or less independently of each other: this has the effect of mixing the contents but not moving them up or down. Both kinds of contraction patterns are called motility. The gastrointestinal tract is divided into four distinct parts: the esophagus, stomach, small intestine, and large intestine (colon). They are separated from each other by special muscles called sphincters which normally stay tightly closed and which regulate the movement of food and food residues from one part to another. Each part of the gastrointestinal tract has a unique function to perform in digestion, and as a result each part has a distinct type of motility and sensation. When motility or sensations are not appropriate for performing this function, they cause symptoms such as bloating, vomiting, constipation, or diarrhea which are associated with subjective sensations such as pain, bloating, fullness, and urgency to have a bowel movement. -

Complex Odontogenic Infections
Complex Odontogenic Infections Larry ). Peterson CHAPTEROUTLINE FASCIAL SPACE INFECTIONS Maxillary Spaces MANDIBULAR SPACES Secondary Fascial Spaces Cervical Fascial Spaces Management of Fascial Space Infections dontogenic infections are usually mild and easily and causes infection in the adjacent tissue. Whether or treated by antibiotic administration and local sur- not this becomes a vestibular or fascial space abscess is 0 gical treatment. Abscess formation in the bucco- determined primarily by the relationship of the muscle lingual vestibule is managed by simple intraoral incision attachment to the point at which the infection perfo- and drainage (I&D) procedures, occasionally including rates. Most odontogenic infections penetrate the bone dental extraction. (The principles of management of rou- in such a way that they become vestibular abscesses. tine odontogenic infections are discussed in Chapter 15.) On occasion they erode into fascial spaces directly, Some odontogenic infections are very serious and require which causes a fascial space infection (Fig. 16-1). Fascial management by clinicians who have extensive training spaces are fascia-lined areas that can be eroded or dis- and experience. Even after the advent of antibiotics and tended by purulent exudate. These areas are potential improved dental health, serious odontogenic infections spaces that do not exist in healthy people but become still sometimes result in death. These deaths occur when filled during infections. Some contain named neurovas- the infection reaches areas distant from the alveolar cular structures and are known as coinpnrtments; others, process. The purpose of this chapter is to present which are filled with loose areolar connective tissue, are overviews of fascial space infections of the head and neck known as clefts. -

Effects of Microflora on the Dimensions of Enterocyte Microvilli in the Rat J.-C
Effects of microflora on the dimensions of enterocyte microvilli in the rat J.-C. Meslin, E. Sacquet, S. Delpal To cite this version: J.-C. Meslin, E. Sacquet, S. Delpal. Effects of microflora on the dimensions of enterocyte microvilli in the rat. Reproduction Nutrition Développement, 1984, 24 (3), pp.307-314. hal-00898154 HAL Id: hal-00898154 https://hal.archives-ouvertes.fr/hal-00898154 Submitted on 1 Jan 1984 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Effects of microflora on the dimensions of enterocyte microvilli in the rat J.-C. MESLIN, E. SACQUET S. DELPAL Station de Recherches de Nutrition, /./V./7./! 78350 Jouy-en-Josas, France. (*) Laboratoire des Animaux sans Germes, CNRS, lNRA, 78350 Jouy-en-Josas, France. Summary. The length and diameter of enterocyte microvilli at mid-villus position were measured on electron-micrographs. The duodenum, jejunum and ileum of axenic (germfree) and holoxenic (conventional) inbred rats fed the same diet have been studied. The microvilli were significantly shorter in all these intestinal regions when the microflora was present. The decrease in microvillus length (due to the presence of microflora), expressed as a percentage of the length in axenic rat, was 5 % in the duodenum, 9 % in the jejunum and 18 % in the ileum.