9.14 MIT Spring 2002 Class #24: Neocortex, Introduction. Readings
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Post-Stroke Movement Disorders: Report of 56 Patients F Alarco´N, J C M Zijlmans, G Duen˜As, N Cevallos
1568 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.2003.011874 on 15 October 2004. Downloaded from PAPER Post-stroke movement disorders: report of 56 patients F Alarco´n, J C M Zijlmans, G Duen˜as, N Cevallos ............................................................................................................................... J Neurol Neurosurg Psychiatry 2004;75:1568–1574. doi: 10.1136/jnnp.2003.011874 Background: Although movement disorders that occur following a stroke have long been recognised in short series of patients, their frequency and clinical and imaging features have not been reported in large series of patients with stroke. Methods: We reviewed consecutive patients with involuntary abnormal movements (IAMs) following a stroke who were included in the Eugenio Espejo Hospital Stroke Registry and they were followed up for at least one year after the onset of the IAM. We determined the clinical features, topographical correlations, See end of article for authors’ affiliations and pathophysiological implications of the IAMs. ....................... Results: Of 1500 patients with stroke 56 developed movement disorders up to one year after the stroke. Patients with chorea were older and the patients with dystonia were younger than the patients with other Correspondence to: Dr. F Alarco´n, Department IAMs. In patients with isolated vascular lesions without IAMs, surface lesions prevailed but patients with of Neurology, Eugenio deep vascular lesions showed a higher probability of developing abnormal movements. One year after Espejo Hospital, P.O. Box onset of the IAMs, 12 patients (21.4%) completely improved their abnormal movements, 38 patients 17-07-9515, Quito, Ecuador, South America; (67.8%) partially improved, four did not improve (7.1%), and two patients with chorea died. -

Magnetic Resonance Imaging of Multiple Sclerosis: a Study of Pulse-Technique Efficacy
691 Magnetic Resonance Imaging of Multiple Sclerosis: A Study of Pulse-Technique Efficacy Val M. Runge1 Forty-two patients with the clinical diagnosis of multiple sclerosis were examined by Ann C. Price1 proton magnetic resonance imaging (MRI) at 0.5 T. An extensive protocol was used to Howard S. Kirshner2 facilitate a comparison of the efficacy of different pulse techniques. Results were also Joseph H. Allen 1 compared in 39 cases with high-resolution x-ray computed tomography (CT). MRI revealed characteristic abnormalities in each case, whereas CT was positive in only 15 C. Leon Partain 1 of 33 patients. Milder grades 1 and 2 disease were usually undetected by CT, and in all A. Everette James, Jr.1 cases, the abnormalities noted on MRI were much more extensive than on CT. Cerebral abnormalities were best shown with the T2-weighted spin-echo sequence (TE/TR = 120/1000); brainstem lesions were best defined on the inversion-recovery sequence (TE/TI/TR =30/400/1250). Increasing TE to 120 msec and TR to 2000 msec heightened the contrast between normal and abnormal white matter. However, the signal intensity of cerebrospinal fluid with this pulse technique obscured some abnormalities. The diagnosis of multiple sclerosis continues to be a clinical challenge [1,2). The lack of an objective means of assessment further complicates the evaluation of treatment regimens. Evoked potentials, cerebrospinal fluid (CSF) analysis , and computed tomography (CT) are currently used for diagnosis, but all lack sensitivity and/or specificity. Furthermore, postmortem examinations demonstrate many more lesions than those suggested by clinical means [3). -

High-Resolution Cortical Imaging
High-Resolution Cortical Imaging Alex de Crespigny Ph.D., Ellen Grant M.D., Larry Wald Ph.D., Jean Augustinack Ph.D., Bruce Fischl Ph.D., Helen D’Arceuil Ph.D. Martinos Center, Department of Radiology, Massachusetts General Hospital, Charlestown, MA Structure of the cortex The adult cerebral cortex is a complex convoluted multilayered structure averaging around 2.3mm thick, but thinner (≤ 2mm) in the depths of the sulcal folds and thicker (3-4mm) at the crown of the gyri. It is typically divided into 6 layers depending upon the constituent cell types. On examination a section of the cortex, it is seen to consist of alternating white and gray layers from the surface inward: (1) a thin layer of white substance; (2) a layer of gray substance; (3) a second white layer (outer band of Baillarger or band of Gennari); (4) a second gray layer; (5) a third white layer (inner band of Baillarger); (6) a third gray layer, which rests on the medullary substance of the gyrus (1). Cortical neurons form a highly organized laminar and radial structure with extensive efferents. Long association fibers connect to distant regions of the ipsilateral hemisphere, while short fibers connect to nearby ipsilateral regions. Commissural fibers connect to the cortical regions of the contralateral hemisphere, and projection fibers reach from the cortex into the subcortical structures e.g., corticothalamic/subthalamic projections, etc. High resolution structural MRI of the cortex Conventional diagnostic clinical MRI scans, with in plane resolution of ~1mm and slice thickness up to 5mm can define the gray-white interface of the cerebral cortex but cannot visualize structure within the cortex itself. -

University of Florida Thesis Or Dissertation Formatting
THE NEURAL CIRCUITRY OF RESTRICTED REPETITIVE BEHAVIOR By BRADLEY JAMES WILKES A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY UNIVERSITY OF FLORIDA 2018 © 2018 Bradley James Wilkes To my father, Wade Wilkes, for his lifelong support, love, and encouragement ACKNOWLEDGMENTS This research was supported by funding from the Dissertation Research Award from the American Psychological Assocation, the Pilot Project Award (Non-Patient Oriented Clinical/Translational Research) from the Clinical and Translational Science Institute at the University of Florida, the Robert A. and Phyllis Levitt Award, the Gerber Behavioral and Cognitive Neuroscience Psychology Research Award, and the Jacquelin Goldman Scholarship in Developmental Psychology. I would especially like to thank Drs. Mark Lewis, Marcelo Febo, David Vaillancourt, Luis Colon-Perez, Darragh Devine, Timothy Vollmer, and Michael King for their support and guidance. 4 TABLE OF CONTENTS page ACKNOWLEDGMENTS .................................................................................................. 4 LIST OF TABLES ............................................................................................................ 7 LIST OF FIGURES .......................................................................................................... 8 LIST OF ABBREVIATIONS ........................................................................................... 10 ABSTRACT .................................................................................................................. -

15 Telencephalon: Neocortex
15 Telencephalon: Neocortex Introduction.........................491 – Dendritic Clusters, Axonal Bundles and Radial Cell Cords As (Possible) Sulcal Pattern ........................498 Constituents of Neocortical Minicolumns . 582 Structural and Functional Subdivision – Microcircuitry of Neocortical Columns .... 586 ofNeocortex.........................498 – Neocortical Columns and Modules: – Structural Subdivision 1: Cytoarchitecture . 498 A Critical Commentary ............... 586 – Structural Subdivision 2: Myeloarchitecture . 506 Comparative Aspects ................... 591 – Structural Subdivision 3: Myelogenesis ....510 Synopsis of Main Neocortical Regions ...... 592 – Structural Subdivision 4: Connectivity .....510 – Introduction....................... 592 – Functional Subdivision ................516 – Association and Commissural Connections . 592 – Structural and Functional Subdivision: – Functional and Structural Asymmetry Overview .........................528 of the Two Hemispheres .............. 599 – Structural and Functional Localization – Occipital Lobe ..................... 600 in the Neocortex: Current Research – Parietal Lobe ...................... 605 and Perspectives ....................530 – TemporalLobe..................... 611 Neocortical Afferents ...................536 – Limbic Lobe and Paralimbic Belt ........ 617 Neocortical Neurons – FrontalLobe ...................... 620 and Their Synaptic Relationships ..........544 – Insula........................... 649 – IntroductoryNote...................544 – Typical Pyramidal -

Patients with Stroke Confined to Basal Ganglia Have Diminished Response to Rehabilitation Efforts
Patients with stroke confined to basal ganglia have diminished response to rehabilitation efforts Ichiro Miyai, MD, PhD; Alan D. Blau, PhD; Michael J. Reding, MD; and Bruce T. Volpe, MD Article abstract-Prediction of the functional outcome for patients with stroke has depended on the severity of impair- ment, location of brain injury, age, and general medical condition. This study compared admission and discharge func- tional outcome (Functional Independence Measure, FIM) and deficit severity (Fugl-Meyer, F-M) scores in a retrospective study of patients with similar neurologic impairments: homonymous hemianopia, hemisensory loss, and hemiparesis. CT-verified stroke location was the independent variable: cortical (n = ll),basal ganglia and internal capsule (normal cortex and thalamus, n = 131, or combined (cortical, basal ganglia, and internal capsule, n = 22). By 3 months on average after stroke, all groups demonstrated significantly improved motor function as measured by F-M scores. Patients with cortical lesions had the least CT-imaged damage and the best outcome. Patients with combined lesions and more extensive brain injury had significantly higher FIM scores (p< 0.05) than patients with injury restricted to the basal ganglid internal capsule. Patients with basal ganglidinternal capsule injury were more likely to have hypotonia, flaccid paralysis, and persistently impaired balance and ambulation performance. While all patients had a comparable rehabilitation experience, these results suggest that patients with stroke confined to the basal ganglia and internal capsule benefited less from therapy. Isolated basal ganglia stroke may cause persistent corticothalamic-basal ganglia interactions that are dysfunctional and impede recovery. NEUROLOGY 1997;48:95-101 In several studies rehabilitative intervention has im- matter, but not the basal ganglia, corona radiata, or inter- proved the functional outcome of patients with nal capsule. -

Target-Specific Contrast Agents for Magnetic Resonance Microscopy
NeuroImage 46 (2009) 382–393 Contents lists available at ScienceDirect NeuroImage journal homepage: www.elsevier.com/locate/ynimg Target-specific contrast agents for magnetic resonance microscopy Megan L. Blackwell a,b,⁎, Christian T. Farrar a,d, Bruce Fischl a,c,d, Bruce R. Rosen a,d a Athinoula A. Martinos Center for Biomedical Imaging, Charlestown, MA, USA b Harvard-MIT Division of Health Sciences and Technology, Cambridge, MA, USA c Computer Science and Artificial Intelligence Laboratory, MIT, Cambridge, MA, USA d Department of Radiology, Massachusetts General Hospital, Charlestown, MA, USA article info abstract Article history: High-resolution ex vivo magnetic resonance (MR) imaging can be used to delineate prominent architectonic Received 2 July 2007 features in the human brain, but increased contrast is required to visualize more subtle distinctions. To aid Revised 5 December 2008 MR sensitivity to cell density and myelination, we have begun the development of target-specific Accepted 15 January 2009 paramagnetic contrast agents. This work details the first application of luxol fast blue (LFB), an optical Available online 30 January 2009 stain for myelin, as a white matter-selective MR contrast agent for human ex vivo brain tissue. Formalin-fixed human visual cortex was imaged with an isotropic resolution between 80 and 150 μm at 4.7 and 14 T before and after en bloc staining with LFB. Longitudinal (R1) and transverse (R2) relaxation rates in LFB-stained tissue increased proportionally with myelination at both field strengths. Changes in R1 resulted in larger contrast-to-noise ratios (CNR), per unit time, on T1-weighted images between more myelinated cortical layers (IV–VI) and adjacent, superficial layers (I–III) at both field strengths. -

Direct Visualization of the Perforant Pathway in the Human Brain with Ex Vivo Diffusion Tensor Imaging
ORIGINAL RESEARCH ARTICLE published: 28 May 2010 HUMAN NEUROSCIENCE doi: 10.3389/fnhum.2010.00042 Direct visualization of the perforant pathway in the human brain with ex vivo diffusion tensor imaging Jean C. Augustinack1*, Karl Helmer1, Kristen E. Huber1, Sita Kakunoori1, Lilla Zöllei1,2 and Bruce Fischl1,2 1 Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Harvard Medical School, Charlestown, MA, USA 2 Computer Science and Artificial Intelligence Laboratory, Massachusetts Institute of Technology, Cambridge, MA, USA Edited by: Ex vivo magnetic resonance imaging yields high resolution images that reveal detailed cerebral Andreas Jeromin, Banyan Biomarkers, anatomy and explicit cytoarchitecture in the cerebral cortex, subcortical structures, and white USA matter in the human brain. Our data illustrate neuroanatomical correlates of limbic circuitry with Reviewed by: Konstantinos Arfanakis, Illinois Institute high resolution images at high field. In this report, we have studied ex vivo medial temporal of Technology, USA lobe samples in high resolution structural MRI and high resolution diffusion MRI. Structural and James Gee, University of Pennsylvania, diffusion MRIs were registered to each other and to histological sections stained for myelin for USA validation of the perforant pathway. We demonstrate probability maps and fiber tracking from Christopher Kroenke, Oregon Health and Science University, USA diffusion tensor data that allows the direct visualization of the perforant pathway. Although it *Correspondence: is not possible to validate the DTI data with invasive measures, results described here provide Jean Augustinack, Athinoula A. an additional line of evidence of the perforant pathway trajectory in the human brain and that Martinos Center for Biomedical the perforant pathway may cross the hippocampal sulcus. -

Staging of Alzheimer Disease-Associated Neurowbrillary Pathology Using Parayn Sections and Immunocytochemistry
Acta Neuropathol (2006) 112:389–404 DOI 10.1007/s00401-006-0127-z METHODS REPORT Staging of Alzheimer disease-associated neuroWbrillary pathology using paraYn sections and immunocytochemistry Heiko Braak · Irina AlafuzoV · Thomas Arzberger · Hans Kretzschmar · Kelly Del Tredici Received: 8 June 2006 / Revised: 21 July 2006 / Accepted: 21 July 2006 / Published online: 12 August 2006 © Springer-Verlag 2006 Abstract Assessment of Alzheimer’s disease (AD)- revised here by adapting tissue selection and process- related neuroWbrillary pathology requires a procedure ing to the needs of paraYn-embedded sections (5–15 m) that permits a suYcient diVerentiation between initial, and by introducing a robust immunoreaction (AT8) for intermediate, and late stages. The gradual deposition hyperphosphorylated tau protein that can be processed of a hyperphosphorylated tau protein within select on an automated basis. It is anticipated that this neuronal types in speciWc nuclei or areas is central to revised methodological protocol will enable a more the disease process. The staging of AD-related neuroW- uniform application of the staging procedure. brillary pathology originally described in 1991 was per- formed on unconventionally thick sections (100 m) Keywords Alzheimer’s disease · NeuroWbrillary using a modern silver technique and reXected the pro- changes · Immunocytochemistry · gress of the disease process based chieXy on the topo- Hyperphosphorylated tau protein · Neuropathologic graphic expansion of the lesions. To better meet the staging · Pretangles demands of routine laboratories this procedure is Introduction This study was made possible by funding from the German Research Council (Deutsche Forschungsgemeinschaft) and BrainNet Europe II (European Commission LSHM-CT-2004- The development of intraneuronal lesions at selec- 503039). -

MITOCW | MIT9 14S09 Lec36-Mp3
MITOCW | MIT9_14S09_lec36-mp3 The following content is provided under a Creative Commons license. Your support will help MIT OpenCourseWare continue to offer high quality educational resources for free. To make a donation or view additional materials from hundreds of MIT courses, visit MIT OpenCourseWare at ocw.mit.edu. PROFESSOR: So this class, we will talk about some of the cell types in the neocortex and the way they're connected. We'll talk about different regions of neocortex, that is actually after it had experienced, in evolution, a lot of expansion, and we're just going to deal with mammalian cortex in small animals, like rodents, and human being. And then we'll talk a little bit about some of the major fibers in and out of the membrain. We've talked about those already, but I want to review them to make sure that they're in your mind. And then we'll get, at least, to an introduction of thalamocortical connections, which again, you've had some because when we talked about visual system, we talked about the genicular body rejection in the visual area, primary visual cortex, the auditory cortex. We talked about medial geniculate body, somatosensory has been talked about several times. We talked about the ventral nucleus. All right. So what are the two most commonly encountered classes in the cortical cells? The most characteristic cell type in the neocortex is the pyramidal cell, and this is what they look like. This is Brodel's simplification of the pyramidal cell that shows their major characteristics, a cell body with a sort of pyramidal shape in an apical dendrite that goes up towards the surface, and many of these cells send their apical dendrite all the way up to the surface where they arborize right up in layer one. -
Visualpath Dental 2010.Jnt
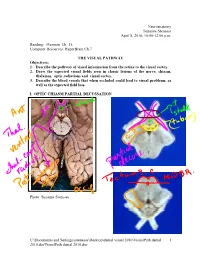
Neuroanatomy Suzanne Stensaas April 8, 2010, 10:00-12:00 p.m. Reading: Waxman Ch. 15, Computer Resources: HyperBrain Ch 7 THE VISUAL PATHWAY Objectives: 1. Describe the pathway of visual information from the retina to the visual cortex. 2. Draw the expected visual fields seen in classic lesions of the nerve, chiasm, thalamus, optic radiations and visual cortex. 3. Describe the blood vessels that when occluded could lead to visual problems, as well as the expected field loss. I. OPTIC CHIASM PARTIAL DECUSSATION Photo: Suzanne Stensaas C:\Documents and Settings\sstensaas\Desktop\dental visual 2010\VisualPath dental 1 2010.docVisualPath dental 2010.doc II. OPTIC TRACT Ganglion cell axons diverge A. 90% go to Lateral geniculate nucleus (LGN) of thalamus (the retino- geniculo-calcarine path ) B. 10% go to Superior colliculus and pretectum (the retinocollicular path for reflexes) C. The hypothalamus for circadian rhythms (not to be discussed) III. THALAMIC RELAY NUCLEUS -- the LATERAL GENICULATE NUCLEUS OR BODY A. Specific retinotopic projection. B. Six layers. Three layers get input from from each eye. Thalamus Red LGN LGN Nucleus C:\Documents and Settings\sstensaas\Desktop\dental visual 2010\VisualPath dental 2 2010.docVisualPath dental 2010.doc The optic tract projects to the LGN Crainial Nerves, Wilson-Pauwels et al., 1988 IV. OPTIC RADIATIONS A. Retinotopic organization from the LGN neurons to the cortex. B. Axons of neurons in the lateral geniculate form the optic radiations = geniculocalcarine tract. The retinotopic organization is maintained. 1. Some loop forward over inferior (or temporal) horn of lateral ventricle = Meyer's Loop 2. Other axons take a more direct posterior course through the deep parietal white matter. -

Journal of Anatomy
JOURNAL OF ANATOMY A CONTRIBUTION TO THE MORPHOLOGY OF THE CORPUS STRIATUM BY RAYMOND A. DART, Demonstrator of Anatomy, University College, London INTRODUCTION Fou a recapitulation of the essential features in the divergent conclusions of investigators who have studied this problem, we are indebted to the recent paper by Elliot Smith ('20) in which he pointed out the nature of the corpus striatum in Sphenodon, and indicated the morphological relationships of its several parts. For some time past I have been studying a series of sections of the brain of the highly specialised Marsupial Mole, Notoryctes typhlops, which was very kindly placed at my disposal by Prof. Elliot Smith. As might be anticipated, in this creature devoid of any visual apparatus, the olfactory and closely associated striatal areas play a dominant role in its cerebral constitution-features already described by Elliot Smith in his communication to the Royal Society of South Australia ('95). In attempting to elucidate the significance of these structures I have investigated more primitive forms in the biological series; and I have to acknowledge the generosity of Professors A. Dendy of King's College and J. P. Hill of University College for the free access to their important collections, which has made possible an extensive comparative study. It is primarily for the purpose of abbreviating the account of the brain of Notoryctes that this preliminary note upon the striatal region is submitted; but the problem of the evolution of the corpus striatum is sufficiently important to call for this separate treatment. - If a transverse section of the brain of Notoryctes be studied in the region of the anterior commissure and foramen of Monro (e.g.