Magnetic Resonance Imaging of Multiple Sclerosis: a Study of Pulse-Technique Efficacy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Post-Stroke Movement Disorders: Report of 56 Patients F Alarco´N, J C M Zijlmans, G Duen˜As, N Cevallos
1568 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.2003.011874 on 15 October 2004. Downloaded from PAPER Post-stroke movement disorders: report of 56 patients F Alarco´n, J C M Zijlmans, G Duen˜as, N Cevallos ............................................................................................................................... J Neurol Neurosurg Psychiatry 2004;75:1568–1574. doi: 10.1136/jnnp.2003.011874 Background: Although movement disorders that occur following a stroke have long been recognised in short series of patients, their frequency and clinical and imaging features have not been reported in large series of patients with stroke. Methods: We reviewed consecutive patients with involuntary abnormal movements (IAMs) following a stroke who were included in the Eugenio Espejo Hospital Stroke Registry and they were followed up for at least one year after the onset of the IAM. We determined the clinical features, topographical correlations, See end of article for authors’ affiliations and pathophysiological implications of the IAMs. ....................... Results: Of 1500 patients with stroke 56 developed movement disorders up to one year after the stroke. Patients with chorea were older and the patients with dystonia were younger than the patients with other Correspondence to: Dr. F Alarco´n, Department IAMs. In patients with isolated vascular lesions without IAMs, surface lesions prevailed but patients with of Neurology, Eugenio deep vascular lesions showed a higher probability of developing abnormal movements. One year after Espejo Hospital, P.O. Box onset of the IAMs, 12 patients (21.4%) completely improved their abnormal movements, 38 patients 17-07-9515, Quito, Ecuador, South America; (67.8%) partially improved, four did not improve (7.1%), and two patients with chorea died. -

Brainstem: Structure & Its Mode of Action
Journal of Neurology & Neurophysiology 2021, Vol.12, Issue 3, 521 Opinion Brainstem: Structure & Its Mode of action Karthikeyan Rupani Research Fellow, Tata Medical Centre, India. Corresponding Author* The brainstem is exceptionally little, making up around as it were 2.6 percent of the brain's add up to weight. It has the basic parts of directing cardiac, and Rupani K, respiratory work, making a difference to control heart rate and breathing rate. Research Fellow, Tata Medical Centre, India; It moreover gives the most engine and tactile nerve supply to the confront and E-mail: [email protected] neck by means of the cranial nerves. Ten sets of cranial nerves come from the brainstem. Other parts incorporate the direction of the central apprehensive Copyright: 2021 Rupani K. This is an open-access article distributed under the framework and the body's sleep cycle. It is additionally of prime significance terms of the Creative Commons Attribution License, which permits unrestricted within the movement of engine and tangible pathways from the rest of the use, distribution, and reproduction in any medium, provided the original author brain to the body, and from the body back to the brain. These pathways and source are credited. incorporate the corticospinal tract (engine work), the dorsal column-medial lemniscus pathway and the spinothalamic tract [3]. The primary part of the brainstem we'll consider is the midbrain. The midbrain Received 01 March 2021; Accepted 15 March 2021; Published 22 March 2021 (too known as the mesencephalon) is the foremost prevalent of the three districts of the brainstem. It acts as a conduit between the forebrain over and the pons and cerebellum underneath. -

University of Florida Thesis Or Dissertation Formatting
THE NEURAL CIRCUITRY OF RESTRICTED REPETITIVE BEHAVIOR By BRADLEY JAMES WILKES A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY UNIVERSITY OF FLORIDA 2018 © 2018 Bradley James Wilkes To my father, Wade Wilkes, for his lifelong support, love, and encouragement ACKNOWLEDGMENTS This research was supported by funding from the Dissertation Research Award from the American Psychological Assocation, the Pilot Project Award (Non-Patient Oriented Clinical/Translational Research) from the Clinical and Translational Science Institute at the University of Florida, the Robert A. and Phyllis Levitt Award, the Gerber Behavioral and Cognitive Neuroscience Psychology Research Award, and the Jacquelin Goldman Scholarship in Developmental Psychology. I would especially like to thank Drs. Mark Lewis, Marcelo Febo, David Vaillancourt, Luis Colon-Perez, Darragh Devine, Timothy Vollmer, and Michael King for their support and guidance. 4 TABLE OF CONTENTS page ACKNOWLEDGMENTS .................................................................................................. 4 LIST OF TABLES ............................................................................................................ 7 LIST OF FIGURES .......................................................................................................... 8 LIST OF ABBREVIATIONS ........................................................................................... 10 ABSTRACT .................................................................................................................. -

Patients with Stroke Confined to Basal Ganglia Have Diminished Response to Rehabilitation Efforts
Patients with stroke confined to basal ganglia have diminished response to rehabilitation efforts Ichiro Miyai, MD, PhD; Alan D. Blau, PhD; Michael J. Reding, MD; and Bruce T. Volpe, MD Article abstract-Prediction of the functional outcome for patients with stroke has depended on the severity of impair- ment, location of brain injury, age, and general medical condition. This study compared admission and discharge func- tional outcome (Functional Independence Measure, FIM) and deficit severity (Fugl-Meyer, F-M) scores in a retrospective study of patients with similar neurologic impairments: homonymous hemianopia, hemisensory loss, and hemiparesis. CT-verified stroke location was the independent variable: cortical (n = ll),basal ganglia and internal capsule (normal cortex and thalamus, n = 131, or combined (cortical, basal ganglia, and internal capsule, n = 22). By 3 months on average after stroke, all groups demonstrated significantly improved motor function as measured by F-M scores. Patients with cortical lesions had the least CT-imaged damage and the best outcome. Patients with combined lesions and more extensive brain injury had significantly higher FIM scores (p< 0.05) than patients with injury restricted to the basal ganglid internal capsule. Patients with basal ganglidinternal capsule injury were more likely to have hypotonia, flaccid paralysis, and persistently impaired balance and ambulation performance. While all patients had a comparable rehabilitation experience, these results suggest that patients with stroke confined to the basal ganglia and internal capsule benefited less from therapy. Isolated basal ganglia stroke may cause persistent corticothalamic-basal ganglia interactions that are dysfunctional and impede recovery. NEUROLOGY 1997;48:95-101 In several studies rehabilitative intervention has im- matter, but not the basal ganglia, corona radiata, or inter- proved the functional outcome of patients with nal capsule. -

Electrophysiological Changes That Accompany Reactive Gliosis in Vitro
The Journal of Neuroscience, October 1, 1997, 17(19):7316–7329 Electrophysiological Changes That Accompany Reactive Gliosis In Vitro Stacey Nee MacFarlane and Harald Sontheimer Department of Neurobiology, University of Alabama, Birmingham, Birmingham, Alabama 35294 An in vitro injury model was used to examine the electrophys- negative resting potentials in nonproliferating (260 mV) versus iological changes that accompany reactive gliosis. Mechanical proliferating astrocytes (253 mV; p 5 0.015). Although 45% of scarring of confluent spinal cord astrocytes led to a threefold the nonproliferating astrocytes expressed Na 1 currents (0.47 increase in the proliferation of scar-associated astrocytes, as pS/pF), the majority of proliferating cells expressed prominent judged by bromodeoxyuridine (BrdU) labeling. Whole-cell Na 1 currents (0.94 pS/pF). Injury-induced electrophysiological patch-clamp recordings demonstrated that current profiles dif- changes are rapid and transient, appearing within 4 hr postin- 2 fered absolutely between nonproliferating (BrdU ) and prolifer- jury and, with the exception of KIR , returning to control con- ating (BrdU 1) astrocytes. The predominant current type ex- ductances within 24 hr. These differences between proliferating pressed in BrdU 2 cells was an inwardly rectifying K 1 current and nonproliferating astrocytes are reminiscent of electrophys- 2 (KIR ; 1.3 pS/pF). BrdU cells also expressed transient outward iological changes observed during gliogenesis, suggesting that K 1 currents, accounting for less than -

Orienting Head Movements Resulting from Electrical Microstimulation of the Brainstem Tegmentum in the Barn Owl
The Journal of Neuroscience, January 1993, 13(l): 351370 Orienting Head Movements Resulting from Electrical Microstimulation of the Brainstem Tegmentum in the Barn Owl Tom Masino and Eric I. Knudsen Department of Neurobiology, Stanford University, Stanford, California 943055401 The size and direction of orienting movements are repre- movement latency, duration, velocity, and size each dem- sented systematically as a motor map in the optic tectum of onstrated dependencies on stimulus amplitude, frequency, the barn owl (du Lac and Knudsen, 1990). The optic tectum and duration. projects to several distinct regions in the medial brainstem The data demonstrate directly that at the level of the mid- tegmentum, which in turn project to the spinal cord (Masino brain tegmentum there exists a three-dimensional Cartesian and Knudsen, 1992). This study explores the hypothesis that representation of head-orienting movements such that hor- a fundamental transformation in the neural representation izontal, vertical, and roll components of movement are en- of orienting movements takes place in the brainstem teg- coded by anatomically distinct neural circuits. The data sug- mentum. Head movements evoked by electrical microstim- gest that in the projection from the optic tectum to these ulation in the brainstem tegmentum of the alert barn owl were medial tegmental regions, the topographic code for orienting cataloged and the sites of stimulation were reconstructed movement that originates in the tectum is transformed into histologically. Movements elicited from the brainstem teg- this Cartesian code. mentum were categorized into one of six different classes: [Key words: optic tectum, superior colliculus, saccadic saccadic head rotations, head translations, facial move- head movement, brainstem tegmentum, interstitial nucleus ments, vocalizations, limb movements, and twitches. -

Brainstem Dysfunction in Critically Ill Patients
Benghanem et al. Critical Care (2020) 24:5 https://doi.org/10.1186/s13054-019-2718-9 REVIEW Open Access Brainstem dysfunction in critically ill patients Sarah Benghanem1,2 , Aurélien Mazeraud3,4, Eric Azabou5, Vibol Chhor6, Cassia Righy Shinotsuka7,8, Jan Claassen9, Benjamin Rohaut1,9,10† and Tarek Sharshar3,4*† Abstract The brainstem conveys sensory and motor inputs between the spinal cord and the brain, and contains nuclei of the cranial nerves. It controls the sleep-wake cycle and vital functions via the ascending reticular activating system and the autonomic nuclei, respectively. Brainstem dysfunction may lead to sensory and motor deficits, cranial nerve palsies, impairment of consciousness, dysautonomia, and respiratory failure. The brainstem is prone to various primary and secondary insults, resulting in acute or chronic dysfunction. Of particular importance for characterizing brainstem dysfunction and identifying the underlying etiology are a detailed clinical examination, MRI, neurophysiologic tests such as brainstem auditory evoked potentials, and an analysis of the cerebrospinal fluid. Detection of brainstem dysfunction is challenging but of utmost importance in comatose and deeply sedated patients both to guide therapy and to support outcome prediction. In the present review, we summarize the neuroanatomy, clinical syndromes, and diagnostic techniques of critical illness-associated brainstem dysfunction for the critical care setting. Keywords: Brainstem dysfunction, Brain injured patients, Intensive care unit, Sedation, Brainstem -

Isolated Necrosis of Central Tegmental Tracts Due to Neonatal Hypoxic-Ischemic Encephalopathy: MRI Findings
Journal of Neurology & Stroke Case Report Open Access Isolated necrosis of central tegmental tracts due to neonatal hypoxic-ischemic encephalopathy: MRI findings Abstract Volume 11 Issue 1 - 2021 Perinatal hypoxia is an old entity that still prevails today and may lead to neurological Tomás de Andrade Lourenção Freddi, Luiz sequelae that can go unnoticed until a certain age, generating many costs for public health. In this case report, we demonstrate on magnetic resonance imaging an unusual pattern of Fellipe Curvêlo Ciraulo Santos, Nelson Paes perinatal hypoxia in a preterm 5-month-old infant, involving the central tegmental tracts Fortes Diniz Ferreira, Felipe Diego Gomes and briefly discuss its possible pathophysiology. Dantas Department of Radiology, Hospital do Coração, Brazil Keywords: magnetic resonance imaging, asphyxia, hypoxic-ischemic encephalopathy, tegmentum, neonates, brainstem Correspondence: Tomás de Andrade Lourenção Freddi, Hospital do Coração, 147 Desembargador Eliseu Guilherme Street, São Paulo, SP, 04004-030, Brazil, Tel +5511976059280, Email Received: May 25, 2020 | Published: Febrauary 15, 2021 Abbreviations: MRI, magnetic resonance imaging; HII, that connect the red nucleus and the inferior olivary nucleus, being hypoxic-ischemic injury; FLAIR, fluid-attenuated inversion recovery; part of the dentato-rubro-olivary system, called Guillain–Mollaret CTT, central tegmental tract; VGB, vigabatrin triangle.3–5 Introduction Hypoxic-ischemic injury (HII) is one of the most important causes of encephalopathy in neonates, irrespective of gestational age, and may occur in the uterus or during delivery by different intrapartum conditions. In preterm or very low birth weight infants, brain magnetic resonance imaging (MRI) can demonstrate multiple different findings, which a detailed description is beyond the scope of this article, although being periventricular leukomalacia the most frequent (seen in at least 50% of cases). -

SAY: Welcome to Module 1: Anatomy & Physiology of the Brain. This
12/19/2018 11:00 AM FOUNDATIONAL LEARNING SYSTEM 092892-181219 © Johnson & Johnson Servicesv Inc. 2018 All rights reserved. 1 SAY: Welcome to Module 1: Anatomy & Physiology of the Brain. This module will strengthen your understanding of basic neuroanatomy, neurovasculature, and functional roles of specific brain regions. 1 12/19/2018 11:00 AM Lesson 1: Introduction to the Brain The brain is a dense organ with various functional units. Understanding the anatomy of the brain can be aided by looking at it from different organizational layers. In this lesson, we’ll discuss the principle brain regions, layers of the brain, and lobes of the brain, as well as common terms used to orient neuroanatomical discussions. 2 SAY: The brain is a dense organ with various functional units. Understanding the anatomy of the brain can be aided by looking at it from different organizational layers. (Purves 2012/p717/para1) In this lesson, we’ll explore these organizational layers by discussing the principle brain regions, layers of the brain, and lobes of the brain. We’ll also discuss the terms used by scientists and healthcare providers to orient neuroanatomical discussions. 2 12/19/2018 11:00 AM Lesson 1: Learning Objectives • Define terms used to specify neuroanatomical locations • Recall the 4 principle regions of the brain • Identify the 3 layers of the brain and their relative location • Match each of the 4 lobes of the brain with their respective functions 3 SAY: Please take a moment to review the learning objectives for this lesson. 3 12/19/2018 11:00 AM Directional Terms Used in Anatomy 4 SAY: Specific directional terms are used when specifying the location of a structure or area of the brain. -

Chapter 128: Basic Mechanisms of Sleep: New Evidence On
128 BASIC MECHANISMS OF SLEEP: NEW EVIDENCE ON THE NEUROANATOMY AND NEUROMODULATION OF THE NREM-REM CYCLE EDWARD F. PACE-SCHOTT J. ALLAN HOBSON The 1990s brought a wealth of new detail to our knowledge NREM sleep (noradrenergic, serotonergic, and cholinergic of the brain structures involved in the control of sleep and systems damped), and REM sleep (noradrenergic and sero- waking and in the cellular level mechanisms that orchestrate tonergic systems off, cholinergic system undamped) (1–4). the sleep cycle through neuromodulation. This chapter pre- sents these new findings in the context of the general history Original Reciprocal Interaction Model: An of research on the brainstem neuromodulatory systems and Aminergic-Cholinergic Interplay the more specific organization of those systems in the con- trol of the alternation of wake, non–rapid eye movement The model of reciprocal interaction (5) provided a theoretic (NREM), and REM sleep. framework for experimental interventions at the cellular and Although the main focus of the chapter is on the our molecular level that has vindicated the notion that waking own model of reciprocal aminergic-cholinergic interaction, and REM sleep are at opposite ends of an aminergically we review new data suggesting the involvement of many dominant to cholinergically dominant neuromodulatory more chemically specific neuronal groups than can be ac- continuum, with NREM sleep holding an intermediate po- commodated by that model. We also extend our purview to sition (Fig. 128.1). The reciprocal interaction hypothesis the way in which the brainstem interacts with the forebrain. (5) provided a description of the aminergic-cholinergic in- These considerations inform not only sleep-cycle control terplay at the synaptic level and a mathematic analysis of per se, but also the way that circadian and ultradian rhythms the dynamics of the neurobiological control system. -

Müller Glia Regenerative Potential Is Maintained Throughout Life Despite 2 Neurodegeneration and Gliosis in the Ageing Zebrafish Retina 3 4 AUTHORS 5 Raquel R
bioRxiv preprint doi: https://doi.org/10.1101/2020.06.28.174821; this version posted October 29, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. 1 Müller Glia regenerative potential is maintained throughout life despite 2 neurodegeneration and gliosis in the ageing zebrafish retina 3 4 AUTHORS 5 Raquel R. Martins1,2, Mazen Zamzam3, Mariya Moosajee4,5,6,7, Ryan Thummel3, Catarina M. 6 Henriques1,2§, Ryan B. MaCDonald4§ 7 8 Affiliations: 9 1. Bateson Centre, University of Sheffield, Sheffield, S10 2TN, UK. 10 2. Department of OnCology and Metabolism, University of Sheffield, Sheffield, S10 2TN 11 UK. 12 3. Department of Ophthalmology, Visual and AnatomiCal SCienCes, Wayne State 13 University School of MediCine, Detroit, MI 48201, USA. 14 4. Institute of Ophthalmology, University College London, London, EC1V 9EL, UK. 15 5. Moorfields Eye Hospital NHS Foundation Trust, London, EC1V 2PD, UK 16 6. Great Ormond Street Hospital for Children NHS Foundation Trust, London, WC1N 17 3JH, UK 18 7. The FranCis CriCk Institute, London, NW1 1AT, London 19 20 21 22 §Co-corresponding authors: [email protected] and [email protected] 23 24 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.06.28.174821; this version posted October 29, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. 25 ABSTRACT 26 Ageing is a signifiCant risk faCtor for degeneration of the retina. -
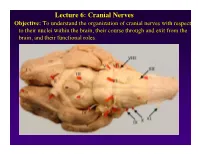
Lecture 6: Cranial Nerves
Lecture 6: Cranial Nerves Objective: To understand the organization of cranial nerves with respect to their nuclei within the brain, their course through and exit from the brain, and their functional roles. Olfactory Eye Muscles 3, 4 &6 Cranial Nerves 1-7 I overview Table, Page 49 II Lecture notes Cranial Nerves and their Functions V Trigeminal VII Facial VIII IX X XII XI Cranial Nerves 8-12 Overview sternocephalic I. Factors Responsible for the Complex Internal Organization of the Brain Stem-> leads to altered location of cranial nerve nuclei in adult brain stem 1. Development of the Fourth Ventricle a. Medulla and Pons develop ventral to the 4th ventricle cerebellum b. Alar plate is displaced lateral to basal plate 4 Medulla Developing Neural Tube 2. Cranial nerve nuclei form discontinuous columns Rostral 12 SE Page 48 Notes 3. Some cranial nerve nuclei migrate from their primitive embryonic positions (e.g., nuclei of V and VII) Facial N. Factors responsible for the complex internal organization of the brainstem: 4) Special senses develop in association with the brain stem. Nuclei of special senses 5) Development of the cerebellum and its connections Cerebellum II. Cranial Nerve Nuclei: Nucleus = column of neuron cell bodies. Efferent nuclei are composed of cell bodies of alpha or gamma motor neurons (SE) or preganglionic parasympathetic neurons (VE). III. Motor Efferent Nuclei (Basal Plate Derivatives): 1. SE (Somatic Efferent) Nuclei: SE neurons form two longitudinally oriented but discontinuous columns of cell bodies in the brain stem. Neurons that comprise these columns are responsible for innervating all of the skeletal musculature of the head.