Bureau of Air Safety Investigation Report Basi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Orientation Sheet for Horizon Updated: 2017-Apr-21
Orientation Sheet for Horizon Updated: 2017-Apr-21 General • All voyages should be documented in the ship’s log book. Report any damage or deficiencies to [email protected] and to boat manager [email protected] / 410-203-2673 Specifications Registration #: MD 5596 AC Hull#: XLY 595267 Make: Islander 36 Year: 1977 Engine: Perkins 4.108; 4-cyl Diesel 48-HP Displacement: 13,450 lbs Draft: 5’ 02” Mast Height Fuel Capacity: 30 gal. Holding tank: 18 gal. (from waterline): 52’ 06” Water Capacity: 54 gal. 2 tanks, below Salon Settees LOA: 36’ 08" Batteries: House battery 1 and 2 (Starboard lazaret) LWL: 28’ 25” Starting Battery (under companionway steps) Beam: 11’ 17” Sails: Main, Genoa on furler, staysail with boom Safety Equipment First Aid Kit: Drawer port side Rescue Sling: Stern Rail PFDs: V-berth Fire Extinguishers: (2) – Starboard side cabin, Port quater berth Day/Night Flares: Aerial & Hand-held – Drawer port side above seats in salon Sounds (Horn, Bell & Whistle): Drawer port side above seats in salon Auto-Switched Bilge Pump: Wired directly to House Battery (must be switched to Auto when leaving boat). The switch is located on the starboard side inside the cabin above the galley sink Old Bilge Pump: Wired to Electric Panel on the engine compartment wall (manual mode only). Do not use this pump unless the other one is not working. Manual Bilge Pump: Cockpit Port side (handle located in drawer port side above seats) Anchors: Danforth (35 lbs) bow; Rode: 15’ of chain & 150’ of line (marked every 30’) Thru-hulls/Sea-cocks: Engine -

Gannet Electronics
Gannet Electronics A Summary of the Electronic Equipment Fitted to early Model R.A.N Gannet A.S.1 Aircraft Prepared by David Mowat Ex-L.R.E.M.(A) 21st. August 2003 Page 1 Page 2 GANNET ELECTRONIC EQUIPMENT Introduction The ‘Heart’ of the Gannet as a Weapons System was its Electronic Equipment. It contained a comprehensive range of electronic equipment to enable it to perform the various roles for which it was designed. Its Primary Role was to detect, locate, and destroy enemy submarines. For this Role, the Aircraft was fitted with a Search Radar and Sonobuoy Systems. Other electronic systems were also installed for Communications, both internal and external, and Navigation. The various equipments were allocated an ‘Aircraft Radio Installation’ (ARI) number, which specified the actual equipment used in each installation. These may vary between aircraft depending on the role that the particular aircraft was to perform. A cross- reference List of ARI’s is shown at Appendix ‘A’. The various equipments can be grouped into four major categories as follows: a.! Communications b.! Navigation c.! Warfare Systems d.! Stores Communications Equipment The Communications Equipment was used to enable the crew to talk to each other (internal communications) and other aircraft, ships or bases (external communications). They are as follows: a.! Audio Amplifier Type A1961 The Type A1921 was used to amplify the Microphone outputs from the three crew members and feed it back into the earphones. It was located on the port side of the rear cockpit at about seat height just forward of the Radio Operator. -

19750827-0 DC-3 5Y-AAF.Pdf
1 CAV/ACC/24/75 ACCIDENT IUVESTIGATION BRANCH CIVIL AIRCRAFT ACCIDEiiT Report on the Accident to Douglas DC-3 Aircraft Registration number 5Y-AAF which occurred on the 27th August,1975 At 0922 hours, at Mtwara Airport, Tanzania. E A S T A F R I CAN C 0 M M U NIT Y AOCIDEwr REPORT AOCIDE:~T INVESTIGATIOn BRAl'WH 'CIVIL ACCIDENT REPORT CAV/ACC/24/75 AIRCRAFT TYPE 8; HEGISTRATION: Douglas DC-::- 5Y-l~ ENGINE: Pratt & \filii tney R1830-90D REGISTERED OWlIJ]~R & OPERATOR: East African Airways Corporation, P.O. Box 19002, NAIROBI, Kenya. CREVf: CAPTAIN Gabriel Sebastian Turuka ) ) Uninjured FIJ:1ST OFFICER Steven Robert Wegoye ) PASSENGER: Sixteen - Uninjured. PLACE OF ACCIDEHT: ~,1twara Airport, Tanzania. DATE AND T1MB: 27th August, 1975, 0922 hours. ALL rrU'lES IN THIS REPORT ARE G.1VI. T. SUMMARY The aircraft was operating East African Airways Service flight number EC037 from Dar es Salaam to Nachingmea with an unscheduled refuelling stop at I1twara with 3 crew and 16 passengers on board. The flight from Dar es Salaam was uneventful and an approach and landing was made onto runway 19. After touch down the aircraft swung to the left and then to the right, after which it left the runway where both main landing gear assys collapsed causing substantial daLage to the centre section and nacelle structure. The report concludes that the most probable cause of the accident was the failure of the pilot to initiate corrective action to prevent the aircraft from turning off the runway. 1.1 HISTORY OF THE FLIGHT: The aircraft departed Dar es Salaam with three crew and 16 passengers. -

Drivetrain 17 36 30 30 31 32 32 33 35 37 38 39 39 40 40 41 41 41 41 41 40 36-40
B Drivetrain ............................... 18 to 41 Drivetrain Struts Main .............................................................................18-19 Self-aligning gland type (with space) ................................. 30 Intermediate ...................................................................... 18 Heavy duty ..................................................................... 30 Sailboat ............................................................................. 19 Studs .................................................................................. 31 Port and starboard ............................................................ 20 Tournament (with space) ................................................ 32 Vee .................................................................................... 21 Self-aligning gland type (without space) ............................ 32 Universal ........................................................................... 21 Spud type Adjustable ....................................................................22-23 Tournament water cooled ............................................... 33 Cut off type ..................................................................... 22 Right hand thread ........................................................... 35 Swivel type ..................................................................... 23 Shaft logs..........................................................................36-40 Strut bolts ............................................................................. -

PRODUCT and SERVICES CATALOGUE September 2021
PRODUCT AND SERVICES CATALOGUE September 2021 COMPONENTS | AVIONICS | STRUCTURES | STC DESIGN/DEVELOPMENT | MANUFACTURING | INSPECTIONS 1 Full Line of Aircraft Services Get Flying, Faster COMPONENTS | AVIONICS | STRUCTURES | STC DESIGN/DEVELOPMENT | MANUFACTURING | INSPECTIONS VIH Aerospace offers a variety of Manufacturing, Maintenance, Repair & Overhaul (MMRO) services and products for the helicopter industry. We specialize in providing high quality and cost effective solutions including: • Component Repair, Overhaul, Paint, Rental & Exchange VIH Aerospace • Avionics Repair, Installations, Upgrades, Rewiring, & NVIS Supports • Structural Repairs, Aircraft Completions, Refurbishments, Paint, & Inspections Bell | Sikorsky | Airbus • Engineering Services, STC Design/Development, 3D Scanning • Manufacturing, Machining, Welding, Modifications, & NDT • Scheduled & Unscheduled Inspections Our Address Contact Us 1962 Canso Rd. Phone: 250-655-6828 | Fax: 250-655-6842 | Toll Free: 1-833-267-9494 North Saanich, BC, Sales Enquiries: [email protected] | General Enquiries: [email protected] Canada V8L 5V5 Website: www.vihaerospace.com 2 TABLE OF CONTENTS Get Flying Faster .............................................................................. 2 Our Industry Partners .................................................................... 3 Meet our Team ................................................................................. 4 Aircraft MMRO Services ................................................................. 5 OUR INDUSTRY PARTNERS Component -

WO 2015/012935 A2 29 January 2015 (29.01.2015) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2015/012935 A2 29 January 2015 (29.01.2015) P O P C T (51) International Patent Classification: Bart Dean [US/US]; 2691 Daunet Ave., Simi Valley, Cali B64C 27/26 (2006.01) B64C 27/54 (2006.01) fornia 93065 (US). PARKS, William Martin [US/US]; B64C 5/02 (2006.01) B64C 39/02 (2006.01) 2805 North Woodrow Ave., Simi Valley, California 93065 B64C 9/00 (2006.01) G05D 1/08 (2006.01) (US). GANZER, David Wayne [US/US]; 4607 Kleberg B64C 25/00 (2006.01) B64C 29/00 (2006.01) St., Simi Valley, California 93063 (US). FISHER, Chris¬ topher Eugene [US/US]; 4 1 Los Vientos Dr., Thousand (21) International Application Number: Oaks, California 91320 (US). MUKHERJEE, Jason Sid- PCT/US20 14/036863 harthadev [US/US]; 605 Muirfield Ave., Simi Valley, (22) International Filing Date: California 93065 (US). KING, Joseph Frederick 5 May 2014 (05.05.2014) [US/US]; 10540 Gaviota Ave., Granada Hills, California 91344 (US). (25) Filing Language: English (74) Agent: DAWSON, James K.; 1445 E. Los Angeles Ave., English (26) Publication Language: Suite 108, Simi Valley, California 93065-2827 (US). (30) Priority Data: (81) Designated States (unless otherwise indicated, for every 3 May 2013 (03.05.2013) 61/819,487 US kind of national protection available): AE, AG, AL, AM, (71) Applicant: AEROVIRONMENT, INC. [US/US]; 181 W . AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, Huntington Drive, Suite 202, Monrovia, California 91016 BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, (US). -

Going Places
Bristow Group Inc. 2007 Annual Report Going Places Bristow Group Inc. 2000 W Sam Houston Pkwy S Suite 1700, Houston, Texas 77042 t 713.267.7600 f 713.267.7620 www.bristowgroup.com 2007 Annual Report BOARD OF DIRECTORS OFFICERS CORPORATE INFORMATION Thomas C. Knudson William E. Chiles Corporate Offi ces Chairman, Bristow Group Inc.; President, Chief Executive Offi cer Bristow Group Inc. Retired Senior Vice President of and Director 2000 W Sam Houston Pkwy S ConocoPhillips Suite 1700, Houston, Texas 77042 Perry L. Elders Telephone: 713.267.7600 Thomas N. Amonett Executive Vice President and Fax: 713.267.7620 President and CEO, Chief Financial Offi cer www.bristowgroup.com Champion Technologies, Inc. Richard D. Burman Common Stock Information Charles F. Bolden, Jr. Senior Vice President, The company’s NYSE symbol is BRS. Major General Charles F. Bolden Jr., Eastern Hemisphere U.S. Marine Corps (Retired); Investor Information CEO of JACKandPANTHER L.L.C. Michael R. Suldo Additional information on the company Senior Vice President, is available at our web site Peter N. Buckley Western Hemisphere www.bristowgroup.com Chairman, Caledonia Investments plc. Michael J. Simon Transfer Agent Senior Vice President, Mellon Investor Services LLC Stephen J. Cannon Production Management 480 Washington Boulevard Retired President, Jersey City, NJ 07310 DynCorp International, L.L.C. Patrick Corr www.melloninvestor.com Senior Vice President, Jonathan H. Cartwright Global Training Auditors Finance Director, KPMG LLP Our Values Caledonia Investments plc. Mark B. Duncan Senior Vice President, William E. Chiles Global Business Development President & Chief Executive Offi cer, Bristow’s values represent our core beliefs about how we conduct our business. -
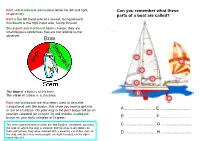
Sailing Terms Into the Wind, but We Can Start Sailing from About 30 Degrees Away from the Wind
Port and starboard are nautical terms for left and right, Can you remember what these respectively. parts of a boat are called? Port is the left-hand side of a vessel, facing forward. Starboard is the right-hand side, facing forward. Since port and starboard never change, they are unambiguous references that are not relative to the observer. Bow The bow of a boat is at the front The stern of a boat is at the back Port and starboard are also terms used to describe navigational aids like buoys, that show you how to get into A …...................... E …...................... or out of a harbour. On your way in the port buoys will be on your left coloured (or at night, lit) red and the starboard buoys on your right coloured or lit green. B …...................... F …...................... The term starboard derives from the Old English 'steorbord', meaning C …...................... G …...................... the side on which the ship is steered. Before ships had rudders on their centrelines, they were steered with a steering oar at the stern of D …...................... H …...................... the ship and, because more people are right-handed, on the right- hand side of it. When we're sailing a boat we always want to know An introduction to where the wind is coming from. We can't sail straight sailing terms into the wind, but we can start sailing from about 30 degrees away from the wind. Each 'point of sail' has a When you first come out sailing you'll discover a whole name according to the angle away from the wind. -

Propulsion Shafting Alignment
Guidance Notes on Propulsion Shafting Alignment GUIDANCE NOTES ON PROPULSION SHAFTING ALIGNMENT SEPTEMBER 2019 American Bureau of Shipping Incorporated by Act of Legislature of the State of New York 1862 2019 American Bureau of Shipping. All rights reserved. 1701 City Plaza Drive Spring, TX 77389 USA Foreword Foreword ABS identified the need to provide a more detailed explanation of alignment design and practices, which resulted in the development of the Guidance Notes on Propulsion Shafting Alignment. Their primary purpose is to provide clarification for ABS Surveyors and plan review engineers to verify consistency of the survey and plan approval processes. Regarding the shaft alignment design and implementation efforts by the shipbuilding industry, these Guidance Notes are valuable to further advance its approach towards shaft alignment analyses and procedures. Additionally, ABS has developed state-of-the-art analytical tools primarily for the purpose of engineering analysis and design. The ABS shaft alignment program, combined with alignment optimization software, is capable of analyzing complex propulsion installations and, when used as a design tool, may provide an optimized solution to the alignment problem. This 2019 edition is arranged to include additional topics on shaft alignment condition monitoring and a section dedicated to alignment problems and their solutions. Shaft alignment survey requirements are summarized in the introduction and are addressed further under a separate section on shaft alignment procedures and practices. Discussion on alignment calculation and measurement is expanded to include the stern tube bearing clearance measurement. Additional clarification is provided on the application of the hull deflections, alignment optimization, propulsion systems with no forward stern tube bearing, and reverse engineering calculation. -

More Embraer Rj-145 Flight Simulators on Order For
The News from FlightSafety… FLIGHTSAFETY RECEIVES APPROVAL FROM AVIATION REGULATORY AUTHORITIES IN EUROPE AND BRAZIL FOR ITS BELL HELICOPTER SIMULATORS AND TRAINING PROGRAMS LaGuardia Airport, New York (October 20, 2009) – FlightSafety International has received Joint Aviation Authority Type Rating Training Organization approval from the United Kingdom Civil Aviation Authority for its Bell Helicopter 212/412 and 430 training programs. In addition the Bell Helicopter 212/412 simulator has been qualified by the European Aviation Safety Agency and the Bell Helicopter 430 simulator has also been qualified by the National Civil Aviation Agency of Brazil and EASA. The Bell Helicopter 212, 412 and 430 simulators and training programs are located at FlightSafety’s Learning Center in Fort Worth, Texas. “This qualification of our Bell Helicopter simulators and training programs demonstrates the quality and effectiveness of our training programs and high fidelity of our flight simulators.” said Barbara Taylor, Manager, Fort Worth Learning Center. “Our Customers appreciate FlightSafety’s ability to develop and deliver helicopter training programs that are tailored to their specific needs and meet the regulatory requirements they operate under.” FlightSafety has provided factory authorized training for aircraft manufactured by Bell Helicopter for more than 30 years. The company currently offers training programs for Bell 212, Bell 214ST, Bell 222, Bell 230, Bell 412 and Bell 430 aircraft at its Learning Center in Fort Worth, Texas. Other professional helicopter training programs are offered by FlightSafety at its Learning Centers in Lafayette, Louisiana; West Palm Beach, Florida and at the Farnborough airport in the United Kingdom. FlightSafety was the first simulator manufacturer to receive Level D qualification from the Federal Aviation Administration for a full flight helicopter simulator. -
Trawl Positioning System User Guide
Trawl Positioning System User Guide Contents | ii Contents Legal................................................................................................. 5 History...........................................................................................................................................................................5 Copyright......................................................................................................................................................................6 Disclaimer....................................................................................................................................................................6 Introduction and Presentation..........................................................7 Introduction................................................................................................................................................................ 7 Applications.................................................................................................................................................................8 Safety Guidelines..................................................................................................................................................... 11 About Trawl Positioning...................................................................................................................................... 12 About Spread Sensors.......................................................................................................................................... -

Bayesian Sensitivity Analysis of Flight Parameters in a Hard-Landing Analysis Process
This is a repository copy of Bayesian Sensitivity Analysis of Flight Parameters in a Hard-Landing Analysis Process. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/121812/ Version: Accepted Version Article: Sartor, P., Becker, W., Worden, K. orcid.org/0000-0002-1035-238X et al. (2 more authors) (2016) Bayesian Sensitivity Analysis of Flight Parameters in a Hard-Landing Analysis Process. Journal of Aircraft, 53 (5). pp. 1317-1331. ISSN 0021-8669 https://doi.org/10.2514/1.C032757 Reuse Unless indicated otherwise, fulltext items are protected by copyright with all rights reserved. The copyright exception in section 29 of the Copyright, Designs and Patents Act 1988 allows the making of a single copy solely for the purpose of non-commercial research or private study within the limits of fair dealing. The publisher or other rights-holder may allow further reproduction and re-use of this version - refer to the White Rose Research Online record for this item. Where records identify the publisher as the copyright holder, users can verify any specific terms of use on the publisher’s website. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Sartor, P. N., Becker, W., Worden, K., Schmidt, R. K., & Bond, D. (2016). Bayesian Sensitivity Analysis of Flight Parameters in a Hard Landing Analysis Process. Journal of Aircraft, 53(5), 1317-1331.