Collagenous Gastritis: a Case Report, Morphologic Evaluation, and Review Z
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Inflammatory Bowel Disease Irritable Bowel Syndrome
Inflammatory Bowel Disease and Irritable Bowel Syndrome Similarities and Differences 2 www.ccfa.org IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 Important Differences Between IBD and IBS Many diseases and conditions can affect the gastrointestinal (GI) tract, which is part of the digestive system and includes the esophagus, stomach, small intestine and large intestine. These diseases and conditions include inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 www.ccfa.org 3 Inflammatory bowel diseases are a group of inflammatory conditions in which the body’s own immune system attacks parts of the digestive system. Inflammatory Bowel Disease Inflammatory bowel diseases are a group of inflamma- Causes tory conditions in which the body’s own immune system attacks parts of the digestive system. The two most com- The exact cause of IBD remains unknown. Researchers mon inflammatory bowel diseases are Crohn’s disease believe that a combination of four factors lead to IBD: a (CD) and ulcerative colitis (UC). IBD affects as many as 1.4 genetic component, an environmental trigger, an imbal- million Americans, most of whom are diagnosed before ance of intestinal bacteria and an inappropriate reaction age 35. There is no cure for IBD but there are treatments to from the immune system. Immune cells normally protect reduce and control the symptoms of the disease. the body from infection, but in people with IBD, the immune system mistakes harmless substances in the CD and UC cause chronic inflammation of the GI tract. CD intestine for foreign substances and launches an attack, can affect any part of the GI tract, but frequently affects the resulting in inflammation. -

Dyspepsia (Indigestion)
Indigestion (dydpepsia). Indigestion information - Patient | Patient Page 1 of 5 View this article online at https://patient.info/health/dyspepsia-indigestion Dyspepsia (Indigestion) Dyspepsia (indigestion) is a term which describes pain and sometimes other symptoms which come from your upper gut (the stomach, oesophagus or duodenum). There are various causes (described below). Treatment depends on the likely cause. Understanding digestion Food passes down the gullet (oesophagus) into the stomach. The stomach makes acid which is not essential but helps to digest food. Food then passes gradually into the first part of the small intestine (the duodenum). In the duodenum and the rest of the small intestine, food mixes with chemicals called enzymes. The enzymes come from the pancreas and from cells lining the intestine. The enzymes break down (digest) the food. Digested food is then absorbed into the body from the small intestine. What is dyspepsia? Dyspepsia is a term which includes a group of symptoms that come from a problem in your upper gut. The gut (gastrointestinal tract) is the tube that starts at the mouth and ends at the anus. The upper gut includes the oesophagus, stomach and duodenum. Various conditions cause dyspepsia. The main symptom is usually pain or discomfort in the upper tummy (abdomen). In addition, other symptoms that may develop include: • Bloating. • Belching. • Quickly feeling full after eating. • Feeling sick (nausea). • Being sick (vomiting). Symptoms are often related to eating. Doctors used to include heartburn (a burning sensation felt in the lower chest area) and bitter-tasting liquid coming up into the back of the throat (sometimes called 'waterbrash') as symptoms of dyspepsia. -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
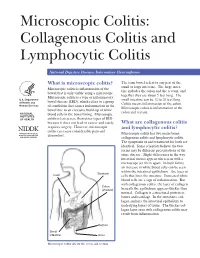
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -

Abdominal Pain - Gastroesophageal Reflux Disease
ACS/ASE Medical Student Core Curriculum Abdominal Pain - Gastroesophageal Reflux Disease ABDOMINAL PAIN - GASTROESOPHAGEAL REFLUX DISEASE Epidemiology and Pathophysiology Gastroesophageal reflux disease (GERD) is one of the most commonly encountered benign foregut disorders. Approximately 20-40% of adults in the United States experience chronic GERD symptoms, and these rates are rising rapidly. GERD is the most common gastrointestinal-related disorder that is managed in outpatient primary care clinics. GERD is defined as a condition which develops when stomach contents reflux into the esophagus causing bothersome symptoms and/or complications. Mechanical failure of the antireflux mechanism is considered the cause of GERD. Mechanical failure can be secondary to functional defects of the lower esophageal sphincter or anatomic defects that result from a hiatal or paraesophageal hernia. These defects can include widening of the diaphragmatic hiatus, disturbance of the angle of His, loss of the gastroesophageal flap valve, displacement of lower esophageal sphincter into the chest, and/or failure of the phrenoesophageal membrane. Symptoms, however, can be accentuated by a variety of factors including dietary habits, eating behaviors, obesity, pregnancy, medications, delayed gastric emptying, altered esophageal mucosal resistance, and/or impaired esophageal clearance. Signs and Symptoms Typical GERD symptoms include heartburn, regurgitation, dysphagia, excessive eructation, and epigastric pain. Patients can also present with extra-esophageal symptoms including cough, hoarse voice, sore throat, and/or globus. GERD can present with a wide spectrum of disease severity ranging from mild, intermittent symptoms to severe, daily symptoms with associated esophageal and/or airway damage. For example, severe GERD can contribute to shortness of breath, worsening asthma, and/or recurrent aspiration pneumonia. -
Practical Approach to Microscopic Colitis and Inflammatory Bowel Disease
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #15 Seymour Katz, M.D., Series Editor Practical Approach to Microscopic Colitis and Inflammatory Bowel Disease by Noel R. Fajardo and Darrell S. Pardi INTRODUCTION The prevalence of IBD, on the other hand, is higher nflammatory disorders of the intestines can be than microscopic colitis, reflecting the younger age of divided into those with macroscopic mucosal onset in patients with IBD. Ichanges (the traditional inflammatory bowel dis- In North America, the incidence of microscopic eases: ulcerative colitis and Crohn’s disease) and those colitis was 0.8/100,000 person-years from 1985 to with primarily microscopic changes. 1989, and this increased significantly to19.1/100,000 Microscopic colitis is a chronic diarrheal condi- from 1998 to 2001 (1). The incidence of collagenous tion that is separated into two main subtypes: collage- colitis and lymphocytic colitis was 5.1 and 9.8/100,000 nous colitis and lymphocytic colitis. These two condi- person-years, and the prevalence was 36 and tions have similar clinical and histologic features, but 64/100,000 persons, respectively (1). In Europe, the are distinguished by the presence or absence of a incidence of collagenous and lymphocytic colitis ranges thickened subepithelial collagen band. Inflammatory from 0.6 to 5.2/100,000 person-years with a prevalence bowel disease (IBD) is traditionally separated into two between 10 to 16/100,000 persons (2). The reason for distinct clinical entities: Crohn’s disease and ulcera- the significantly higher incidence and prevalence of MC tive colitis. Although there is considerable symptom in North America compared with Europe is not known, overlap between these diseases, there are several fea- though increasing recognition may play a role. -

Chronic Viral Hepatitis in a Cohort of Inflammatory Bowel Disease
pathogens Article Chronic Viral Hepatitis in a Cohort of Inflammatory Bowel Disease Patients from Southern Italy: A Case-Control Study Giuseppe Losurdo 1,2 , Andrea Iannone 1, Antonella Contaldo 1, Michele Barone 1 , Enzo Ierardi 1 , Alfredo Di Leo 1,* and Mariabeatrice Principi 1 1 Section of Gastroenterology, Department of Emergency and Organ Transplantation, University “Aldo Moro” of Bari, 70124 Bari, Italy; [email protected] (G.L.); [email protected] (A.I.); [email protected] (A.C.); [email protected] (M.B.); [email protected] (E.I.); [email protected] (M.P.) 2 Ph.D. Course in Organs and Tissues Transplantation and Cellular Therapies, Department of Emergency and Organ Transplantation, University “Aldo Moro” of Bari, 70124 Bari, Italy * Correspondence: [email protected]; Tel.: +39-080-559-2925 Received: 14 September 2020; Accepted: 21 October 2020; Published: 23 October 2020 Abstract: We performed an epidemiologic study to assess the prevalence of chronic viral hepatitis in inflammatory bowel disease (IBD) and to detect their possible relationships. Methods: It was a single centre cohort cross-sectional study, during October 2016 and October 2017. Consecutive IBD adult patients and a control group of non-IBD subjects were recruited. All patients underwent laboratory investigations to detect chronic hepatitis B (HBV) and C (HCV) infection. Parameters of liver function, elastography and IBD features were collected. Univariate analysis was performed by Student’s t or chi-square test. Multivariate analysis was performed by binomial logistic regression and odds ratios (ORs) were calculated. We enrolled 807 IBD patients and 189 controls. Thirty-five (4.3%) had chronic viral hepatitis: 28 HCV (3.4%, versus 5.3% in controls, p = 0.24) and 7 HBV (0.9% versus 0.5% in controls, p = 0.64). -

Gastritis - Symptoms and Causes - Mayo Clinic Visited 11/22/2019
Gastritis - Symptoms and causes - Mayo Clinic Visited 11/22/2019 Request an Appointment Find a Doctor MENU Find a Job Give Now Log in to Patient Account English Patient Care & Health Information Diseases & Conditions Request an Gastritis Appointment Symptoms & causes Diagnosis & treatment Doctors & departments Overview Print Advertisement Gastritis is a general term for a group Mayo Clinic does not endorse companies or of conditions with one thing in common: products. Advertising revenue supports our not- inflammation of the lining of the for-profit mission. stomach. The inflammation of gastritis Advertising & Sponsorship is most often the result of infection with Policy Opportunities Ad Choices the same bacterium that causes most stomach ulcers. Regular use of certain Stomach and pain relievers and drinking too much pyloric valve Mayo Clinic Marketplace alcohol also can contribute to gastritis. Check out these best-sellers and special offers on books and newsletters from Mayo Clinic. Gastritis may occur suddenly (acute gastritis), or appear slowly over time (chronic gastritis). In some cases, gastritis NEW – Guide to Fibromyalgia can lead to ulcers and an increased risk of stomach cancer. Instant access – Mayo Clinic Health Letter For most people, however, gastritis isn't serious and improves quickly with treatment. Diabetes? This diet works … Stop osteoporosis in its tracks The Mayo Clinic Diet Online Products & Services Book: Mayo Clinic on Digestive Health https://www.mayoclinic.org/diseases-conditions/gastritis/symptoms-causes/syc-20355807[11/22/2019 4:16:25 PM] Gastritis - Symptoms and causes - Mayo Clinic Visited 11/22/2019 Symptoms The signs and symptoms of gastritis include: Gnawing or burning ache or pain (indigestion) in your upper abdomen that may become either worse or better with eating Nausea Vomiting A feeling of fullness in your upper abdomen after eating Gastritis doesn't always cause signs and symptoms. -

Gastroesophageal Reflux Disease (GERD)
Guidelines for Clinical Care Quality Department Ambulatory GERD Gastroesophageal Reflux Disease (GERD) Guideline Team Team Leader Patient population: Adults Joel J Heidelbaugh, MD Objective: To implement a cost-effective and evidence-based strategy for the diagnosis and Family Medicine treatment of gastroesophageal reflux disease (GERD). Team Members Key Points: R Van Harrison, PhD Diagnosis Learning Health Sciences Mark A McQuillan, MD History. If classic symptoms of heartburn and acid regurgitation dominate a patient’s history, then General Medicine they can help establish the diagnosis of GERD with sufficiently high specificity, although sensitivity Timothy T Nostrant, MD remains low compared to 24-hour pH monitoring. The presence of atypical symptoms (Table 1), Gastroenterology although common, cannot sufficiently support the clinical diagnosis of GERD [B*]. Testing. No gold standard exists for the diagnosis of GERD [A*]. Although 24-hour pH monitoring Initial Release is accepted as the standard with a sensitivity of 85% and specificity of 95%, false positives and false March 2002 negatives still exist [II B*]. Endoscopy lacks sensitivity in determining pathologic reflux but can Most Recent Major Update identify complications (eg, strictures, erosive esophagitis, Barrett’s esophagus) [I A]. Barium May 2012 radiography has limited usefulness in the diagnosis of GERD and is not recommended [III B*]. Content Reviewed Therapeutic trial. An empiric trial of anti-secretory therapy can identify patients with GERD who March 2018 lack alarm or warning symptoms (Table 2) [I A*] and may be helpful in the evaluation of those with atypical manifestations of GERD, specifically non-cardiac chest pain [II B*]. Treatment Ambulatory Clinical Lifestyle modifications. -

Ulcerative Colitis: Diagnosis and Treatment ROBERT C
Ulcerative Colitis: Diagnosis and Treatment ROBERT C. LANGAN, MD; PATRICIA B. GOTSCH, MD; MICHAEL A. KRAFCZYK, MD; and DAVID D. SKILLINGE, DO, St. Luke’s Family Medicine Residency, Bethlehem, Pennsylvania Ulcerative colitis is a chronic disease with recurrent symptoms and significant morbidity. The precise etiology is still unknown. As many as 25 percent of patients with ulcerative colitis have extraintestinal manifestations. The diagnosis is made endoscopically. Tests such as perinuclear antineutrophilic cytoplasmic antibodies and anti-Saccharomyces cerevisiae antibodies are promising, but not yet recommended for routine use. Treatment is based on the extent and severity of the disease. Rectal therapy with 5-aminosalicylic acid compounds is used for proc- titis. More extensive disease requires treatment with oral 5-aminosalicylic acid compounds and oral corticosteroids. The side effects of steroids limit their usefulness for chronic therapy. Patients who do not respond to treatment with oral corticosteroids require hospitalization and intravenous steroids. Refractory symptoms may be treated with azathioprine or infliximab. Surgical treatment of ulcerative colitis is reserved for patients who fail medical therapy or who develop severe hemorrhage, perforation, or cancer. Longstanding ulcerative colitis is associated with an increased risk of colon cancer. Patients should receive an initial screening colonos- copy eight years after the onset of pancolitis and 12 to 15 years after the onset of left-sided dis- ease; follow-up colonoscopy should be repeated every two to three years. (Am Fam Physician 2007;76:1323-30, 1331. Copyright © 2007 American Academy of Family Physicians.) This article exempli- lcerative colitis is a chronic dis- of ulcerative colitis is not well understood. -

Liver Disease in Ulcerative Colitis: an Epidemiological and Follow up Study
84 Gut 1994; 35:84-89 Liver disease in ulcerative colitis: an epidemiological and follow up study in the county of Stockholm Gut: first published as 10.1136/gut.35.1.84 on 1 January 1994. Downloaded from U Broome, H Glaumann, G Hellers, B Nilsson, J Sorstad, R Hultcrantz Abstract sclerosing cholangitis (PSC) are said to be more In an epidemiological study ofthe incidence of common in patients with UC.47 The incidence of ulcerative colitis (UC) in the county of Stock- these complications varies in different studies holm between 1955 and 1979, 1274 patients depending on selection criteria and on the with UC were discovered. Almost all these definition of hepatobiliary disease.89 The true patients had regularly been investigated with incidence of hepatobiliary dysfunction in UC, liver function tests; 142 (11%) of them showed however, can only be obtained by tests of liver signs of hepatobiliary disease. A follow up function tests such as transaminases, alkaline study on all 142 patients with abnormal liver phosphatases, and bilirubin made routinely in function and UC was made between 1989 and unselected groups of patients with UC. Because 1991 to evaluate the cause of the liver abnor- the cause of hepatic involvement in UC is mality and to find out if the liver disease had enigmatic it is important to find out if the rate affected the survival rates. At follow up, eight of this complication is increasing, because of patients were reclassified as having Crohn's factors unrelated to UC, or if it mirrors the disease, 60 had developed normal liver func- incidence ofUC in itself. -
Familial Occurrence of Lymphocytic Colitis
BRIEF COMMUNICATION Familial occurrence of lymphocytic colitis Hugh J Freeman MD HJ Freeman. Familial occurrence of lymphocytic colitis. Can J Occurrence familiale de la colite Gastroenterol 2001;15(11):757-760. The familial occurrence lymphocytaire of lymphocytic colitis in a female parent and her two female children is reported. No other genetically based disorder, includ- RÉSUMÉ : On fait ici état de l’occurrence familiale de la colite lym- ing celiac disease, was evident. For both children, the age of phocytaire chez une patiente et ses deux filles. Aucune autre maladie diagnosis was more than two decades younger than the age of d’origine génétique, comme la maladie cæliaque, ne s’est manifestée. recognition of disease in the parent, and some clinical features, Pour les deux enfants, le diagnostic a été posé plus d’une vingtaine d’an- including the requirement for pharmacological agents in both nées avant l’âge qu’avait la mère au moment de son diagnostic et cer- taines caractéristiques cliniques, dont le traitement pharmacologique children, suggested that their disease severity was more signifi- chez les deux enfants, donnent à penser que leur maladie est plus grave cant than that of the involved parent. These characteristics of a que chez le parent atteint. Ces caractéristiques de la maladie familiale familial disease have been previously reported and labelled ont déjà été mentionnées et ont été appelées "anticipation génétique" ‘genetic anticipation’ in some monogenetic forms of neurologi- dans le cas de certaines formes monogénétiques de maladies neu- cal disease, as well as in other types of inflammatory bowel dis- rologiques, de même que dans d’autres types de maladies inflammatoires eases, including Crohn’s disease. -

In Patients with Crohn's Disease Gut: First Published As 10.1136/Gut.38.3.379 on 1 March 1996
Gut 1996; 38: 379-383 379 High frequency of helicobacter negative gastritis in patients with Crohn's disease Gut: first published as 10.1136/gut.38.3.379 on 1 March 1996. Downloaded from L Halme, P Karkkainen, H Rautelin, T U Kosunen, P Sipponen Abstract In a previous study we described upper gastro- The frequency of gastric Crohn's disease intestinal lesions characteristic of CD in 17% has been considered low. This study was of patients with ileocolonic manifestations of undertaken to determine the prevalence of the disease.10 Furthermore, 40% of these chronic gastritis and Helicobacter pylori patients had chronic, non-specific gastritis. infection in patients with Crohn's disease. This study aimed to determine the prevalence Oesophagogastroduodenoscopy was per- of chronic gastritis and that of H pylori infec- formed on 62 consecutive patients suffer- tion in patients with CD who had undergone ing from ileocolonic Crohn's disease. oesophagogastroduodenoscopy (OGDS) at the Biopsy specimens from the antrum and Fourth Department of Surgery, Helsinki corpus were processed for both histological University Hospital between 1989 and 1994. and bacteriological examinations. Hpylori antibodies of IgG and IgA classes were measured in serum samples by enzyme Patients and methods immunoassay. Six patients (9.70/o) were During a five year period from September 1989 infected with H pylorn, as shown by histo- to August 1994, OGDS was performed on 62 logy, and in five of them the infection consecutive patients with CD to establish the was also verified by serology. Twenty one distribution of their disease. During the study patients (32%) had chronic H pyloni period, the OGDS was repeated (one to seven negative gastritis (negative by both times) - on three patients because of anaemia histology and serology) and one of them and on five patients because of upper gastroin- also had atrophy in the antrum and corpus.