Clinical and Pathological Aspects of Inflammatory Bowel Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
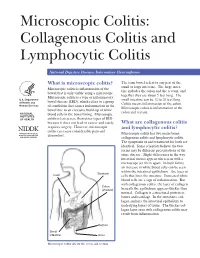
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -

Picquestion of the Week:3/09/09
McKechnie Field - Spring Training Home of the Pirates PIC QUESTION OF THE WEEK: 3/09/09 Q: Why is rifaximin used in patients with pouchitis? A: Pouchitis is an inflammation of the internal pouch fashioned from small intestinal tissue during ileal pouch anal anastamosis (IPAA). This surgical procedure bypasses the large intestine and may be employed in patients with ulcerative colitis or Crohn’s disease. A temporary ileostomy is placed to allow the pouch to heal without risk of infection. IPAA is considered preferable to an ostomy for patients suffering from inflammatory bowel diseases refractory to medical treatment. The pouch serves as a collection device for waste, but permits the patient to experience regular bowel movements. It is typical for patients with an internal pouch to experience more frequent (average 6 per day) and watery bowel movements. Pouchitis is the most common complication of IPAA and widely regarded as an idiopathic disease; however, colonization by fecal bacteria may be a contributing factor. The condition occurs most commonly in the first six months following reversal of the ileostomy. Although its frequency decreases after six months, nearly 50% of patients with an IPAA will eventually experience pouchitis. Presenting symptoms include diarrhea, increased frequency of bowel movements, bleeding, abdominal pain, and fever. It can result in dehydration and, in severe cases, hospitalization. Treatment of acute pouchitis generally consists of a two-week course of antibiotic therapy with metronidazole or ciprofloxacin. Approximately 10% of patients do not respond to initial treatment and develop chronic (> 4 weeks) pouchitis. A small number of clinical trials support the potential use of rifaximin for the treatment of refractory or recurrent pouchitis. -

Pouchitis in Pediatric Ulcerative Colitis: a Multicenter Study on Behalf
Digestive and Liver Disease 51 (2019) 1551–1556 Contents lists available at ScienceDirect Digestive and Liver Disease jou rnal homepage: www.elsevier.com/locate/dld Alimentary Tract Pouchitis in pediatric ulcerative colitis: A multicenter study on behalf of Italian Society of Pediatric Gastroenterology, Hepatology and Nutrition a b b c Valeria Dipasquale , Girolamo Mattioli , Serena Arrigo , Matteo Bramuzzo , d e e e Caterina Strisciuglio , Simona Faraci , Erminia Francesca Romeo , Anna Chiara Contini , f g h i a,∗ Marco Ventimiglia , Giovanna Zuin , Enrico Felici , Patrizia Alvisi , Claudio Romano a Pediatric Gastroenterology and Cystic Fibrosis Unit, University of Messina, Messina, Italy b Pediatric Surgery Unit, Giannina Research Institute and Children Hospital, Genova, Italy c Pediatric Department, Gastroenterology, Digestive Endoscopy and Nutrition Unit, Institute for Maternal and Child Health, IRCCS “Burlo Garofalo”, Trieste, Italy d Department of Woman, Child and General and Specialistic Surgery, University of Campania “Luigi Vanvitelli”, Naples, Italy e Digestive Endoscopy and Surgery Unit, Bambino Gesù Children’s Hospital IRCCS, Rome, Italy f Inflammatory Bowel Disease Unit, “Villa Sofia-Cervello” Hospital, Palermo, Italy g Pediatric Department, University of Milano Bicocca, FMBBM, San Gerardo Hospital, Monza, Italy h Unit of Pediatrics and “Umberto Bosio” Center for Digestive Diseases, The Children Hospital, AON SS Antonio e Biagio e Cesare Arrigo, Alessandria, Italy i Pediatric Gastroenterology Unit, Maggiore Hospital, Bologna, Italy a r t i c l e i n f o a b s t r a c t Article history: Background: Data on the epidemiology and risk factors for pouchitis following restorative Received 27 April 2019 proctocolectomy and ileal pouch-anal anastomosis (IPAA) in pediatric patients with ulcerative colitis Accepted 27 June 2019 (UC) are scarce. -

Second European Evidence-Based Consensus on the Diagnosis and Management of Ulcerative Colitis: Special Situations
CROHNS-00649; No of Pages 33 Journal of Crohn's and Colitis (2012) xx, xxx–xxx Available online at www.sciencedirect.com SPECIAL ARTICLE Second European evidence-based consensus on the diagnosis and management of ulcerative colitis: Special situations Gert Van Assche⁎,1,2, Axel Dignass⁎⁎,2, Bernd Bokemeyer1, Silvio Danese1, Paolo Gionchetti1, Gabriele Moser1, Laurent Beaugerie1, Fernando Gomollón1, Winfried Häuser1, Klaus Herrlinger1, Bas Oldenburg1, Julian Panes1, Francisco Portela1, Gerhard Rogler1, Jürgen Stein1, Herbert Tilg1, Simon Travis1, James O. Lindsay1 Received 30 August 2012; accepted 3 September 2012 KEYWORDS Ulcerative colitis; Anaemia; Pouchitis; Colorectal cancer surveillance; Psychosomatic; Extraintestinal manifestations Contents 8. Pouchitis ............................................................ 0 8.1. General ......................................................... 0 8.1.1. Symptoms ................................................... 0 ⁎ Correspondence to: G. Van Assche, Division of Gastroenterology, Department of Medicine, Mt. Sinai Hospital and University Health Network, University of Toronto and University of Leuven, 600 University Avenue, Toronto, ON, Canada M5G 1X5. ⁎⁎ Correspondence to: A. Dignass, Department of Medicine 1, Agaplesion Markus Hospital, Wilhelm-Epstein-Str. 4, D-60431 Frankfurt/Main, Germany. E-mail addresses: [email protected] (G. Van Assche), [email protected] (A. Dignass). 1 On behalf of ECCO. 2 G.V.A. and A.D. acted as convenors of the consensus and contributed equally to this paper. 1873-9946/$ - see front matter © 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.crohns.2012.09.005 Please cite this article as: Van Assche G, et al, Second European evidence-based consensus on the diagnosis and management of ulcerative colitis: Special situations, Journal of Crohn's and Colitis (2012), http://dx.doi.org/10.1016/j.crohns.2012.09.005 2 G. -
Calprotectin Could Be a Potential Biomarker for Acute Appendicitis Peter C
Ambe et al. J Transl Med (2016) 14:107 DOI 10.1186/s12967-016-0863-3 Journal of Translational Medicine RESEARCH Open Access Calprotectin could be a potential biomarker for acute appendicitis Peter C. Ambe1*, Daniel Gödde2, Lars Bönicke1, Marios Papadakis1, Stephan Störkel2 and Hubert Zirngibl1 Abstract Background: Acute appendicitis is a common cause for a visit to the emergency department and appendectomy represents the most common emergency procedure in surgery. The rate of negative appendectomy however has remained high despite modern diagnostic apparatus. Therefore, there is need for a better preoperative screening of patients with suspected appendicitis. Calprotectin represents a predominant protein in the cytosol of neutrophil granulocytes and has been extensively investigated with regard to bowel pathologies. This study investigates the expression of calprotectin in the lumen of the vermiform appendix of patients undergoing appendectomy for sus- pected appendicitis. Methods: Appendix specimens from patients undergoing emergency appendectomy for suspected acute appendi- citis were examined. Acute appendicitis was confirmed on histopathology. The qualitative expression of calprotectin in the vermiform appendix specimens was analyzed using specific calprotectin antibodies. Results: Vermiform appendix specimens from 52 patients (22 female and 30 male) including 11 with uncomplicated and 41 with complicated appendicitis were analyzed. Strong immunostainings were achieved with calprotectin antibody in the lumen of all specimens irrespective of the extent of appendicitis. Immunostaining was negative in the uninflamed appendix. Conclusions: High calprotectin activity could be demonstrated within the lumen of vermiform appendix specimens following appendectomy for acute appendicitis. The high luminal accumulation of calprotectin-carrying cells could be interpreted as an invitation to study the expression of calprotectin in stool as a new diagnostic aid in patients with suspected appendicitis. -

Associated Ulcerative Colitis, Sclerosing Cholangitis, and Insulin*Dependent Diabetes Mellitus
CASE REPORT Associated ulcerative colitis, sclerosing cholangitis, and insulin*dependent diabetes mellitus MARSHA KAY, MD; ROBERT WYLLIE, MD; WILLIAM MICHENER, MD; MAUREEN CAULFIELD, MD; RITA STEFFEN, MD LINICALLY symptomatic We report two young men with clinical and laboratory evidence ulcerative colitis, sclero- of macroscopic ulcerative colitis, sclerosing cholangitis, and insu- sing cholangitis, and in- lin-dependent diabetes mellitus. The first patient presented at age Csulin-dependent diabe- 15 with vomiting, abdominal pain, weight loss, and abnormal tes mellitus have not previously liver function test results. Liver biopsy and endoscopic retrograde been reported in the same patient. cholangiopancreatography (ERCP) demonstrated sclerosing cho- Although each may be associated langitis. Colonoscopy with biopsy revealed ulcerative colitis with the other, their occurrence in which responded to sulfasalazine. Diabetes occurred at age 18 and the same individual implies a com- insulin therapy was begun. mon susceptibility, perhaps involv- The second patient was 19 at presentation with diarrhea, hema- ing the immune system. We have tochezia, and weight loss. Proctosigmoidoscopy revealed identified two patients with each ulcerative colitis, and sulfasalazine led to clinical remission. Three of these disorders. These two months later he developed diabetes requiring insulin therapy. At young men were followed up at age 28, he developed elevated alkaline phosphatase, and ERCP re- The Cleveland Clinic Foundation vealed sclerosing cholangitis. At age 37 he expired from adenocar- between 1970 and 1992. cinoma that metastasized to the liver. Literature review revealed only one possible case report of this PATIENT I; CASE HISTORY association with microscopic asymptomatic ulcerative colitis in that patient. Statistical analysis suggests that this association is Patient 1 presented at age 15 real rather than a chance occurrence. -
Microscopic Colitis
From Department of Medicine, Solna Karolinska Institutet, Stockholm, Sweden MICROSCOPIC COLITIS Marie-Rose Mellander Stockholm 2017 All previously published papers were reproduced with permission from the publisher. Published by Karolinska Institutet. Printed by Eprint AB 2017 © Marie-Rose Mellander, 2017 ISBN 978-91-7676-586-9 Microscopic colitis THESIS FOR DOCTORAL DEGREE (Ph.D.) By Marie-Rose Mellander Principal Supervisor: Opponent: Rolf Hultcrantz Marie Carlson Karolinska Institutet Uppsala University Department of Medicine, Huddinge Department of Medical Sciences; Gastroenterology/Hepatology Co-supervisors: Jan Björk Examination Board: Karolinska Institutet Catarina Almqvist Malmros Department of Medicine, Solna Karolinska Institutet Department of Medical Epidemiology and Robert Löfberg Biostatistics Karolinska Institutet Department of Medicine, Solna Kjell-Arne Ung University of Gothenburg Anders Ekbom Department of Medicine, Sahlgrenska Karolinska Institutet Department of Medicine, Solna Anders Höög Karolinska Institutet Department of Oncology-Pathology To my daughters Julia, Tilda and Sara ABSTRACT Microscopic colitis (MC) is an inflammatory bowel disease (IBD) and a common cause of chronic non-bloody diarrhoea, especially in elderly women. There are two main subtypes, lymphocytic colitis (LC) and collagenous colitis (CC) which are clinically indistinguishable and can be separated only by their characteristic histopathological features. The colonoscopy is usually macroscopically normal although subtle mucosal changes have been reported. The aetiology of MC is unknown and the genetic factors are poorly investigated. This thesis aims to describe MC in a large urban cohort and compare LC and CC regarding clinical and endoscopic features, both at diagnosis and at follow-up (F-U), and to observe the occurrence of coeliac disease, ulcerative colitis (UC) and Crohn’s disease (CD). -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
A SPECIAL ARTICLE Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis Brennan A. Scott Thomas P. Prindiville Collagenous colitis and lymphocytic colitis are chronic relapsing diarrheal illnesses, which are often referred to together as microscopic colitis. It most commonly occurs in women in their fifth to sixth decade. The symptoms usually include profuse watery diarrhea and crampy abdominal pain. Laboratory and endoscopic studies are gener- ally normal but microscopic inflammation is seen when colonic biopsies are performed. In collagenous colitis there is a subepithelial collagen band in addition to chronic inflammation in the lamina propria. The etiology is not known but multiple theories exist including autoimmune, infectious, and medication-induced. Although the course is generally benign, patients may have multiple relapses over many years. Treatment regimens vary and have included anti-diarrheals, antibiotics, 5-aminosalicylates, steroids, and immunosuppressive agents. INTRODUCTION abdominal pain. Both conditions have normal mucosa ollagenous colitis (CC) (Figure 1) and lympho- when viewed endoscopically, however biopsy speci- cytic colitis (LC) (Figure 2) are uncommon mens show chronic mucosal inflammation. In CC C chronic relapsing diarrheal illnesses. The major- there is a subepithelial collagen band of varying thick- ity of patients are women in their fifth to sixth decade ness in association with an inflammatory cell infiltrate who complain of profuse, watery diarrhea, and crampy in the lamina propria (1). The collagen band is absent in LC (2,3). The term microscopic colitis (MC) was Brennan A. Scott, MD, Clinical Fellow, Division of Gas- originally used to describe patients with chronic diar- troenterology, University of California, Davis Medical rhea and normal endoscopic and barium enema stud- Center. -
Microscopic Colitis Collagenous and Lymphocytic Colitis Publisher
The informed patient Microscopic colitis Collagenous and lymphocytic colitis Publisher © 2020 Dr. Falk Pharma GmbH 6th updated and All rights reserved. revised edition 2020 The informed patient Microscopic colitis Collagenous and lymphocytic colitis Prof. Dr. Andreas Tromm, Hattingen (Germany) Microscopic colitis – Collagenous and lymphocytic colitis Address of the author Prof. Dr. Andreas Tromm Klinik für Innere Medizin Augusta-Kranken-Anstalt gGmbH Betriebsstelle EVK Hattingen Akademisches Lehrkrankenhaus der Universität Duisburg-Essen Bredenscheider Str. 54 45525 Hattingen Germany www.klinik-gastroenterologie.de Contents Introduction 4 Clinical presentation 6 Causes and development of microscopic colitis 9 Diagnosis 11 Treatment 14 Frequently asked questions about microscopic colitis 17 3 Microscopic colitis – Collagenous and lymphocytic colitis Introduction The term microscopic colitis encompasses two different disorders of the colon known as collagenous colitis and lymphocytic colitis. Both disorders are characterized by non-bloody watery diarrhea and are sometimes referred to as watery diar- rhea syndromes (Fig. 1). Microscopic colitis Collagenous colitis Lymphocytic colitis Watery diarrhea syndrome Fig. 1: Definition of microscopic colitis. 4 Introduction The term microscopic colitis describes a chronic in- flammatory disease of the colon (“colitis” comes from the Latin term “colon” and the ending “-itis”, which is used in medicine to refer to inflammation) that a doctor cannot identify by colonoscopy with the naked eye because the mucosa of the colon appears normal. In order for the disease to be diagnosed, the doctor must therefore remove a small tissue sample and examine it under a microscope. This is the only way to diagnose microscopic colitis. For collagenous colitis, a thickened collagen layer becomes visible when the tissue samples are stained using special methods, whereas lymphocytic colitis is detected as an increased number of a specific type of white blood cells called lymphocytes (see page 12). -

Microscopic Colitis What Is Microscopic Colitis?
Microscopic Colitis What is microscopic colitis? Microscopic colitis is an inflammation of the colon that a health care provider can see only with a microscope. Inflammation is the body’s normal response to injury, irritation, or infection of tissues. Microscopic colitis is a type of inflammatory bowel disease—the general name for diseases that cause irritation and inflammation in the intestines. The two types of microscopic colitis are collagenous colitis and lymphocytic colitis. Health care providers often use the term microscopic colitis to describe both types because their symptoms and treatments are the same. Some scientists believe that collagenous colitis and lymphocytic colitis may be different phases of the same condition rather than separate conditions. In both types of microscopic colitis, an increase in the number of lymphocytes, a type of white blood cell, can be seen in the epithelium—the layer of cells that lines the colon. An increase in the number of white blood cells is a sign of inflammation. The two types of colitis affect the colon tissue in slightly different ways: Lymphocytic colitis. The number of lymphocytes is higher, and the tissues and lining of the colon are of normal thickness. Collagenous colitis. The layer of collagen, a threadlike protein, underneath the epithelium builds up and becomes thicker than normal. When looking through a microscope, the health care provider may find variations in lymphocyte numbers and collagen thickness in different parts of the colon. These variations may indicate an overlap of the two types of microscopic colitis. What causes microscopic colitis? The exact cause of microscopic colitis is unknown. -

Pouchitis After Ileal Pouch-Anal Anastomosis for Ulcerative Colitis Occurs with Increased Frequency Cholangitis
234 Gut 1996; 38: 234-239 Pouchitis after ileal pouch-anal anastomosis for ulcerative colitis occurs with increased frequency in patients with associated primary sclerosing Gut: first published as 10.1136/gut.38.2.234 on 1 February 1996. Downloaded from cholangitis C Penna, R Dozois, W Tremaine, W Sandborn, N LaRusso, C Schleck, D Ilstrup Abstract of concomitant primary sclerosing cholangitis Primary sclerosing cholangitis (PSC), (PSC), a chronic cholestatic syndrome of present in 5% of patients with ulcerative unknown cause characterised by fibrosing colitis, may be associated with pouchitis obliteration of the bile ducts, seems to be a after ileal pouch-anal anastomosis. The significant risk factor for the development of cumulative frequency of pouchitis in pouchitis.7 patients with and without PSC who To further explore the association between underwent ileal pouch-anal anastomosis PSC and pouchitis, the aims ofthis study were: for ulcerative colitis was determined. A (a) to determine if PSC represents an indepen- total of 1097 patients who had an ileal dent risk factor for pouchitis; (b) to compare pouch-anal anastomosis for ulcerative clinical, endoscopic, and pathological findings colitis, 54 with associated PSC, were of pouchitis in a subset of patients without studied. Pouchitis was defined by clinical PSC; and (c) to search for correlations criteria in all patients and by clinical, between the risk of pouchitis and status of endoscopic, and histological criteria in liver disease. 83% of PSC patients and 85% of their matched controls. PSC was defined by clinical, radiological, and pathological Methods findings. One or more episodes of pouchitis occurred in 32% of patients Patients without PSC and 63% of patients with Between January 1981 and April 1993, 1097 PSC. -
Microscopic Colitis (PDF)
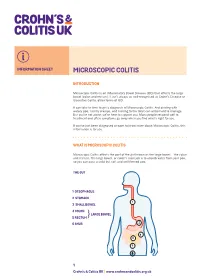
INFORMATION SHEET MICROSCOPIC COLITIS INTRODUCTION Microscopic Colitis is an Inflammatory Bowel Disease (IBD) that affects the large bowel (colon and rectum). It isn’t always as well-recognised as Crohn’s Disease or Ulcerative Colitis, other forms of IBD. It can take to time to get a diagnosis of Microscopic Colitis. And dealing with watery poo, tummy cramps, and rushing to the toilet can all be hard to manage. But you’re not alone; we’re here to support you. Many people respond well to treatment and often symptoms go away when you find what’s right for you. If you’ve just been diagnosed or want to know more about Microscopic Colitis, this information is for you. WHAT IS MICROSCOPIC COLITIS Microscopic Colitis affects the part of the gut known as the large bowel – the colon and rectum. The large bowel, or colon’s main job is to absorb water from your poo, so you can pass a solid but soft and well-formed poo. THE GUT 1 OESOPHAGUS 2 STOMACH 1 3 SMALL BOWEL 2 4 COLON LARGE BOWEL 5 RECTUM} 6 ANUS 2 4 3 5 6 1 Crohn’s & Colitis UK | www.crohnsandcolitis.org.uk MICROSCOPIC COLITIS The walls of your bowel have layers. In Microscopic Colitis the inner lining becomes inflamed. But this change can only be seen when a sample of tissue (biopsy) is taken from your colon and looked at under a microscope. BOWEL LAYERS INNER LINING MIDDLE LAYER OUTER LAYER There are two types of Microscopic Colitis: • Lymphocytic Colitis (LC) – where the inner lining has more white blood cells (lymphocytes) than usual.