European Consensus on the Histopathology of Inflammatory Bowel Disease☆ F
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Communicable Disease Chart
COMMON INFECTIOUS ILLNESSES From birth to age 18 Disease, illness or organism Incubation period How is it spread? When is a child most contagious? When can a child return to the Report to county How to prevent spreading infection (management of conditions)*** (How long after childcare center or school? health department* contact does illness develop?) To prevent the spread of organisms associated with common infections, practice frequent hand hygiene, cover mouth and nose when coughing and sneezing, and stay up to date with immunizations. Bronchiolitis, bronchitis, Variable Contact with droplets from nose, eyes or Variable, often from the day before No restriction unless child has fever, NO common cold, croup, mouth of infected person; some viruses can symptoms begin to 5 days after onset or is too uncomfortable, fatigued ear infection, pneumonia, live on surfaces (toys, tissues, doorknobs) or ill to participate in activities sinus infection and most for several hours (center unable to accommodate sore throats (respiratory diseases child’s increased need for comfort caused by many different viruses and rest) and occasionally bacteria) Cold sore 2 days to 2 weeks Direct contact with infected lesions or oral While lesions are present When active lesions are no longer NO Avoid kissing and sharing drinks or utensils. (Herpes simplex virus) secretions (drooling, kissing, thumb sucking) present in children who do not have control of oral secretions (drooling); no exclusions for other children Conjunctivitis Variable, usually 24 to Highly contagious; -

Dyspepsia (Indigestion)
Indigestion (dydpepsia). Indigestion information - Patient | Patient Page 1 of 5 View this article online at https://patient.info/health/dyspepsia-indigestion Dyspepsia (Indigestion) Dyspepsia (indigestion) is a term which describes pain and sometimes other symptoms which come from your upper gut (the stomach, oesophagus or duodenum). There are various causes (described below). Treatment depends on the likely cause. Understanding digestion Food passes down the gullet (oesophagus) into the stomach. The stomach makes acid which is not essential but helps to digest food. Food then passes gradually into the first part of the small intestine (the duodenum). In the duodenum and the rest of the small intestine, food mixes with chemicals called enzymes. The enzymes come from the pancreas and from cells lining the intestine. The enzymes break down (digest) the food. Digested food is then absorbed into the body from the small intestine. What is dyspepsia? Dyspepsia is a term which includes a group of symptoms that come from a problem in your upper gut. The gut (gastrointestinal tract) is the tube that starts at the mouth and ends at the anus. The upper gut includes the oesophagus, stomach and duodenum. Various conditions cause dyspepsia. The main symptom is usually pain or discomfort in the upper tummy (abdomen). In addition, other symptoms that may develop include: • Bloating. • Belching. • Quickly feeling full after eating. • Feeling sick (nausea). • Being sick (vomiting). Symptoms are often related to eating. Doctors used to include heartburn (a burning sensation felt in the lower chest area) and bitter-tasting liquid coming up into the back of the throat (sometimes called 'waterbrash') as symptoms of dyspepsia. -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
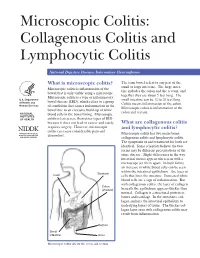
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -

797 Circulating Tumor DNA and Circulating Tumor Cells for Cancer
Medical Policy Circulating Tumor DNA and Circulating Tumor Cells for Cancer Management (Liquid Biopsy) Table of Contents • Policy: Commercial • Coding Information • Information Pertaining to All Policies • Policy: Medicare • Description • References • Authorization Information • Policy History • Endnotes Policy Number: 797 BCBSA Reference Number: 2.04.141 Related Policies Biomarkers for the Diagnosis and Cancer Risk Assessment of Prostate Cancer, #336 Policy1 Commercial Members: Managed Care (HMO and POS), PPO, and Indemnity Plasma-based comprehensive somatic genomic profiling testing (CGP) using Guardant360® for patients with Stage IIIB/IV non-small cell lung cancer (NSCLC) is considered MEDICALLY NECESSARY when the following criteria have been met: Diagnosis: • When tissue-based CGP is infeasible (i.e., quantity not sufficient for tissue-based CGP or invasive biopsy is medically contraindicated), AND • When prior results for ALL of the following tests are not available: o EGFR single nucleotide variants (SNVs) and insertions and deletions (indels) o ALK and ROS1 rearrangements o PDL1 expression. Progression: • Patients progressing on or after chemotherapy or immunotherapy who have never been tested for EGFR SNVs and indels, and ALK and ROS1 rearrangements, and for whom tissue-based CGP is infeasible (i.e., quantity not sufficient for tissue-based CGP), OR • For patients progressing on EGFR tyrosine kinase inhibitors (TKIs). If no genetic alteration is detected by Guardant360®, or if circulating tumor DNA (ctDNA) is insufficient/not detected, tissue-based genotyping should be considered. Other plasma-based CGP tests are considered INVESTIGATIONAL. CGP and the use of circulating tumor DNA is considered INVESTIGATIONAL for all other indications. 1 The use of circulating tumor cells is considered INVESTIGATIONAL for all indications. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Medical Microbiology and Infectious Diseases 22% Specialists in 2017 = 11%3
Medical Microbiology & Infectious Diseases Profile Updated December 2019 1 Table of Contents Slide . General Information 3-5 . Total number & number/100,000 population by province, 2019 6 . Number/100,000 population, 1995-2019 7 . Number by gender & year, 1995-2019 8 . Percentage by gender & age, 2019 9 . Number by gender & age, 2019 10 . Percentage by main work setting, 2019 11 . Percentage by practice organization, 2017 12 . Hours worked per week (excluding on-call), 2019 13 . On-call duty hours per month, 2019 14 . Percentage by remuneration method 15 . Professional & work-life balance satisfaction, 2019 16 . Number of retirees during the three year period of 2016-2018 17 . Employment situation, 2017 18 . Links to additional resources 19 2 General information Microbiology and infectious diseases focuses on the diagnosis and treatment of infectious diseases; thus, it is concerned with human illness due to micro-organisms. Since such disease can affect any and all organs and systems, this specialist must be prepared to deal with any region of the body. The specialty of Medical Microbiology and Infectious Disease consists primarily of four major spheres of activity: 1. the provision of clinical consultations on the investigation, diagnosis and treatment of patients suffering from infectious diseases; 2. the establishment and direction of infection control programs across the continuum of care; 3. public health and communicable disease prevention and epidemiology; 4. the scientific and administrative direction of a diagnostic microbiology laboratory. Source: Pathway evaluation program 3 General information Once you’ve completed medical school, it takes an additional 5 years of Royal College-approved residency training to become certified in medical microbiology and infectious disease. -

Abnormal Small Bowel Permeability and Duodenitis in Recurrent Abdominal Pain
Archives ofDisease in Childhood 1990; 65: 1311-1314 1311 Abnormal small bowel permeability and duodenitis Arch Dis Child: first published as 10.1136/adc.65.12.1311 on 1 December 1990. Downloaded from in recurrent abdominal pain S B van der Meer, P P Forget, J W Arends Abstract assess the value of 5"Cr-EDTA permeability Thirty nine children with recurrent abdominal tests of intestinal inflammation. As the absorp- pain aged between 5.5 and 12 years, underwent tion of 51Cr-EDTA takes place predominantly endoscopic duodenal biopsy to find out if in the small bowel,'2 duodenal biopsies from 39 there were any duodenal inflammatory patients with recurrent abdominal pain were changes, and if there was a relationship examined for the presence of inflammatory between duodenal inflammation and intestinal changes. permeability to 5tCr-EDTA. Duodenal in- flammation was graded by the duodenitis scale of Whitehead et al (grade 0, 1, 2, and 3). Patients and methods In 13 out of 39 patients (33%) definite signs of During a prospective study 106 children with inflammation were found (grade 2 and 3). recurrent abdominal pain were investigated Intestinal permeability to 5tCr-EDTA in according to a standard protocol. Patients were patients with duodenitis (grade 1, 2, and 3) diagnosed as having recurrent abdominal pain if was significantly higher (4-42 (1-73)%) than in they were aged between 5 5 and 12 years; had patients with normal (grade 0) duodenal had recurrent abdominal pain for at least six biopsy appearances (3.3 (0-9)%). A significant months; had had attacks of pain varying in association was found between duodenal in- severity, duration, and frequency; and if their flammation and abnormal intestinal per- attacks were sometimes accompanied by pale- meability. -

Diagnostic Tests Diagnostic Tests Attempt to Classify Whether Somebody Has a Disease Or Not Before Symptoms Are Present
community project encouraging academics to share statistics support resources All stcp resources are released under a Creative Commons licence stcp-rothwell-diagnostictests Diagnostic Tests Diagnostic tests attempt to classify whether somebody has a disease or not before symptoms are present. We are interested in detecting the disease early, while it is still curable. However, there is a need to establish how good a diagnostic test is in detecting disease. In this situation a 2x2 table similar to the below would be produced to test how effective a diagnostic test is at predicting the outcome of interest. A number of different measures can be calculated from this information. True Diagnosis Disease +ve Disease -ve Total Test Results +ve a b a+b -ve c d c+d a+c b+d N = This is the proportion of diseased individuals that are correctly Sensitivity: ( ) identified by the test as having the disease. (+ | ) + = This is the proportion of non-diseased individuals that Specificity: ( ) are correctly identified by the test as not having the disease. ( | ) + = This is the proportion − of individuals with Positive Predictive Value**: ( ) positive test results that are correctly diagnosed and actually have the disease. ( | + ) + = This is the proportion of individuals with Negative Predictive Value**: ( ) negative test results that are correctly diagnosed and do not have the disease. ( | + ) − © Joanne Rothwell Reviewer: Chris Knox University of Sheffield University of Sheffield Medical Statistics – diagnostic tests Positive Likelihood Ratio: = This gives a ratio of the test being positive + for patients with disease compared with those without disease. Aim to be much greater − than 1 for a good test. -

~L.Il~I~1 ORGANISATION MONDIALE ORGANIZATION DE LA SANTE ~,JII /'1 'IJ,Rj ~,JII-:.CJI REGIONAL OFFICE for THE
WORLD HEALTH ~l.Il~I~1 ORGANISATION MONDIALE ORGANIZATION DE LA SANTE ~,JII /'1 'IJ,rJ ~,JII-:.CJI REGIONAL OFFICE FOR THE . BUREAU REGIONAL DE LA EASTERN MEDITBRRANEAN MEDITERRANEE ORIENTALE REGIONAL CCMVIITrEE FOR THE EM/RC14/Tech.Disc./3 EASTERN MEDITERRANEAN 25 August 1964 Fourteenth Session Agenda item 12 TECHNICAL DISCUSSIONS INFANTILE DIARRHOEA CONTRIBUTIONS FROM VARIOUS EXPERTS IN THE EASTERN MEDITERRANEAN REGION (In original language o~ presentation) EM/RC14/Tech.Disc./3 TABLE OF CONTENTS INFANTILE DIARRHOEA IN EGYPl', UAR, by A. Shafik Abbasy, M.D. 1 I Assessment of the Magnitude of Diarrhoeal Disease 1 II Study of Factors Influencing Morbidity and Mortality 3 III Etiological Studies 7 IV Conclusion 13 V Recommendations 13 References 17 INFANTILE DIARRHOEA IN EGYPl', UAR, by Dr. Girgis Abd-EI-Messih 21 I Introduction 21 II Statistical Data in Egypt 22 III Socio-Economic and Environmental Sanitary Factors in Relation to Infantile Diarrhoea 23 IV Comparison between Rates in Egypt and in some other Countries 24 V The Problem of Infantile Diarrhoea in Egypt 25 References 27 Tables 1 to 8 28 MANAGEMENT OF THE DIARRHOEAL DISEASES IN IRAN, by Dr. Hassan Ahari 35 References 42 INFAl·lrILE DIARRHOEA - Summary of Routine Care and Conclusions 43 observed at the Paediatric Ward, Pahlavi University Hospital, Teheran, by Mohammad Gharib, M.D. THE PROBLEM OF INFANTILE DIARRHOEA IN PAKISTAN, by Dr. Hamid Ali Khan 47 I Case History 48 II Degree of Dehydration 49 III Laboratory Investigation 50 IV Principles of Treatment followed 51 V Results and Analysis 53 VI Treatment and Results 56 VII Further Plans for the Study 57 L 'ETAT ACTUEL DES DIARRHEES INFANTlIES EN IRAN, par le Dr. -

Burden of Disease: What Is It and Why Is It Important for Safer Food?
Burden of disease: what is it and why is it important for safer food? What is ‘burden of disease’? Burden of disease is concept that was developed in the 1990s by the Harvard School of Public Health, the World Bank and the World Health Organization (WHO) to describe death and loss of health due to diseases, injuries and risk factors for all regions of the world.1 The burden of a particular disease or condition is estimated by adding together: • the number of years of life a person loses as a consequence of dying early because of the disease (called YLL, or Years of Life Lost); and • the number of years of life a person lives with disability caused by the disease (called YLD, or Years of Life lived with Disability). Adding together the Years of Life Lost and Years of Life lived with Disability gives a single-figure estimate of disease burden, called the Disability Adjusted Life Year (or DALY). One DALY represents the loss of one year of life lived in full health (see text box for more explanation and examples). Looking at burden of disease using DALYs can reveal surprises about a population’s health. For example, the Global Burden of Disease 2004 Update suggests that neuropsychiatric conditions are the most important causes of disability in all regions of the world, accounting for around 33% of all years lived with disability among adults aged 15 years and over, but only 2.2% of deaths.2 Therefore while psychiatric disorders are not traditionally regarded as having a major impact on the health of populations, this picture is completely altered when the burden of disease is estimated using DALYs. -

Diabetic Foot and Gangrene
11 Diabetic Foot and Gangrene Jude Rodrigues and Nivedita Mitta Department of Surgery, Goa Medical College, India 1. Introduction “Early intervention in order to prevent potential disaster in the management of Diabetic foot is not only a great responsibility, but also a great opportunity” Despite advances in our understanding and treatment of diabetes mellitus, diabetic foot disease still remains a terrifying problem. Diabetes is recognized as the most common cause of non-traumatic lower limb amputation in the western world, with individuals over 20 times more likely to undergo an amputation compared to the rest of the population. There is growing evidence that the vascular contribution to diabetic foot disease is greater than was previously realised. This is important because, unlike peripheral neuropathy, Peripheral Arterial Occlusive Disease (PAOD) due to atherosclerosis, is generally far more amenable to therapeutic intervention. PAOD, has been demonstrated to be a greater risk factor than neuropathy in both foot ulceration and lower limb amputation in patients with diabetes. Diabetes is associated with macrovascular and microvascular disease. The term peripheral vascular disease may be more appropriate when referring to lower limb tissue perfusion in diabetes, as this encompasses the influence of both microvascular dysfunction and PAOD. Richards-George P. in his paper about vasculopathy on Jamaican diabetic clinic attendees showed that Doppler measurements of ankle/brachial pressure index (A/BI) revealed that 23% of the diabetics had peripheral occlusive arterial disease (POAD) which was mostly asymptomatic. This underscores the need for regular Doppler A/BI testing in order to improve the recognition, and treatment of POAD. -

Clinical Biliary Tract and Pancreatic Disease
Clinical Upper Gastrointestinal Disorders in Urgent Care, Part 2: Biliary Tract and Pancreatic Disease Urgent message: Upper abdominal pain is a common presentation in urgent care practice. Narrowing the differential diagnosis is sometimes difficult. Understanding the pathophysiology of each disease is the key to making the correct diagnosis and providing the proper treatment. TRACEY Q. DAVIDOFF, MD art 1 of this series focused on disorders of the stom- Pach—gastritis and peptic ulcer disease—on the left side of the upper abdomen. This article focuses on the right side and center of the upper abdomen: biliary tract dis- ease and pancreatitis (Figure 1). Because these diseases are regularly encountered in the urgent care center, the urgent care provider must have a thorough understand- ing of them. Biliary Tract Disease The gallbladder’s main function is to concentrate bile by the absorption of water and sodium. Fasting retains and concentrates bile, and it is secreted into the duodenum by eating. Impaired gallbladder contraction is seen in pregnancy, obesity, rapid weight loss, diabetes mellitus, and patients receiving total parenteral nutrition (TPN). About 10% to 15% of residents of developed nations will form gallstones in their lifetime.1 In the United States, approximately 6% of men and 9% of women 2 have gallstones. Stones form when there is an imbal- ©Phototake.com ance in the chemical constituents of bile, resulting in precipitation of one or more of the components. It is unclear why this occurs in some patients and not others, Tracey Q. Davidoff, MD, is an urgent care physician at Accelcare Medical Urgent Care in Rochester, New York, is on the Board of Directors of the although risk factors do exist.