Associated Ulcerative Colitis, Sclerosing Cholangitis, and Insulin*Dependent Diabetes Mellitus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
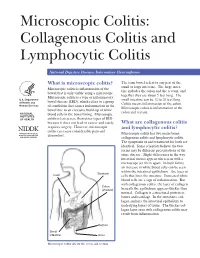
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -

Clinical and Pathological Aspects of Inflammatory Bowel Disease
Inflammatory Bowel Diseases: B.R. Bistrian; J.A. Walker-Smith (eds), Nestlé Nutrition Workshop Series Clinical & Performance Programme, Vol. 2, pp. 83–92, Nestec Ltd.; Vevey/S. Karger AG, Basel, © 1999. Clinical and Pathological Aspects of Inflammatory Bowel Disease Ph. Marteau Gastroenterology Department, European Hospital Georges Pompidou, Paris, France The term “inflammatory bowel disease” applies to bowel diseases of unknown etiology characterized by chronic and often relapsing inflammation. They include ulcerative colitis, Crohn’s disease, indeterminate colitis, pouchitis, and micro- scopic colitides. Although these diseases share a number of epidemiological, pathological, and clinical features, they differ sufficiently to be classified as dis- tinct entities. The term “indeterminate colitis” is used for colitides which do not present enough criteria to be classified as ulcerative colitis or Crohn’s disease. Ulcerative Colitis Pathology Ulcerative colitis is a mucosal disease, which always affects the rectum and often also involves a variable contiguous proximal segment of colonic mucosa [1]. The lesions are continuous, and their upper limit is sharply demarcated from the normal mucosa above. They are limited to the rectum in about 25% of the patients (proctitis); reach the sigmoid colon in another 25% (proctosigmoiditis); spread to the splenic flexure in another 25% (left-sided colitis), and affect the whole colon in about 15% (pancolitis). The small intestine is usually normal but may be occasionally involved by superficial inflammation (“backwash ileitis”) in some patients with pancolitis. Macroscopic lesions can be evaluated during endoscopic examination [2]. Active lesions consist of edema, erythema, lack of the normal vascular pattern, bleeding, exudation of mucus or pus, and ulceration (Table 1). -
Microscopic Colitis
From Department of Medicine, Solna Karolinska Institutet, Stockholm, Sweden MICROSCOPIC COLITIS Marie-Rose Mellander Stockholm 2017 All previously published papers were reproduced with permission from the publisher. Published by Karolinska Institutet. Printed by Eprint AB 2017 © Marie-Rose Mellander, 2017 ISBN 978-91-7676-586-9 Microscopic colitis THESIS FOR DOCTORAL DEGREE (Ph.D.) By Marie-Rose Mellander Principal Supervisor: Opponent: Rolf Hultcrantz Marie Carlson Karolinska Institutet Uppsala University Department of Medicine, Huddinge Department of Medical Sciences; Gastroenterology/Hepatology Co-supervisors: Jan Björk Examination Board: Karolinska Institutet Catarina Almqvist Malmros Department of Medicine, Solna Karolinska Institutet Department of Medical Epidemiology and Robert Löfberg Biostatistics Karolinska Institutet Department of Medicine, Solna Kjell-Arne Ung University of Gothenburg Anders Ekbom Department of Medicine, Sahlgrenska Karolinska Institutet Department of Medicine, Solna Anders Höög Karolinska Institutet Department of Oncology-Pathology To my daughters Julia, Tilda and Sara ABSTRACT Microscopic colitis (MC) is an inflammatory bowel disease (IBD) and a common cause of chronic non-bloody diarrhoea, especially in elderly women. There are two main subtypes, lymphocytic colitis (LC) and collagenous colitis (CC) which are clinically indistinguishable and can be separated only by their characteristic histopathological features. The colonoscopy is usually macroscopically normal although subtle mucosal changes have been reported. The aetiology of MC is unknown and the genetic factors are poorly investigated. This thesis aims to describe MC in a large urban cohort and compare LC and CC regarding clinical and endoscopic features, both at diagnosis and at follow-up (F-U), and to observe the occurrence of coeliac disease, ulcerative colitis (UC) and Crohn’s disease (CD). -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
A SPECIAL ARTICLE Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis Brennan A. Scott Thomas P. Prindiville Collagenous colitis and lymphocytic colitis are chronic relapsing diarrheal illnesses, which are often referred to together as microscopic colitis. It most commonly occurs in women in their fifth to sixth decade. The symptoms usually include profuse watery diarrhea and crampy abdominal pain. Laboratory and endoscopic studies are gener- ally normal but microscopic inflammation is seen when colonic biopsies are performed. In collagenous colitis there is a subepithelial collagen band in addition to chronic inflammation in the lamina propria. The etiology is not known but multiple theories exist including autoimmune, infectious, and medication-induced. Although the course is generally benign, patients may have multiple relapses over many years. Treatment regimens vary and have included anti-diarrheals, antibiotics, 5-aminosalicylates, steroids, and immunosuppressive agents. INTRODUCTION abdominal pain. Both conditions have normal mucosa ollagenous colitis (CC) (Figure 1) and lympho- when viewed endoscopically, however biopsy speci- cytic colitis (LC) (Figure 2) are uncommon mens show chronic mucosal inflammation. In CC C chronic relapsing diarrheal illnesses. The major- there is a subepithelial collagen band of varying thick- ity of patients are women in their fifth to sixth decade ness in association with an inflammatory cell infiltrate who complain of profuse, watery diarrhea, and crampy in the lamina propria (1). The collagen band is absent in LC (2,3). The term microscopic colitis (MC) was Brennan A. Scott, MD, Clinical Fellow, Division of Gas- originally used to describe patients with chronic diar- troenterology, University of California, Davis Medical rhea and normal endoscopic and barium enema stud- Center. -
Microscopic Colitis Collagenous and Lymphocytic Colitis Publisher
The informed patient Microscopic colitis Collagenous and lymphocytic colitis Publisher © 2020 Dr. Falk Pharma GmbH 6th updated and All rights reserved. revised edition 2020 The informed patient Microscopic colitis Collagenous and lymphocytic colitis Prof. Dr. Andreas Tromm, Hattingen (Germany) Microscopic colitis – Collagenous and lymphocytic colitis Address of the author Prof. Dr. Andreas Tromm Klinik für Innere Medizin Augusta-Kranken-Anstalt gGmbH Betriebsstelle EVK Hattingen Akademisches Lehrkrankenhaus der Universität Duisburg-Essen Bredenscheider Str. 54 45525 Hattingen Germany www.klinik-gastroenterologie.de Contents Introduction 4 Clinical presentation 6 Causes and development of microscopic colitis 9 Diagnosis 11 Treatment 14 Frequently asked questions about microscopic colitis 17 3 Microscopic colitis – Collagenous and lymphocytic colitis Introduction The term microscopic colitis encompasses two different disorders of the colon known as collagenous colitis and lymphocytic colitis. Both disorders are characterized by non-bloody watery diarrhea and are sometimes referred to as watery diar- rhea syndromes (Fig. 1). Microscopic colitis Collagenous colitis Lymphocytic colitis Watery diarrhea syndrome Fig. 1: Definition of microscopic colitis. 4 Introduction The term microscopic colitis describes a chronic in- flammatory disease of the colon (“colitis” comes from the Latin term “colon” and the ending “-itis”, which is used in medicine to refer to inflammation) that a doctor cannot identify by colonoscopy with the naked eye because the mucosa of the colon appears normal. In order for the disease to be diagnosed, the doctor must therefore remove a small tissue sample and examine it under a microscope. This is the only way to diagnose microscopic colitis. For collagenous colitis, a thickened collagen layer becomes visible when the tissue samples are stained using special methods, whereas lymphocytic colitis is detected as an increased number of a specific type of white blood cells called lymphocytes (see page 12). -

Microscopic Colitis What Is Microscopic Colitis?
Microscopic Colitis What is microscopic colitis? Microscopic colitis is an inflammation of the colon that a health care provider can see only with a microscope. Inflammation is the body’s normal response to injury, irritation, or infection of tissues. Microscopic colitis is a type of inflammatory bowel disease—the general name for diseases that cause irritation and inflammation in the intestines. The two types of microscopic colitis are collagenous colitis and lymphocytic colitis. Health care providers often use the term microscopic colitis to describe both types because their symptoms and treatments are the same. Some scientists believe that collagenous colitis and lymphocytic colitis may be different phases of the same condition rather than separate conditions. In both types of microscopic colitis, an increase in the number of lymphocytes, a type of white blood cell, can be seen in the epithelium—the layer of cells that lines the colon. An increase in the number of white blood cells is a sign of inflammation. The two types of colitis affect the colon tissue in slightly different ways: Lymphocytic colitis. The number of lymphocytes is higher, and the tissues and lining of the colon are of normal thickness. Collagenous colitis. The layer of collagen, a threadlike protein, underneath the epithelium builds up and becomes thicker than normal. When looking through a microscope, the health care provider may find variations in lymphocyte numbers and collagen thickness in different parts of the colon. These variations may indicate an overlap of the two types of microscopic colitis. What causes microscopic colitis? The exact cause of microscopic colitis is unknown. -
Microscopic Colitis (PDF)
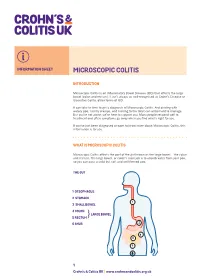
INFORMATION SHEET MICROSCOPIC COLITIS INTRODUCTION Microscopic Colitis is an Inflammatory Bowel Disease (IBD) that affects the large bowel (colon and rectum). It isn’t always as well-recognised as Crohn’s Disease or Ulcerative Colitis, other forms of IBD. It can take to time to get a diagnosis of Microscopic Colitis. And dealing with watery poo, tummy cramps, and rushing to the toilet can all be hard to manage. But you’re not alone; we’re here to support you. Many people respond well to treatment and often symptoms go away when you find what’s right for you. If you’ve just been diagnosed or want to know more about Microscopic Colitis, this information is for you. WHAT IS MICROSCOPIC COLITIS Microscopic Colitis affects the part of the gut known as the large bowel – the colon and rectum. The large bowel, or colon’s main job is to absorb water from your poo, so you can pass a solid but soft and well-formed poo. THE GUT 1 OESOPHAGUS 2 STOMACH 1 3 SMALL BOWEL 2 4 COLON LARGE BOWEL 5 RECTUM} 6 ANUS 2 4 3 5 6 1 Crohn’s & Colitis UK | www.crohnsandcolitis.org.uk MICROSCOPIC COLITIS The walls of your bowel have layers. In Microscopic Colitis the inner lining becomes inflamed. But this change can only be seen when a sample of tissue (biopsy) is taken from your colon and looked at under a microscope. BOWEL LAYERS INNER LINING MIDDLE LAYER OUTER LAYER There are two types of Microscopic Colitis: • Lymphocytic Colitis (LC) – where the inner lining has more white blood cells (lymphocytes) than usual. -

European Consensus on the Histopathology of Inflammatory Bowel Disease☆ F
Journal of Crohn's and Colitis (2013) 7, 827–851 Available online at www.sciencedirect.com ScienceDirect CONSENSUS/GUIDELINES European consensus on the histopathology of inflammatory bowel disease☆ F. Magro a,⁎,1, C. Langner b,1, A. Driessen c, A. Ensari d, K. Geboes e, G.J. Mantzaris f, V. Villanacci g, G. Becheanu h, P. Borralho Nunes i, G. Cathomas j, W. Fries k, A. Jouret-Mourin l, C. Mescoli m, G. de Petris n, C.A. Rubio o, N.A. Shepherd p, M. Vieth q, R. Eliakim r on behalf of the European Society of Pathology (ESP) and the European Crohn's and Colitis Organisation (ECCO)2 a Department of Pharmacology & Therapeutics, Institute for Molecular and Cell Biology, Faculty of Medicine University of Porto, Department of Gastroenterology, Hospital de Sao Joao, Porto, Portugal b Institute of Pathology, Medical University of Graz, Austria c Department of Pathology, University Hospital Antwerp, Belgium d Department of Pathology, Ankara University Medical School, Turkey e Department of Pathology, UZ Leuven, Belgium f 1st Department of Gastroenterology, Evangelismos Hospital, Athens, Greece g Pathology, Spedali Civili, Brescia, Italy h Carol Davila University of Medicine and Pharmacy, Department of Pathology, Bucharest, Romania i Instituto de Anatomia Patologica, Escola Superior de Tecnologia da Saúde de Lisboa & Faculdade de Medicina da Universidade de Lisboa, Portugal j Institute for Pathology, Kanonsspital Baselland, Liestal, Switzerland k Dept. of Clinical and Experimental Medicine, Clinical Unit for Chronic Bowel Disorders, University of -

Collagenous Gastritis: a Morphologic and Immunohistochemical Study of 40 Patients
Modern Pathology (2015) 28, 533–544 & 2015 USCAP, Inc. All rights reserved 0893-3952/15 $32.00 533 Collagenous gastritis: a morphologic and immunohistochemical study of 40 patients Thomas Arnason1,2,10,, Ian S Brown3,4,10, Jeffrey D Goldsmith5, William Anderson6, Blake H O’Brien7, Claire Wilson8, Harland Winter9 and Gregory Y Lauwers1 1Gastrointestinal Pathology Service, Department of Pathology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA; 2Division of Anatomical Pathology, Queen Elizabeth II Health Sciences Centre, Dalhousie University, Halifax, NS, Canada; 3Royal Brisbane and Women’s Hospital, Brisbane, QLD, Australia; 4Envoi Pathology, Brisbane, QLD, Australia; 5Department of Pathology, Children’s Hospital Boston, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA; 6GastroEnterology Associates of Ocala, Ocala, FL, USA; 7Sullivan Nicolaides Pathology, Brisbane, QLD, Australia; 8Providence Alaska Medical Center, Anchorage, AK, USA and 9Department of Pediatrics, Massachusetts General Hospital, Boston, MA, USA Collagenous gastritis is a rare condition defined histologically by a superficial subepithelial collagen layer. This study further characterizes the morphologic spectrum of collagenous gastritis by evaluating a multi- institutional series of 40 patients (26 female and 14 male). The median age at onset was 16 years (range 3–89 years), including 24 patients (60%) under age 18. Twelve patients (30%) had associated celiac disease, collagenous sprue, or collagenous colitis. Hematoxylin and eosin slides were reviewed in biopsies from all patients and tenascin, gastrin, eotaxin, and IgG4/IgG immunohistochemical stains were applied to a subset. The distribution of subepithelial collagen favored the body/fundus in pediatric patients and the antrum in adults. There were increased surface intraepithelial lymphocytes (425 lymphocytes/100 epithelial cells) in five patients. -

Microscopic Colitis—Microbiome, Barrier Function and Associated Diseases
Review Article Page 1 of 10 Microscopic colitis—microbiome, barrier function and associated diseases Saskia van Hemert1, Karolina Skonieczna-Żydecka2, Igor Loniewski2,3, Piotr Szredzki4, Wojciech Marlicz5 1Winclove Probiotics, Amsterdam, the Netherlands; 2Department of Biochemistry and Human Nutrition, Pomeranian Medical University, Szczecin, Poland; 3Sanprobi Sp. z o.o. Sp. K., Szczecin, Poland; 4Endoscopy Unit, Department of Surgery, Hospital Sędziszów Małopolski, Sędziszów Małopolski, Poland; 5Department of Gastroenterology, Pomeranian Medical University, Szczecin, Poland Contributions: (I) Conception and design: S van Hemert, W Marlicz; (II) Administrative support: None; (III) Provision of study materials or patients: K Żydecka-Skonieczna, I Loniewski; (IV) Collection and assembly of data: S van Hemert, K Żydecka-Skonieczna, W Marlicz; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Wojciech Marlicz, MD, PhD, FACG. Department of Gastroenterology, Pomeranian Medical University, Unii Lubelskiej 1, 71-252 Szczecin, Poland. Email: [email protected]. Abstract: Microscopic colitis (MC) is a chronic inflammatory bowel disease (IBD) with little in terms of endoscopic abnormalities and is frequently associated with other autoimmune diseases. The peak incidence of the disease is in middle aged or older populations, mostly females. The pathogenesis of MC is complex, multifactorial and poorly understood. Current concepts revolve around innate immunity or microbiome alterations as well as gut barrier dysfunction, all of which lead to the development of subtle inflammatory lesions in gut mucosa. The results of numerous basic and clinical studies involving molecular techniques as well as advanced endoscopic imaging revealed the important role of both intrinsic (e.g., hormonal) as well as extrinsic (e.g., NSAIDs and PPIs) factors in the modulation of gastrointestinal microbiome and MC pathogenesis. -

Undiagnosed Microscopic Colitis: a Hidden Cause of Chronic Diarrhoea and a Frequently Missed Treatment Opportunity
EDUCATION Frontline Gastroenterol: first published as 10.1136/flgastro-2019-101227 on 5 July 2019. Downloaded from REVIEW Undiagnosed microscopic colitis: a hidden cause of chronic diarrhoea and a frequently missed treatment opportunity Andreas Münch ,1 David S Sanders,2 Michael Molloy- Bland,3 A Pali S Hungin4 1Division of Gastroenterology ABSTRACT patients and clinicians. In many national and Hepatology, Department Microscopic colitis (MC) is a treatable cause of Clinical and Experimental settings, because of downward pressure Medicine, Faculty of Health of chronic, non-bloody , watery diarrhoea, but to minimise specialist referrals and colo- Science, Linköping University, physicians (particularly in primary care) are less noscopies with histology in patients with Linköping, Sweden familiar with MC than with other causes of 2Department of seemingly normal endoscopic appear- Gastroenterology, Royal chronic diarrhoea. The colon in patients with ances, the systems for diagnosing and Hallamshire Hospital, Sheffield, MC is usually macroscopically normal. MC can managing patients with gastrointestinal UK only be diagnosed by histological examination 3Oxford PharmaGenesis, problems work against a diagnosis of MC Melbourne, Victoria, Australia of colonic biopsies (subepithelial collagen band and its effective management. 4 The Institute of Health and >10 µm (collagenous colitis) or >20 intraepithelial When first described in 1980, MC was Society, Faculty of Medical lymphocytes per 100 epithelial cells (lymphocytic 1 Sciences, Newcastle University, thought to be a rare condition. We now Newcastle upon Tyne, UK colitis), both with lamina propria inflammation). know that MC is a common form of inflam- The UK National Health Service exerts downward matory bowel disease (IBD), with one Correspondence to pressure to minimise colonoscopy referrals. -

Collagenous Colitis
Collagenous colitis Author: Doctor Fernando Fernández-Bañares1, Creation Date: July 2003 Update: February 2005 Scientific editor: Professor Jean-Alain Chayvialle 1Department of Gastroenterology, Hospital Universitari Mutua Terrassa, Plaza Dr Robert nº 5, 08221 Terrassa (Barcelona), Spain. [email protected] Abstract Key-words Disease name and synonyms Diagnosis criteria/definition Differential diagnosis Incidence Clinical description Management including treatment Etiology Diagnostic methods Unresolved questions References Abstract Collagenous colitis is characterized by chronic watery diarrhea, normal radiological and endoscopic appearances, and microscopic abnormalities in the colon. The specific histopathological feature is the presence of a subepithelial collagen band (10 µm or more) adjacent to the basal membrane, together with epithelial lymphocyte infiltration and chronic inflammation in lamina propria. A mean annual incidence of 0.6 to 6.1 per 100,000 inhabitants has been described, with a peak incidence in older women. The overall prognosis of the disease is good because cases with life-threatening diarrhea are extremely rare, and diarrhea subsides in almost all patients either spontaneously (near 20%) or with adequate therapy. Recent randomised placebo-controlled trials suggest that budesonide is an effective treatment for collagenous colitis inducing short-term clinical response in 57 to 87% of patients. However, relapse usually occurs early after stopping the drug, and thus maintenance therapy with low doses of budesonide is often required. Uncontrolled studies suggest that either mesalazine, cholestyramine, or bismuth subsalicylate are also effective. The etiology and pathogenesis of collagenous colitis are unknown. A mechanism based on genetic-predisposition, with some features of autoimmunity, initiated by a noxious agent(s) in the fecal stream, which would induce dysfunction of signal transmission between surface epithelium and subepithelial myofibroblasts generating abnormalities in collagen synthesis and/or degradation has been evoked.