Microscopic Cholitis, an Increasingly Frequent Diagnosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Upregulation of Peroxisome Proliferator-Activated Receptor-Α And
Upregulation of peroxisome proliferator-activated receptor-α and the lipid metabolism pathway promotes carcinogenesis of ampullary cancer Chih-Yang Wang, Ying-Jui Chao, Yi-Ling Chen, Tzu-Wen Wang, Nam Nhut Phan, Hui-Ping Hsu, Yan-Shen Shan, Ming-Derg Lai 1 Supplementary Table 1. Demographics and clinical outcomes of five patients with ampullary cancer Time of Tumor Time to Age Differentia survival/ Sex Staging size Morphology Recurrence recurrence Condition (years) tion expired (cm) (months) (months) T2N0, 51 F 211 Polypoid Unknown No -- Survived 193 stage Ib T2N0, 2.41.5 58 F Mixed Good Yes 14 Expired 17 stage Ib 0.6 T3N0, 4.53.5 68 M Polypoid Good No -- Survived 162 stage IIA 1.2 T3N0, 66 M 110.8 Ulcerative Good Yes 64 Expired 227 stage IIA T3N0, 60 M 21.81 Mixed Moderate Yes 5.6 Expired 16.7 stage IIA 2 Supplementary Table 2. Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis of an ampullary cancer microarray using the Database for Annotation, Visualization and Integrated Discovery (DAVID). This table contains only pathways with p values that ranged 0.0001~0.05. KEGG Pathway p value Genes Pentose and 1.50E-04 UGT1A6, CRYL1, UGT1A8, AKR1B1, UGT2B11, UGT2A3, glucuronate UGT2B10, UGT2B7, XYLB interconversions Drug metabolism 1.63E-04 CYP3A4, XDH, UGT1A6, CYP3A5, CES2, CYP3A7, UGT1A8, NAT2, UGT2B11, DPYD, UGT2A3, UGT2B10, UGT2B7 Maturity-onset 2.43E-04 HNF1A, HNF4A, SLC2A2, PKLR, NEUROD1, HNF4G, diabetes of the PDX1, NR5A2, NKX2-2 young Starch and sucrose 6.03E-04 GBA3, UGT1A6, G6PC, UGT1A8, ENPP3, MGAM, SI, metabolism -

(12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 De Juan Et Al
US 200601 10428A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 de Juan et al. (43) Pub. Date: May 25, 2006 (54) METHODS AND DEVICES FOR THE Publication Classification TREATMENT OF OCULAR CONDITIONS (51) Int. Cl. (76) Inventors: Eugene de Juan, LaCanada, CA (US); A6F 2/00 (2006.01) Signe E. Varner, Los Angeles, CA (52) U.S. Cl. .............................................................. 424/427 (US); Laurie R. Lawin, New Brighton, MN (US) (57) ABSTRACT Correspondence Address: Featured is a method for instilling one or more bioactive SCOTT PRIBNOW agents into ocular tissue within an eye of a patient for the Kagan Binder, PLLC treatment of an ocular condition, the method comprising Suite 200 concurrently using at least two of the following bioactive 221 Main Street North agent delivery methods (A)-(C): Stillwater, MN 55082 (US) (A) implanting a Sustained release delivery device com (21) Appl. No.: 11/175,850 prising one or more bioactive agents in a posterior region of the eye so that it delivers the one or more (22) Filed: Jul. 5, 2005 bioactive agents into the vitreous humor of the eye; (B) instilling (e.g., injecting or implanting) one or more Related U.S. Application Data bioactive agents Subretinally; and (60) Provisional application No. 60/585,236, filed on Jul. (C) instilling (e.g., injecting or delivering by ocular ion 2, 2004. Provisional application No. 60/669,701, filed tophoresis) one or more bioactive agents into the Vit on Apr. 8, 2005. reous humor of the eye. Patent Application Publication May 25, 2006 Sheet 1 of 22 US 2006/0110428A1 R 2 2 C.6 Fig. -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
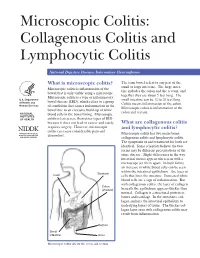
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -

Identification of Potentially Inappropriate Medications with Risk
Journal name: Clinical Interventions in Aging Article Designation: Original Research Year: 2019 Volume: 14 Clinical Interventions in Aging Dovepress Running head verso: Aguiar et al Running head recto: Aguiar et al open access to scientific and medical research DOI: 192252 Open Access Full Text Article ORIGINAL RESEARCH Identification of potentially inappropriate medications with risk of major adverse cardiac and cerebrovascular events among elderly patients in ambulatory setting and long-term care facilities This article was published in the following Dove Medical Press journal: Clinical Interventions in Aging João Pedro Aguiar1 Purpose: Cardiovascular diseases (CVDs) are extremely common among the elderly, but Luís Heitor Costa2 information on the use of potentially inappropriate medications (PIMs) with cardiovascular Filipa Alves da Costa3,4 risk is scarce. We aimed to determine the prevalence of PIMs with risk of cardiac and cere- Hubert GM Leufkens5 brovascular adverse events (CCVAEs), including major adverse cardiac and cerebrovascular Ana Paula Martins1 events (MACCE). Patients and methods: A cross-sectional study was performed using a convenience sample 1Research Institute for Medicines (iMED.ULisboa), Faculdade de from four long-term care facilities and one community pharmacy in Portugal. Patients were For personal use only. Farmácia, Universidade de Lisboa, included if they were aged 65 or older and presented at least one type of medication in their 2 Lisboa, Portugal; Serviço de medical and pharmacotherapeutic records from 2015 until December 2017. The main outcome Medicina Interna, Centro Hospitalar Psiquiátrico de Lisboa (CHPL), Lisboa, was defined as the presence of PIMs with risk of MACCE and was assessed by applying a Portugal; 3Centro de Investigação PIM-MACCE list that was developed from a previous study. -

Associated Ulcerative Colitis, Sclerosing Cholangitis, and Insulin*Dependent Diabetes Mellitus
CASE REPORT Associated ulcerative colitis, sclerosing cholangitis, and insulin*dependent diabetes mellitus MARSHA KAY, MD; ROBERT WYLLIE, MD; WILLIAM MICHENER, MD; MAUREEN CAULFIELD, MD; RITA STEFFEN, MD LINICALLY symptomatic We report two young men with clinical and laboratory evidence ulcerative colitis, sclero- of macroscopic ulcerative colitis, sclerosing cholangitis, and insu- sing cholangitis, and in- lin-dependent diabetes mellitus. The first patient presented at age Csulin-dependent diabe- 15 with vomiting, abdominal pain, weight loss, and abnormal tes mellitus have not previously liver function test results. Liver biopsy and endoscopic retrograde been reported in the same patient. cholangiopancreatography (ERCP) demonstrated sclerosing cho- Although each may be associated langitis. Colonoscopy with biopsy revealed ulcerative colitis with the other, their occurrence in which responded to sulfasalazine. Diabetes occurred at age 18 and the same individual implies a com- insulin therapy was begun. mon susceptibility, perhaps involv- The second patient was 19 at presentation with diarrhea, hema- ing the immune system. We have tochezia, and weight loss. Proctosigmoidoscopy revealed identified two patients with each ulcerative colitis, and sulfasalazine led to clinical remission. Three of these disorders. These two months later he developed diabetes requiring insulin therapy. At young men were followed up at age 28, he developed elevated alkaline phosphatase, and ERCP re- The Cleveland Clinic Foundation vealed sclerosing cholangitis. At age 37 he expired from adenocar- between 1970 and 1992. cinoma that metastasized to the liver. Literature review revealed only one possible case report of this PATIENT I; CASE HISTORY association with microscopic asymptomatic ulcerative colitis in that patient. Statistical analysis suggests that this association is Patient 1 presented at age 15 real rather than a chance occurrence. -

Pharmaceutical Appendix to the Tariff Schedule 2
Harmonized Tariff Schedule of the United States (2007) (Rev. 2) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2007) (Rev. 2) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. ABACAVIR 136470-78-5 ACIDUM LIDADRONICUM 63132-38-7 ABAFUNGIN 129639-79-8 ACIDUM SALCAPROZICUM 183990-46-7 ABAMECTIN 65195-55-3 ACIDUM SALCLOBUZICUM 387825-03-8 ABANOQUIL 90402-40-7 ACIFRAN 72420-38-3 ABAPERIDONUM 183849-43-6 ACIPIMOX 51037-30-0 ABARELIX 183552-38-7 ACITAZANOLAST 114607-46-4 ABATACEPTUM 332348-12-6 ACITEMATE 101197-99-3 ABCIXIMAB 143653-53-6 ACITRETIN 55079-83-9 ABECARNIL 111841-85-1 ACIVICIN 42228-92-2 ABETIMUSUM 167362-48-3 ACLANTATE 39633-62-0 ABIRATERONE 154229-19-3 ACLARUBICIN 57576-44-0 ABITESARTAN 137882-98-5 ACLATONIUM NAPADISILATE 55077-30-0 ABLUKAST 96566-25-5 ACODAZOLE 79152-85-5 ABRINEURINUM 178535-93-8 ACOLBIFENUM 182167-02-8 ABUNIDAZOLE 91017-58-2 ACONIAZIDE 13410-86-1 ACADESINE 2627-69-2 ACOTIAMIDUM 185106-16-5 ACAMPROSATE 77337-76-9 -

2009 Nhamcs Micro-Data File Documentation Page 1
2009 NHAMCS MICRO-DATA FILE DOCUMENTATION PAGE 1 ABSTRACT This material provides documentation for users of the public use micro-data files of the 2009 National Hospital Ambulatory Medical Care Survey (NHAMCS). NHAMCS is a national probability sample survey of visits to hospital outpatient and emergency departments, conducted by the National Center for Health Statistics, Centers for Disease Control and Prevention. The survey is a component of the National Health Care Surveys, which measure health care utilization across a variety of health care providers. There are two micro-data files produced from NHAMCS, one for outpatient department records and one for emergency department records. Section I of this documentation, “Description of the National Hospital Ambulatory Medical Care Survey,” includes information on the scope of the survey, the sample, field activities, data collection procedures, medical coding procedures, and population estimates. Section II provides detailed descriptions of the contents of each file’s data record by location. Section III contains marginal data for selected items on each file. The appendixes contain sampling errors, instructions and definitions for completing the Patient Record forms, and lists of codes used in the survey. PAGE 2 2009 NHAMCS MICRO-DATA FILE DOCUMENTATION SUMMARY OF CHANGES FOR 2009 The 2009 NHAMCS Emergency Department and Outpatient Department public use micro-data files are, for the most part, similar to the 2008 files, but there are some important changes. These are described in more detail below and reflect changes to the survey instrument, the Patient Record form. Emergency Departments 1. New or Modified Items a. In item 1, Patient Information, there is a new checkbox item “Arrival by Ambulance.” This replaces the 2008 item, “Mode of Arrival.” b. -

Clinical and Pathological Aspects of Inflammatory Bowel Disease
Inflammatory Bowel Diseases: B.R. Bistrian; J.A. Walker-Smith (eds), Nestlé Nutrition Workshop Series Clinical & Performance Programme, Vol. 2, pp. 83–92, Nestec Ltd.; Vevey/S. Karger AG, Basel, © 1999. Clinical and Pathological Aspects of Inflammatory Bowel Disease Ph. Marteau Gastroenterology Department, European Hospital Georges Pompidou, Paris, France The term “inflammatory bowel disease” applies to bowel diseases of unknown etiology characterized by chronic and often relapsing inflammation. They include ulcerative colitis, Crohn’s disease, indeterminate colitis, pouchitis, and micro- scopic colitides. Although these diseases share a number of epidemiological, pathological, and clinical features, they differ sufficiently to be classified as dis- tinct entities. The term “indeterminate colitis” is used for colitides which do not present enough criteria to be classified as ulcerative colitis or Crohn’s disease. Ulcerative Colitis Pathology Ulcerative colitis is a mucosal disease, which always affects the rectum and often also involves a variable contiguous proximal segment of colonic mucosa [1]. The lesions are continuous, and their upper limit is sharply demarcated from the normal mucosa above. They are limited to the rectum in about 25% of the patients (proctitis); reach the sigmoid colon in another 25% (proctosigmoiditis); spread to the splenic flexure in another 25% (left-sided colitis), and affect the whole colon in about 15% (pancolitis). The small intestine is usually normal but may be occasionally involved by superficial inflammation (“backwash ileitis”) in some patients with pancolitis. Macroscopic lesions can be evaluated during endoscopic examination [2]. Active lesions consist of edema, erythema, lack of the normal vascular pattern, bleeding, exudation of mucus or pus, and ulceration (Table 1). -
Microscopic Colitis
From Department of Medicine, Solna Karolinska Institutet, Stockholm, Sweden MICROSCOPIC COLITIS Marie-Rose Mellander Stockholm 2017 All previously published papers were reproduced with permission from the publisher. Published by Karolinska Institutet. Printed by Eprint AB 2017 © Marie-Rose Mellander, 2017 ISBN 978-91-7676-586-9 Microscopic colitis THESIS FOR DOCTORAL DEGREE (Ph.D.) By Marie-Rose Mellander Principal Supervisor: Opponent: Rolf Hultcrantz Marie Carlson Karolinska Institutet Uppsala University Department of Medicine, Huddinge Department of Medical Sciences; Gastroenterology/Hepatology Co-supervisors: Jan Björk Examination Board: Karolinska Institutet Catarina Almqvist Malmros Department of Medicine, Solna Karolinska Institutet Department of Medical Epidemiology and Robert Löfberg Biostatistics Karolinska Institutet Department of Medicine, Solna Kjell-Arne Ung University of Gothenburg Anders Ekbom Department of Medicine, Sahlgrenska Karolinska Institutet Department of Medicine, Solna Anders Höög Karolinska Institutet Department of Oncology-Pathology To my daughters Julia, Tilda and Sara ABSTRACT Microscopic colitis (MC) is an inflammatory bowel disease (IBD) and a common cause of chronic non-bloody diarrhoea, especially in elderly women. There are two main subtypes, lymphocytic colitis (LC) and collagenous colitis (CC) which are clinically indistinguishable and can be separated only by their characteristic histopathological features. The colonoscopy is usually macroscopically normal although subtle mucosal changes have been reported. The aetiology of MC is unknown and the genetic factors are poorly investigated. This thesis aims to describe MC in a large urban cohort and compare LC and CC regarding clinical and endoscopic features, both at diagnosis and at follow-up (F-U), and to observe the occurrence of coeliac disease, ulcerative colitis (UC) and Crohn’s disease (CD). -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
A SPECIAL ARTICLE Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis Brennan A. Scott Thomas P. Prindiville Collagenous colitis and lymphocytic colitis are chronic relapsing diarrheal illnesses, which are often referred to together as microscopic colitis. It most commonly occurs in women in their fifth to sixth decade. The symptoms usually include profuse watery diarrhea and crampy abdominal pain. Laboratory and endoscopic studies are gener- ally normal but microscopic inflammation is seen when colonic biopsies are performed. In collagenous colitis there is a subepithelial collagen band in addition to chronic inflammation in the lamina propria. The etiology is not known but multiple theories exist including autoimmune, infectious, and medication-induced. Although the course is generally benign, patients may have multiple relapses over many years. Treatment regimens vary and have included anti-diarrheals, antibiotics, 5-aminosalicylates, steroids, and immunosuppressive agents. INTRODUCTION abdominal pain. Both conditions have normal mucosa ollagenous colitis (CC) (Figure 1) and lympho- when viewed endoscopically, however biopsy speci- cytic colitis (LC) (Figure 2) are uncommon mens show chronic mucosal inflammation. In CC C chronic relapsing diarrheal illnesses. The major- there is a subepithelial collagen band of varying thick- ity of patients are women in their fifth to sixth decade ness in association with an inflammatory cell infiltrate who complain of profuse, watery diarrhea, and crampy in the lamina propria (1). The collagen band is absent in LC (2,3). The term microscopic colitis (MC) was Brennan A. Scott, MD, Clinical Fellow, Division of Gas- originally used to describe patients with chronic diar- troenterology, University of California, Davis Medical rhea and normal endoscopic and barium enema stud- Center. -
Microscopic Colitis Collagenous and Lymphocytic Colitis Publisher
The informed patient Microscopic colitis Collagenous and lymphocytic colitis Publisher © 2020 Dr. Falk Pharma GmbH 6th updated and All rights reserved. revised edition 2020 The informed patient Microscopic colitis Collagenous and lymphocytic colitis Prof. Dr. Andreas Tromm, Hattingen (Germany) Microscopic colitis – Collagenous and lymphocytic colitis Address of the author Prof. Dr. Andreas Tromm Klinik für Innere Medizin Augusta-Kranken-Anstalt gGmbH Betriebsstelle EVK Hattingen Akademisches Lehrkrankenhaus der Universität Duisburg-Essen Bredenscheider Str. 54 45525 Hattingen Germany www.klinik-gastroenterologie.de Contents Introduction 4 Clinical presentation 6 Causes and development of microscopic colitis 9 Diagnosis 11 Treatment 14 Frequently asked questions about microscopic colitis 17 3 Microscopic colitis – Collagenous and lymphocytic colitis Introduction The term microscopic colitis encompasses two different disorders of the colon known as collagenous colitis and lymphocytic colitis. Both disorders are characterized by non-bloody watery diarrhea and are sometimes referred to as watery diar- rhea syndromes (Fig. 1). Microscopic colitis Collagenous colitis Lymphocytic colitis Watery diarrhea syndrome Fig. 1: Definition of microscopic colitis. 4 Introduction The term microscopic colitis describes a chronic in- flammatory disease of the colon (“colitis” comes from the Latin term “colon” and the ending “-itis”, which is used in medicine to refer to inflammation) that a doctor cannot identify by colonoscopy with the naked eye because the mucosa of the colon appears normal. In order for the disease to be diagnosed, the doctor must therefore remove a small tissue sample and examine it under a microscope. This is the only way to diagnose microscopic colitis. For collagenous colitis, a thickened collagen layer becomes visible when the tissue samples are stained using special methods, whereas lymphocytic colitis is detected as an increased number of a specific type of white blood cells called lymphocytes (see page 12). -

Microscopic Colitis What Is Microscopic Colitis?
Microscopic Colitis What is microscopic colitis? Microscopic colitis is an inflammation of the colon that a health care provider can see only with a microscope. Inflammation is the body’s normal response to injury, irritation, or infection of tissues. Microscopic colitis is a type of inflammatory bowel disease—the general name for diseases that cause irritation and inflammation in the intestines. The two types of microscopic colitis are collagenous colitis and lymphocytic colitis. Health care providers often use the term microscopic colitis to describe both types because their symptoms and treatments are the same. Some scientists believe that collagenous colitis and lymphocytic colitis may be different phases of the same condition rather than separate conditions. In both types of microscopic colitis, an increase in the number of lymphocytes, a type of white blood cell, can be seen in the epithelium—the layer of cells that lines the colon. An increase in the number of white blood cells is a sign of inflammation. The two types of colitis affect the colon tissue in slightly different ways: Lymphocytic colitis. The number of lymphocytes is higher, and the tissues and lining of the colon are of normal thickness. Collagenous colitis. The layer of collagen, a threadlike protein, underneath the epithelium builds up and becomes thicker than normal. When looking through a microscope, the health care provider may find variations in lymphocyte numbers and collagen thickness in different parts of the colon. These variations may indicate an overlap of the two types of microscopic colitis. What causes microscopic colitis? The exact cause of microscopic colitis is unknown.