2009 Nhamcs Micro-Data File Documentation Page 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Upregulation of Peroxisome Proliferator-Activated Receptor-Α And
Upregulation of peroxisome proliferator-activated receptor-α and the lipid metabolism pathway promotes carcinogenesis of ampullary cancer Chih-Yang Wang, Ying-Jui Chao, Yi-Ling Chen, Tzu-Wen Wang, Nam Nhut Phan, Hui-Ping Hsu, Yan-Shen Shan, Ming-Derg Lai 1 Supplementary Table 1. Demographics and clinical outcomes of five patients with ampullary cancer Time of Tumor Time to Age Differentia survival/ Sex Staging size Morphology Recurrence recurrence Condition (years) tion expired (cm) (months) (months) T2N0, 51 F 211 Polypoid Unknown No -- Survived 193 stage Ib T2N0, 2.41.5 58 F Mixed Good Yes 14 Expired 17 stage Ib 0.6 T3N0, 4.53.5 68 M Polypoid Good No -- Survived 162 stage IIA 1.2 T3N0, 66 M 110.8 Ulcerative Good Yes 64 Expired 227 stage IIA T3N0, 60 M 21.81 Mixed Moderate Yes 5.6 Expired 16.7 stage IIA 2 Supplementary Table 2. Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis of an ampullary cancer microarray using the Database for Annotation, Visualization and Integrated Discovery (DAVID). This table contains only pathways with p values that ranged 0.0001~0.05. KEGG Pathway p value Genes Pentose and 1.50E-04 UGT1A6, CRYL1, UGT1A8, AKR1B1, UGT2B11, UGT2A3, glucuronate UGT2B10, UGT2B7, XYLB interconversions Drug metabolism 1.63E-04 CYP3A4, XDH, UGT1A6, CYP3A5, CES2, CYP3A7, UGT1A8, NAT2, UGT2B11, DPYD, UGT2A3, UGT2B10, UGT2B7 Maturity-onset 2.43E-04 HNF1A, HNF4A, SLC2A2, PKLR, NEUROD1, HNF4G, diabetes of the PDX1, NR5A2, NKX2-2 young Starch and sucrose 6.03E-04 GBA3, UGT1A6, G6PC, UGT1A8, ENPP3, MGAM, SI, metabolism -

(12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 De Juan Et Al
US 200601 10428A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 de Juan et al. (43) Pub. Date: May 25, 2006 (54) METHODS AND DEVICES FOR THE Publication Classification TREATMENT OF OCULAR CONDITIONS (51) Int. Cl. (76) Inventors: Eugene de Juan, LaCanada, CA (US); A6F 2/00 (2006.01) Signe E. Varner, Los Angeles, CA (52) U.S. Cl. .............................................................. 424/427 (US); Laurie R. Lawin, New Brighton, MN (US) (57) ABSTRACT Correspondence Address: Featured is a method for instilling one or more bioactive SCOTT PRIBNOW agents into ocular tissue within an eye of a patient for the Kagan Binder, PLLC treatment of an ocular condition, the method comprising Suite 200 concurrently using at least two of the following bioactive 221 Main Street North agent delivery methods (A)-(C): Stillwater, MN 55082 (US) (A) implanting a Sustained release delivery device com (21) Appl. No.: 11/175,850 prising one or more bioactive agents in a posterior region of the eye so that it delivers the one or more (22) Filed: Jul. 5, 2005 bioactive agents into the vitreous humor of the eye; (B) instilling (e.g., injecting or implanting) one or more Related U.S. Application Data bioactive agents Subretinally; and (60) Provisional application No. 60/585,236, filed on Jul. (C) instilling (e.g., injecting or delivering by ocular ion 2, 2004. Provisional application No. 60/669,701, filed tophoresis) one or more bioactive agents into the Vit on Apr. 8, 2005. reous humor of the eye. Patent Application Publication May 25, 2006 Sheet 1 of 22 US 2006/0110428A1 R 2 2 C.6 Fig. -
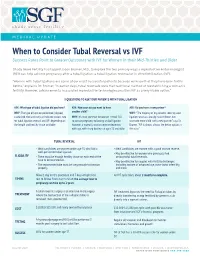
When to Consider Tubal Reversal Vs IVF Success Rates Point to Greater Outcomes with IVF for Women in Their Mid-Thirties and Older
MEDICAL UPDATE When to Consider Tubal Reversal vs IVF Success Rates Point to Greater Outcomes with IVF for Women in their Mid-Thirties and Older Shady Grove Fertility has tapped Jason Bromer, M.D., to explore the two primary ways a reproductive endocrinologist (REI) can help achieve pregnancy after a tubal ligation: a tubal ligation reversal or in vitro fertilization (IVF). "Women with tubal ligations are some of our most successful patients because we know that they have been fertile before," explains Dr. Bromer. "In earlier days, tubal reversals were the traditional method of reestablishing a woman’s fertility. However, advancements in assisted reproductive technologies position IVF as a very viable option." 3 QUESTIONS TO ASK YOUR PATIENTS WITH TUBAL LIGATION ASK: What type of tubal ligation did you have? ASK: How soon do you want to have ASK: Do you have a new partner? WHY: The type of ligation performed (clipped, another child? WHY: "The majority of my patients seeking tubal cauterized, tied and cut) can indicate success rate WHY: It’s most common for women in their 30s ligation reversals already have children, but for tubal ligation reversal and IVF, depending on to pursue pregnancy following a tubal ligation. want one more child with a new partner," says Dr. the length and healthy tissue available. However, a woman’s ovarian reserve decreases Bromer. "IVF is almost always the better option in with age, with sharp declines at ages 35 and older. this case." TUBAL REVERSAL IVF • Ideal candidates are women under age 35 who had a • Ideal candidates are women with a good ovarian reserve. -

Appendix on Tariff Elimination Schedule for Mercosur
Trade part of the EU-Mercosur Association Agreement Without Prejudice Disclaimer: In view of the Commission's transparency policy, the Commission is publishing the texts of the Trade Part of the Agreement following the agreement in principle announced on 28 June 2019. The texts are published for information purposes only and may undergo further modifications including as a result of the process of legal revision. However, in view of the growing public interest in the negotiations, the texts are published at this stage of the negotiations for information purposes. These texts are without prejudice to the final outcome of the agreement between the EU and Mercosur. The texts will be final upon signature. The agreement will become binding on the Parties under international law only after completion by each Party of its internal legal procedures necessary for the entry into force of the Agreement (or its provisional application). AR applied BR applied PY applied UY applied Mercosur Final NCM Description Comments tariff tariff tariff tariff Offer 01012100 Pure-bred horses 0 0 0 0 0 01012900 Lives horses, except pure-bred breeding 2 2 2 2 0 01013000 Asses, pure-bred breeding 4 4 4 4 4 01019000 Asses, except pure-bred breeding 4 4 4 4 4 01022110 Purebred breeding cattle, pregnant or lactating 0 0 0 0 0 01022190 Other pure-bred cattle, for breeding 0 0 0 0 0 01022911 Other bovine animals for breeding,pregnant or lactating 2 2 2 2 0 01022919 Other bovine animals for breeding 2 2 2 2 4 01022990 Other live catlle 2 2 2 2 0 01023110 Pure-bred breeding buffalo, pregnant or lactating 0 0 0 0 0 01023190 Other pure-bred breeding buffalo 0 0 0 0 0 01023911 Other buffalo for breeding, ex. -

New Therapeutic Property of Dimebon As a Neuroprotective Agent
Send Orders for Reprints to [email protected] Current Medicinal Chemistry, 2016, 23, 1-12 1 REVIEW ARTICLE New Therapeutic Property of Dimebon as a Neuroprotective Agent Aleksey Ustyugov1, Elena Shevtsova1, George E. Barreto2,3, Ghulam Md Ashraf 4, Sergey O. Bachurin1 and Gjumrakch Aliev1,5,6,* 1Institute of Physiologically Active Compounds, Russian Academy of Sciences, Severniy Proezd 1, Cher- nogolovka, 142432, Russia; 2Departamento de Nutrición y Bioquímica, Facultad de Ciencias, Pontificia Uni- versidad Javeriana, Bogotá D.C., Colombia; 3Instituto de Ciencias Biomédicas, Universidad Autónoma de Chile, Santiago, Chile; 4King Fahd Medical Research Center, King Abdulaziz University, Jeddah, Saudi Ara- bia; 5GALLY International Biomedical Research Consulting LLC., 7733 Louis Pasteur Drive, #330, San An- tonio, TX, 78229, USA; 6School of Health Science and Healthcare Administration, University of Atlanta, E. Johns Crossing, #175, Johns Creek, GA, 30097, USA Abstract: Dimebon (or Latrepirdine) was initially used as an anti-histamergic drug but later new therapeutic properties were rediscovered, adding to a growing body of “old” agents with prominent neuroprotective effects. In the present manuscript, we are focusing on our latest study on Dimebon with regard to brain’s pathological processes using in vivo protei- A R T I C L E H I S T O R Y nopathy models. In the study, neurodegenerative pathology has been attributed to a group of aggregate-prone proteins: hyperphosphorylated tau, fused in sarcoma and γ-synuclein , which Received: March 13, 2016 Revised: June 08, 2016 are involved in a number of neurological disorders. We have also presented our in vitro Accepted: July 24, 2016 model based on overexpression of an aberrant mutant form of transactive response DNA DOI: 10.2174/0929867323666160804 binding 43 kDa protein in cultured SH-SY5Y neuroblastoma cells. -

List of Union Reference Dates A
Active substance name (INN) EU DLP BfArM / BAH DLP yearly PSUR 6-month-PSUR yearly PSUR bis DLP (List of Union PSUR Submission Reference Dates and Frequency (List of Union Frequency of Reference Dates and submission of Periodic Frequency of submission of Safety Update Reports, Periodic Safety Update 30 Nov. 2012) Reports, 30 Nov. -

Successful Pregnancies After Removal of Intratubal Microinserts
2. Tonni G, De Felice C, Centini G, Ginanneschi C. Cervical and 5. Levine AB, Alvarez M, Wedgwood J, Berkowitz RL, Holzman oral teratoma in the fetus: a systematic review of etiology, I. Contemporary management of a potentially lethal fetal pathology, diagnosis, treatment and prognosis. Arch Gynecol anomaly: a successful perinatal approach to epignathus. Obstet Obstet 2010;282:355–61. Gynecol 1990;76:962–6. 3. Calda P, Novotna M, Cutka D, Brestak M, Haslik L, Goldova 6. Berrington JE, Stafford FW, Macphail S. Emergency EXIT for B, et al. A case of an epignathus with intracranial extension preterm labour after FETO. Arch Dis Child Fetal Neonatal Ed appearing as a persistently open mouth at 16 weeks and 2010;95:F376–7. subsequently diagnosed at 20 weeks of gestation. J Clin Ultra- 7. Hedrick HL, Flake AW, Crombleholme TM, Howell LJ, sound 2011;39:164–8. Johnson MP, Wilson RD, et al. The ex utero intrapartum 4. Marwan A, Crombleholme TM. The EXIT procedure: principles, therapy procedure for high-risk fetal lung lesions. J Pediatr pitfalls, and progress. Semin Pediatr Surg 2006;15:107–15. Surg 2005;40:1038–44. Successful Pregnancies After and who would like to conceive have two options: in vitro fertilization and sterilization reversal. Successful Removal of Intratubal Microinserts pregnancies resulting from in vitro fertilization after intratubal microinsert sterilization have been described.2 Charles W. Monteith, MD, Based on a literature search of the entire PubMed and Gary S. Berger, MD, MPH database up to August 2011 (using the key words “Essure” and “pregnancy”), these are the first two re- BACKGROUND: Patients with intratubal microinsert ports of successful pregnancy after surgical outpatient sterilization later may request reversal. -

Pharmaceutical Manufacturing Formulations Liquid Products V () L UME Sarfaraz K
HANDBOOK OF Pharmaceutical Manufacturing Formulations Liquid Products V () L UME Sarfaraz K. Niazi CRC PRESS Boca Raton London New York Washington, D.C. Table of Contents PART I Regulatory and Manufacturing Guidance 1 Chapter 1 Current Good Manufacturing Practice Considerations in Liquid Manufacturing 3 I. Introduction 3 II. Facilities 3 III. Equipment 3 IV. Raw Materials 4 V. Compounding 4 VI. Microbiological Quality 4 VII. Oral Suspensions 5 VIII. Product Specifications 5 IX. Process Validation 5 X. Stability 5 XI. Packaging 6 Chapter 2 Stability Testing of New Drug Substances and Products 7 I. Introduction 7 II. Drug Substance 7 A. General Case 8 B. Drug Substances Intended for Storage in a Refrigerator 8 C. Drag Substances Intended for Storage in a Freezer 8 D. Drug Substances Intended for Storage below -20°C 9 HI. Drag Product 10 A. General Case •' B. Drag Products Packaged in Impermeable Containers 11 C. Drag Products Packaged in Semipermeable Containers 11 D. Drag Products Intended for Storage in a Refrigerator 12 E. Drag Products Intended for Storage in a Freezer 13 F. Drag Products Intended for Storage below -20"C 13 IV Glossary 14 References 1() Chapter 3 Container Closure Systems '7 I. Introduction '7 A. Definitions '7 B. Current Good Manufacturing Practice, the Consumer Product Safety Commission, and Requirements on Containers and Closures 17 C. Additional Considerations 17 II. Qualification and Quality Control of Packaging Components 18 A. Description 21 B. Information about Suitability 21 C. Stability Data (Packaging Concerns) 22 D. Inhalation Drag Products 23 E. Injection and Ophthalmic Drag Products 23 F. -

Monash Health Referral Guidelines – Gynaecology
Monash Health Referral Guidelines (Incorporating Statewide Referral Criteria) GYNAECOLOGY EXCLUSIONS Services not offered In Vitro Fertilisation by Monash Health CONDITIONS CONTRACEPTIVE COUNSELLING MENSTRUAL MANAGEMENT Contraception Persistent, heavy menstrual bleeding Pregnancy Choices Bartholin's cysts / vaginal lesions Post-Menopausal bleeding Post-Coital bleeding DYSPLASIA Persistent or unexplained intermenstrual Dysplasia/Abnormal Cervical bleeding Screening Test Fibroids Vulval ulcers Vulval disorders PELVIC FLOOR/UROGYNAECOLOGY Genital warts Pelvic organ prolapse Urinary incontinence Recurrent UTI’s GYNAECOLOGY ENDOSCOPY Ovarian and other adnexal pathology Dyspareunia REPRODUCTIVE MEDICINE Pelvic Inflammatory disease Infertility Persistent pelvic pain Amenorrhea Male infertility Recurrent miscarriages GYNAECOLOGY ONCOLOGY Tubal & vasectomy reversal Cancer of the cervix Endocrine problems (Polycystic Ovarian cancer Ovarian Syndrome) Gynae cancers -suspected and confirmed SEXUAL MEDICINE & THERAPY CLINIC Sexual & relationship counselling MENOPAUSE Turner 's Syndrome Cancer and menopause PAEDIATRIC & ADOLESCENT GYNAE Premature menopause Paediatric and Adolescent Gynaecology General menopause ENDOMETRIOSIS Endometriosis Head of unit: Program Director: Last updated: Professor Beverley Vollenhoven Associate Professor Ryan Hodges 06/02/2020 Monash Health Referral Guidelines (Incorporating Statewide Referral Criteria) GYNAECOLOGY PRIORITY For emergency cases please do any of the following: EMERGENCY - send the patient to the Emergency -

)&F1y3x PHARMACEUTICAL APPENDIX to THE
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ACTODIGIN 36983-69-4 ABANOQUIL 90402-40-7 ADAFENOXATE 82168-26-1 ABCIXIMAB 143653-53-6 ADAMEXINE 54785-02-3 ABECARNIL 111841-85-1 ADAPALENE 106685-40-9 ABITESARTAN 137882-98-5 ADAPROLOL 101479-70-3 ABLUKAST 96566-25-5 ADATANSERIN 127266-56-2 ABUNIDAZOLE 91017-58-2 ADEFOVIR 106941-25-7 ACADESINE 2627-69-2 ADELMIDROL 1675-66-7 ACAMPROSATE 77337-76-9 ADEMETIONINE 17176-17-9 ACAPRAZINE 55485-20-6 ADENOSINE PHOSPHATE 61-19-8 ACARBOSE 56180-94-0 ADIBENDAN 100510-33-6 ACEBROCHOL 514-50-1 ADICILLIN 525-94-0 ACEBURIC ACID 26976-72-7 ADIMOLOL 78459-19-5 ACEBUTOLOL 37517-30-9 ADINAZOLAM 37115-32-5 ACECAINIDE 32795-44-1 ADIPHENINE 64-95-9 ACECARBROMAL 77-66-7 ADIPIODONE 606-17-7 ACECLIDINE 827-61-2 ADITEREN 56066-19-4 ACECLOFENAC 89796-99-6 ADITOPRIM 56066-63-8 ACEDAPSONE 77-46-3 ADOSOPINE 88124-26-9 ACEDIASULFONE SODIUM 127-60-6 ADOZELESIN 110314-48-2 ACEDOBEN 556-08-1 ADRAFINIL 63547-13-7 ACEFLURANOL 80595-73-9 ADRENALONE -

Anesthesia: the Good, the Bad, and the Elderly
ANESTHESIA: THE GOOD, THE BAD, AND THE ELDERLY Item Type Electronic Thesis; text Authors Hansen, Madeline Citation Hansen, Madeline. (2020). ANESTHESIA: THE GOOD, THE BAD, AND THE ELDERLY (Bachelor's thesis, University of Arizona, Tucson, USA). Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 25/09/2021 08:05:26 Item License http://rightsstatements.org/vocab/InC/1.0/ Link to Item http://hdl.handle.net/10150/651023 ANESTHESIA: THE GOOD, THE BAD, AND THE ELDERLY By MADELINE JOLLEEN HANSEN ____________________ A Thesis Submitted to The Honors College In Partial Fulfillment of the Bachelors degree With Honors in Physiology THE UNIVERSITY OF ARIZONA M A Y 2 0 2 0 Approved by: ____________________________ Dr. Zoe Cohen Department of Physiology Table of Contents Page number(s) Abstract……………………………………………………………………………………………………..2 General History of Anesthesia.………………………………………………………………………….3-14 Prehistoric-200AD…………………………………………………………….………………....3-5 200AD- 1846 (historical surgery)…………………….………………………………………….5-8 1847-1992……………………...…………………….……………………………………...….9-14 Physiology of General Anesthesia………………………………………………………...…………...14-16 Understanding of anesthesia mechanism…………………………………………………………14 System impacts………………………………………………………………………………..15-16 Description -

PHARMACEUTICAL APPENDIX to the TARIFF SCHEDULE 2 Table 1
Harmonized Tariff Schedule of the United States (2020) Revision 19 Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2020) Revision 19 Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names INN which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service CAS registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known.