The Importance of Head Circumference: When to Reassure, When to Monitor, When to Refer?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
New Guidelines Review Evidence on PT, Helmets for Positional Plagiocephaly by Sandi K
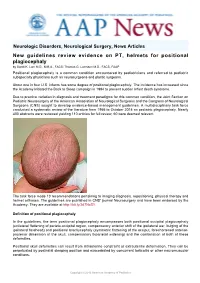
Neurologic Disorders, Neurological Surgery, News Articles New guidelines review evidence on PT, helmets for positional plagiocephaly by Sandi K. Lam M.D., M.B.A., FACS; Thomas G. Luerssen M.D., FACS, FAAP Positional plagiocephaly is a common condition encountered by pediatricians and referred to pediatric subspecialty physicians such as neurosurgeons and plastic surgeons. About one in four U.S. infants has some degree of positional plagiocephaly. The incidence has increased since the Academy initiated the Back to Sleep campaign in 1994 to prevent sudden infant death syndrome. Due to practice variation in diagnosis and treatment paradigms for this common condition, the Joint Section on Pediatric Neurosurgery of the American Association of Neurological Surgeons and the Congress of Neurological Surgeons (CNS) sought to develop evidence-based management guidelines. A multidisciplinary task force conducted a systematic review of the literature from 1966 to October 2014 on pediatric plagiocephaly. Nearly 400 abstracts were reviewed yielding 110 articles for full review; 60 were deemed relevant. The task force made 10 recommendations pertaining to imaging diagnosis, repositioning, physical therapy and helmet orthoses. The guidelines are published in CNS' journal Neurosurgery and have been endorsed by the Academy. They are available at http://bit.ly/2d7NzS1. Definition of positional plagiocephaly In the guidelines, the term positional plagiocephaly encompasses both positional occipital plagiocephaly (unilateral flattening of parieto-occipital region, compensatory anterior shift of the ipsilateral ear, bulging of the ipsilateral forehead) and positional brachycephaly (symmetric flattening of the occiput, foreshortened anterior- posterior dimension of the skull, compensatory biparietal widening) and the combination of both of these deformities. -

Pfeiffer Syndrome Type II Discovered Perinatally
Diagnostic and Interventional Imaging (2012) 93, 785—789 CORE Metadata, citation and similar papers at core.ac.uk Provided by Elsevier - Publisher Connector LETTER / Musculoskeletal imaging Pfeiffer syndrome type II discovered perinatally: Report of an observation and review of the literature a,∗ a a a H. Ben Hamouda , Y. Tlili , S. Ghanmi , H. Soua , b c b a S. Jerbi , M.M. Souissi , H. Hamza , M.T. Sfar a Unité de néonatologie, service de pédiatrie, CHU Tahar Sfar, 5111 Mahdia, Tunisia b Service de radiologie, CHU Tahar Sfar, 5111 Mahdia, Tunisia c Service de gynéco-obstétrique, CHU Tahar Sfar, 5111 Mahdia, Tunisia Pfeiffer syndrome, described for the first time by Pfeiffer in 1964, is a rare hereditary KEYWORDS condition combining osteochondrodysplasia with craniosynostosis [1]. This syndrome is Pfeiffer syndrome; also called acrocephalosyndactyly type 5, which is divided into three sub-types. Type I Cloverleaf skull; is the classic Pfeiffer syndrome, with autosomal dominant transmission, often associated Craniosynostosis; with normal intelligence. Types II and III occur as sporadic cases in individuals who have Syndactyly; craniosynostosis with broad thumbs, broad big toes, ankylosis of the elbows and visceral Prenatal diagnosis abnormalities [2]. We report a case of Pfeiffer syndrome type II, discovered perinatally, which is distinguished from type III by the skull appearing like a cloverleaf, and we shall discuss the clinical, radiological and evolutive features and the advantage of prenatal diagnosis of this syndrome with a review of the literature. Observation The case involved a male premature baby born at 36 weeks of amenorrhoea with multiple deformities at birth. The parents were not blood-related and in good health who had two other boys and a girl with normal morphology. -

1Q21.1 Duplication Syndrome and Epilepsy Case Report and Review
CLINICAL/SCIENTIFIC NOTES OPEN ACCESS 1q21.1 Duplication syndrome and epilepsy Case report and review Ioulia Gourari, MD, Romaine Schubert, MD, and Aparna Prasad, PhD Correspondence Dr. Gourari Neurol Genet 2018;4:e219. doi:10.1212/NXG.0000000000000219 [email protected] Copy number variants (CNVs) of 1q21.1 are increasingly being recognized due to the wide- spread use of genetic screening tests for the investigation of developmental disorders and epilepsy. These include microdeletion and microduplication syndromes, associated with a wide variety of pathology including autism spectrum disorders, attention-deficit disorder, learning disabilities, hypotonia, facial dysmorphisms, and schizophrenia. The 1q21.1 region is consid- ered to be genetically unstable because it contains one of the largest areas of identical dupli- cation sequences in the human genome. Epilepsy has been reported in the literature, particularly in microdeletion syndromes, but rarely in association with microduplication syn- dromes. We report a patient with epilepsy and autism spectrum disorder due to a distal 1q21.1 microduplication and review the available literature and genetic information. Case report We present a 10-year-old girl with a low-functioning autism spectrum disorder and focal motor epilepsy. On examination, she has hypertelorism, minimal communicative language skills, and severe macrocephaly (HC = 57 cm, 3.6 SD > 99%). Seizures started at 7 years of age and consisted of head deviation to the left, generalized stiffening, clonic activity of the mouth, and fluttering of the eyelids, lasting for 1–2 minutes. Multiple video EEG recordings showed a right temporal focus with a less active, independent left temporal focus. 3T MRI scan of the brain was normal. -

Second Family with the Bostontype Craniosynostosis Syndrome: Novel Mutation and Expansion of the Clinical Spectrum
CLINICAL REPORT Second Family With the Boston-Type Craniosynostosis Syndrome: Novel Mutation and Expansion of the Clinical Spectrum Alexander Janssen,1 Mohammad J. Hosen,2 Philippe Jeannin,3 Paul J. Coucke,2 Anne De Paepe,2 and Olivier M. Vanakker2* 1Department of Neurosurgery, Ghent University Hospital, Ghent, Belgium 2Center for Medical Genetics, Ghent University Hospital, Ghent, Belgium 3Department of Pediatrics, Jan Palfijn Hospital, Ghent, Belgium Manuscript Received: 11 January 2013; Manuscript Accepted: 3 May 2013 Craniosynostosis, caused by early fusion of one or more cranial sutures, can affect the coronal or lambdoid sutures, or include How to Cite this Article: premature fusion of the sagittal (scaphocephaly) or metopic Janssen A, Hosen MJ, Jeannin P, Coucke suture (trigonocephaly). Often occurring as isolated finding, PJ, De Paepe A, Vanakker OM. 2013. their co-existence in a craniosynostosis syndrome is infrequent. Second family with the Boston-type We describe a four-generation family with variable expression of craniosynostosis syndrome: Novel mutation a craniosynostosis phenotype with scaphocephaly and a partic- and expansion of the clinical spectrum. ularly severe trigonocephaly. Molecular analysis revealed a mis- sense mutation in the MSX2—associated with the Boston-type Am J Med Genet Part A 161A:2352–2357. craniosynostosis syndrome—affecting the same amino-acid res- idue as in the original Boston family. Besides unique features such as the cranial sutures involved, minor limb abnormalities isolated sagittal synostosis, accounting for more than half of all and incomplete penetrance, our patients share with the original reported cases. Premature fusion of the sagittal suture results in family autosomal dominant inheritance and the presence of decreased width and inverse elongation of the anteroposterior axis multiple endocranial erosions on CT imaging. -

Megalencephaly and Macrocephaly
277 Megalencephaly and Macrocephaly KellenD.Winden,MD,PhD1 Christopher J. Yuskaitis, MD, PhD1 Annapurna Poduri, MD, MPH2 1 Department of Neurology, Boston Children’s Hospital, Boston, Address for correspondence Annapurna Poduri, Epilepsy Genetics Massachusetts Program, Division of Epilepsy and Clinical Electrophysiology, 2 Epilepsy Genetics Program, Division of Epilepsy and Clinical Department of Neurology, Fegan 9, Boston Children’s Hospital, 300 Electrophysiology, Department of Neurology, Boston Children’s Longwood Avenue, Boston, MA 02115 Hospital, Boston, Massachusetts (e-mail: [email protected]). Semin Neurol 2015;35:277–287. Abstract Megalencephaly is a developmental disorder characterized by brain overgrowth secondary to increased size and/or numbers of neurons and glia. These disorders can be divided into metabolic and developmental categories based on their molecular etiologies. Metabolic megalencephalies are mostly caused by genetic defects in cellular metabolism, whereas developmental megalencephalies have recently been shown to be caused by alterations in signaling pathways that regulate neuronal replication, growth, and migration. These disorders often lead to epilepsy, developmental disabilities, and Keywords behavioral problems; specific disorders have associations with overgrowth or abnor- ► megalencephaly malities in other tissues. The molecular underpinnings of many of these disorders are ► hemimegalencephaly now understood, providing insight into how dysregulation of critical pathways leads to ► -
Dysmorphology and Dysfunction in the Brain and Calvarial Vault of Nonsyndromic Craniosynostosis
Yale University EliScholar – A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2013 Dysmorphology And Dysfunction In The rB ain And Calvarial Vault Of Nonsyndromic Craniosynostosis Joel Stanley Beckett Yale School of Medicine, [email protected] Follow this and additional works at: http://elischolar.library.yale.edu/ymtdl Recommended Citation Beckett, Joel Stanley, "Dysmorphology And Dysfunction In The rB ain And Calvarial Vault Of Nonsyndromic Craniosynostosis" (2013). Yale Medicine Thesis Digital Library. 1781. http://elischolar.library.yale.edu/ymtdl/1781 This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for Scholarly Publishing at Yale. It has been accepted for inclusion in Yale Medicine Thesis Digital Library by an authorized administrator of EliScholar – A Digital Platform for Scholarly Publishing at Yale. For more information, please contact [email protected]. Dysmorphology and Dysfunction in the Brain and Calvarial Vault of Nonsyndromic Craniosynostosis Yale University School of Medicine in Partial Fulfillment of the Requirements for the Degree of Doctor of Medicine by Joel Stanley Beckett 2013 Abstract Craniosynostosis is a premature pathologic fusion of one or more sutures in the calvarial vault. The six calvarial sutures are growth sites between adjacent intramembranous bones, which allow for flexibility during passage through the birth canal and accommodation for the growing brain. (1) Premature fusion results in obvious cranial morphologic abnormality and can be associated with elevated intracranial pressure, visual dysfunction, mental retardation and various forms of subtler learning disability. (2) A category of disease called isolated nonsyndromic craniosynostosis (NSC) represents nearly 85% of cases. -

Genetics of Congenital Hand Anomalies
G. C. Schwabe1 S. Mundlos2 Genetics of Congenital Hand Anomalies Die Genetik angeborener Handfehlbildungen Original Article Abstract Zusammenfassung Congenital limb malformations exhibit a wide spectrum of phe- Angeborene Handfehlbildungen sind durch ein breites Spektrum notypic manifestations and may occur as an isolated malforma- an phänotypischen Manifestationen gekennzeichnet. Sie treten tion and as part of a syndrome. They are individually rare, but als isolierte Malformation oder als Teil verschiedener Syndrome due to their overall frequency and severity they are of clinical auf. Die einzelnen Formen kongenitaler Handfehlbildungen sind relevance. In recent years, increasing knowledge of the molecu- selten, besitzen aber aufgrund ihrer Häufigkeit insgesamt und lar basis of embryonic development has significantly enhanced der hohen Belastung für Betroffene erhebliche klinische Rele- our understanding of congenital limb malformations. In addi- vanz. Die fortschreitende Erkenntnis über die molekularen Me- tion, genetic studies have revealed the molecular basis of an in- chanismen der Embryonalentwicklung haben in den letzten Jah- creasing number of conditions with primary or secondary limb ren wesentlich dazu beigetragen, die genetischen Ursachen kon- involvement. The molecular findings have led to a regrouping of genitaler Malformationen besser zu verstehen. Der hohe Grad an malformations in genetic terms. However, the establishment of phänotypischer Variabilität kongenitaler Handfehlbildungen er- precise genotype-phenotype correlations for limb malforma- schwert jedoch eine Etablierung präziser Genotyp-Phänotyp- tions is difficult due to the high degree of phenotypic variability. Korrelationen. In diesem Übersichtsartikel präsentieren wir das We present an overview of congenital limb malformations based Spektrum kongenitaler Malformationen, basierend auf einer ent- 85 on an anatomic and genetic concept reflecting recent molecular wicklungsbiologischen, anatomischen und genetischen Klassifi- and developmental insights. -

Endoscopy-Assisted Early Correction of Single-Suture Metopic Craniosynostosis: a 19-Year Experience
CLINICAL ARTICLE J Neurosurg Pediatr 23:61–74, 2019 Endoscopy-assisted early correction of single-suture metopic craniosynostosis: a 19-year experience David F. Jimenez, MD,1 Michael J. McGinity, MD,1 and Constance M. Barone, MD2 1Department of Neurosurgery, University of Texas Health San Antonio; and 2Cosmetic Surgery Center, San Antonio, Texas OBJECTIVE The objective of this study was to present the authors’ 19-year experience treating metopic craniosynos- tosis by using an endoscopy-assisted technique and postoperative cranial orthotic therapy. The authors also aimed to provide a comprehensive, comparative statistical analysis of minimally invasive surgery (MIS) versus open surgery in reports previously published in the literature (through 2014) regarding only patients with metopic synostosis. METHODS A total of 141 patients with single-suture metopic nonsyndromic craniosynostosis sutures were treated between 1998 and 2017 by endoscopically resecting the synostosed bone followed by postoperative custom cranial orthosis use. All data used in the case series were collected prospectively and stored in a secure database. A compre- hensive literature review was performed that included all previous case series reporting common surgical performance measures. A statistical comparison of traditional open methods versus MIS techniques was performed with regard to age, length of hospital stay (LOS), surgical time, estimated blood loss (EBL), and transfusion rate. RESULTS The mean age at the time of surgery in the current series was 4.1 months. The mean EBL was 33 ml (range 5–250 ml). One patient underwent an intraoperative blood transfusion and 5 underwent postoperative blood transfu- sion for a total transfusion rate of 4.3%. -

Macrocephaly Information Sheet 6-13-19
Next Generation Sequencing Panel for Macrocephaly Clinical Features: Macrocephaly refers to an abnormally large head, OFC greater than 98th percentile, inclusive of the scalp, cranial bone and intracranial contents. Megalencephaly, brain weight/volume ratio greater than 98th percentile, results from true enlargement of the brain parenchyma [1]. Megalencephaly is typically accompanied by macrocephaly, however macrocephaly can occur in the absence of megalencephaly [2]. Both macrocephaly and megalencephaly can been seen as isolated clinical findings as well as clinical features of a mutli-systemic syndromic diagnosis. Our Macrocephaly Panel includes analysis of the 36 genes listed below. Macrocephaly Sequencing Panel ASXL2 GLI3 MTOR PPP2R5D TCF20 BRWD3 GPC3 NFIA PTEN TBC1D7 CHD4 HEPACAM NFIX RAB39B UPF3B CHD8 HERC1 NONO RIN2 ZBTB20 CUL4B KPTN NSD1 RNF125 DNMT3A MED12 OFD1 RNF135 EED MITF PIGA SEC23B EZH2 MLC1 PPP1CB SETD2 Gene Clinical Features Details ASXL2 Shashi-Pena Shashi et al. (2016) found that six patients with developmental delay, syndrome macrocephaly, and dysmorphic features were found to have de novo truncating variants in ASXL2 [3]. Distinguishing features were macrocephaly, absence of growth retardation, and variability in the degree of intellectual disabilities The phenotype also consisted of prominent eyes, arched eyebrows, hypertelorism, a glabellar nevus flammeus, neonatal feeding difficulties and hypotonia. BRWD3 X-linked intellectual Truncating mutations in the BRWD3 gene have been described in males with disability nonsyndromic intellectual disability and macrocephaly [4]. Other features include a prominent forehead and large cupped ears. CHD4 Sifrim-Hitz-Weiss Weiss et al., 2016, identified five individuals with de novo missense variants in the syndrome CHD4 gene with intellectual disabilities and distinctive facial dysmorphisms [5]. -
Craniosynostosis and Related Disorders Mark S
CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care Identifying the Misshapen Head: Craniosynostosis and Related Disorders Mark S. Dias, MD, FAAP, FAANS,a Thomas Samson, MD, FAAP,b Elias B. Rizk, MD, FAAP, FAANS,a Lance S. Governale, MD, FAAP, FAANS,c Joan T. Richtsmeier, PhD,d SECTION ON NEUROLOGIC SURGERY, SECTION ON PLASTIC AND RECONSTRUCTIVE SURGERY Pediatric care providers, pediatricians, pediatric subspecialty physicians, and abstract other health care providers should be able to recognize children with abnormal head shapes that occur as a result of both synostotic and aSection of Pediatric Neurosurgery, Department of Neurosurgery and deformational processes. The purpose of this clinical report is to review the bDivision of Plastic Surgery, Department of Surgery, College of characteristic head shape changes, as well as secondary craniofacial Medicine and dDepartment of Anthropology, College of the Liberal Arts characteristics, that occur in the setting of the various primary and Huck Institutes of the Life Sciences, Pennsylvania State University, State College, Pennsylvania; and cLillian S. Wells Department of craniosynostoses and deformations. As an introduction, the physiology and Neurosurgery, College of Medicine, University of Florida, Gainesville, genetics of skull growth as well as the pathophysiology underlying Florida craniosynostosis are reviewed. This is followed by a description of each type of Clinical reports from the American Academy of Pediatrics benefit from primary craniosynostosis (metopic, unicoronal, bicoronal, sagittal, lambdoid, expertise and resources of liaisons and internal (AAP) and external reviewers. However, clinical reports from the American Academy of and frontosphenoidal) and their resultant head shape changes, with an Pediatrics may not reflect the views of the liaisons or the emphasis on differentiating conditions that require surgical correction from organizations or government agencies that they represent. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

West Texas Craniofacial Center of Excellence
TEAM MEMBERS Tammy Camp, M.D. PAID PERMIT #68 LUBBOCK, TX LUBBOCK, U.S. POSTAGE POSTAGE U.S. NONPROFIT ORG Pediatrician, Texas Tech Physicians Desiree Pendergrass, M.D. Pediatrician Dr. Camp Dr. Camp and Dr. Pendergrass will screen infants and children for cardiac, renal, feeding or airway problems often associated with syndromic craniofacial deformities. Alan Eisenbaum, M.D. Pediatric ophthalmologist, Dr. Pendergrass Texas Tech Physicians Curt Cockings, M.D. Pediatric ophthalmologist Dr. Eisenbaum and Dr. Cockings will screen infants and children with abnormal head shapes for any evidence of optic disc swelling of papilledema Dr. Eisenbaum suggestive of elevated intracranial pressure. They will also screen for any visual loss secondary to optic neuropathy, amblyopia or exposure keratopathy as a results of small orbital volume in syndromic synostoses. APPOINTMENTS Dr. Demke sees patients at the Texas Tech Physicians Medical Pavilion in the Surgery Clinic. His clinic days are Tuesday and Thursday, 8 a.m. – 5 p.m. Please call (806)743-2373 for a referral. SURGERY Dr. Nagy sees patients at Covenant Women’s and Children’s Hospital on Tuesdays and Wednesdays 9am – 5pm weekly. For this clinic location, Lubbock, 79430 Texas please call (806) 743-7700 for a referral. He also sees patients at Texas Department Surgery of Tech Physicians Medical Pavilion, 3rd floor, on Mondays from 9am – 5pm 8312 – MS Street 4th 3601 weekly. For this clinic location, please call (806) 743-7335 for a referral. If a patient needs to see both Dr. Demke and Dr. Nagy, arrangements SURGERY will be made to see the patient on the same day.