J Wave Syndromes As a Cause of Sudden Arrhythmic Death
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2D6 Substrates 2D6 Inhibitors 2D6 Inducers
Physician Guidelines: Drugs Metabolized by Cytochrome P450’s 1 2D6 Substrates Acetaminophen Captopril Dextroamphetamine Fluphenazine Methoxyphenamine Paroxetine Tacrine Ajmaline Carteolol Dextromethorphan Fluvoxamine Metoclopramide Perhexiline Tamoxifen Alprenolol Carvedilol Diazinon Galantamine Metoprolol Perphenazine Tamsulosin Amiflamine Cevimeline Dihydrocodeine Guanoxan Mexiletine Phenacetin Thioridazine Amitriptyline Chloropromazine Diltiazem Haloperidol Mianserin Phenformin Timolol Amphetamine Chlorpheniramine Diprafenone Hydrocodone Minaprine Procainamide Tolterodine Amprenavir Chlorpyrifos Dolasetron Ibogaine Mirtazapine Promethazine Tradodone Aprindine Cinnarizine Donepezil Iloperidone Nefazodone Propafenone Tramadol Aripiprazole Citalopram Doxepin Imipramine Nifedipine Propranolol Trimipramine Atomoxetine Clomipramine Encainide Indoramin Nisoldipine Quanoxan Tropisetron Benztropine Clozapine Ethylmorphine Lidocaine Norcodeine Quetiapine Venlafaxine Bisoprolol Codeine Ezlopitant Loratidine Nortriptyline Ranitidine Verapamil Brofaramine Debrisoquine Flecainide Maprotline olanzapine Remoxipride Zotepine Bufuralol Delavirdine Flunarizine Mequitazine Ondansetron Risperidone Zuclopenthixol Bunitrolol Desipramine Fluoxetine Methadone Oxycodone Sertraline Butylamphetamine Dexfenfluramine Fluperlapine Methamphetamine Parathion Sparteine 2D6 Inhibitors Ajmaline Chlorpromazine Diphenhydramine Indinavir Mibefradil Pimozide Terfenadine Amiodarone Cimetidine Doxorubicin Lasoprazole Moclobemide Quinidine Thioridazine Amitriptyline Cisapride -

Long QT Syndrome: from Channels to Cardiac Arrhythmias
Long QT syndrome: from channels to cardiac arrhythmias Arthur J. Moss, Robert S. Kass J Clin Invest. 2005;115(8):2018-2024. https://doi.org/10.1172/JCI25537. Review Series Long QT syndrome, a rare genetic disorder associated with life-threatening arrhythmias, has provided a wealth of information about fundamental mechanisms underlying human cardiac electrophysiology that has come about because of truly collaborative interactions between clinical and basic scientists. Our understanding of the mechanisms that control the critical plateau and repolarization phases of the human ventricular action potential has been raised to new levels through these studies, which have clarified the manner in which both potassium and sodium channels regulate this critical period of electrical activity. Find the latest version: https://jci.me/25537/pdf Review series Long QT syndrome: from channels to cardiac arrhythmias Arthur J. Moss1 and Robert S. Kass2 1Heart Research Follow-up Program, Department of Medicine, University of Rochester School of Medicine and Dentistry, Rochester, New York, USA. 2Department of Pharmacology, Columbia University Medical Center, New York, New York, USA. Long QT syndrome, a rare genetic disorder associated with life-threatening arrhythmias, has provided a wealth of information about fundamental mechanisms underlying human cardiac electrophysiology that has come about because of truly collaborative interactions between clinical and basic scientists. Our understanding of the mecha- nisms that control the critical plateau and repolarization phases of the human ventricular action potential has been raised to new levels through these studies, which have clarified the manner in which both potassium and sodium channels regulate this critical period of electrical activity. -

Systematic Review of the Effect of Intravenous Lipid Emulsion Therapy for Non-Local Anesthetics Toxicity
Clinical Toxicology ISSN: 1556-3650 (Print) 1556-9519 (Online) Journal homepage: http://www.tandfonline.com/loi/ictx20 Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity Michael Levine, Robert S. Hoffman, Valéry Lavergne, Christine M. Stork, Andis Graudins, Ryan Chuang, Samuel J. Stellpflug, Martin Morris, Andrea Miller-Nesbitt, Sophie Gosselin & for the Lipid Emulsion Workgroup* To cite this article: Michael Levine, Robert S. Hoffman, Valéry Lavergne, Christine M. Stork, Andis Graudins, Ryan Chuang, Samuel J. Stellpflug, Martin Morris, Andrea Miller-Nesbitt, Sophie Gosselin & for the Lipid Emulsion Workgroup* (2016) Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity, Clinical Toxicology, 54:3, 194-221, DOI: 10.3109/15563650.2015.1126286 To link to this article: http://dx.doi.org/10.3109/15563650.2015.1126286 Published online: 06 Feb 2016. Submit your article to this journal Article views: 692 View related articles View Crossmark data Citing articles: 2 View citing articles Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ictx20 Download by: [UPSTATE Medical University Health Sciences Library] Date: 03 August 2016, At: 08:19 CLINICAL TOXICOLOGY, 2016 VOL. 54, NO. 3, 194–221 http://dx.doi.org/10.3109/15563650.2015.1126286 REVIEW Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity Michael Levinea, Robert S. Hoffmanb, Vale´ry Lavergnec, Christine M. Storkd, Andis Graudinse, Ryan Chuangf, Samuel J. Stellpflugg, Martin Morrish, Andrea Miller-Nesbitth, Sophie Gosselini and for the Lipid Emulsion Workgroup* aDepartment of Emergency Medicine, Section of Medical Toxicology, University of Southern California, Los Angeles, CA, USA; bDivision of Medical Toxicology, Ronald O. -

Neurotransmitter Actions
Central University of South Bihar Panchanpur, Gaya, India E-Learning Resources Department of Biotechnology NB: These materials are taken/borrowed/modified/compiled from various resources like research articles and freely available internet websites, and are meant to be used solely for the teaching purpose in a public university, and for serving the needs of specified educational programmes. Dr. Jawaid Ahsan Assistant Professor Department of Biotechnology Central University of South Bihar (CUSB) Course Code: MSBTN2003E04 Course Name: Neuroscience Neurotransmitter Actions • Excitatory Action: – A neurotransmitter that puts a neuron closer to an action potential (facilitation) or causes an action potential • Inhibitory Action: – A neurotransmitter that moves a neuron further away from an action potential • Response of neuron: – Responds according to the sum of all the neurotransmitters received at one time Neurotransmitters • Acetylcholine • Monoamines – modified amino acids • Amino acids • Neuropeptides- short chains of amino acids • Depression: – Caused by the imbalances of neurotransmitters • Many drugs imitate neurotransmitters – Ex: Prozac, zoloft, alcohol, drugs, tobacco Release of Neurotransmitters • When an action potential reaches the end of an axon, Ca+ channels in the neuron open • Causes Ca+ to rush in – Cause the synaptic vesicles to fuse with the cell membrane – Release the neurotransmitters into the synaptic cleft • After binding, neurotransmitters will either: – Be destroyed in the synaptic cleft OR – Taken back in to surrounding neurons (reuptake) Excitable cells: Definition: Refers to the ability of some cells to be electrically excited resulting in the generation of action potentials. Neurons, muscle cells (skeletal, cardiac, and smooth), and some endocrine cells (e.g., insulin- releasing pancreatic β cells) are excitable cells. -

Ventricular Tachycardia Drugs Versus Devices John Camm St
Cardiology Update 2015 Davos, Switzerland: 8-12th February 2015 Ventricular Arrhythmias Ventricular Tachycardia Drugs versus Devices John Camm St. George’s University of London, UK Imperial College, London, UK Declaration of Interests Chairman: NICE Guidelines on AF, 2006; ESC Guidelines on Atrial Fibrillation, 2010 and Update, 2012; ACC/AHA/ESC Guidelines on VAs and SCD; 2006; NICE Guidelines on ACS and NSTEMI, 2012; NICE Guidelines on heart failure, 2008; NICE Guidelines on Atrial Fibrillation, 2006; ESC VA and SCD Guidelines, 2015 Steering Committees: multiple trials including novel anticoagulants DSMBs: multiple trials including BEAUTIFUL, SHIFT, SIGNIFY, AVERROES, CASTLE- AF, STAR-AF II, INOVATE, and others Events Committees: one trial of novel oral anticoagulants and multiple trials of miscellaneous agents with CV adverse effects Editorial Role: Editor-in-Chief, EP-Europace and Clinical Cardiology; Editor, European Textbook of Cardiology, European Heart Journal, Electrophysiology of the Heart, and Evidence Based Cardiology Consultant/Advisor/Speaker: Astellas, Astra Zeneca, ChanRX, Gilead, Merck, Menarini, Otsuka, Sanofi, Servier, Xention, Bayer, Boehringer Ingelheim, Bristol- Myers Squibb, Daiichi Sankyo, Pfizer, Boston Scientific, Biotronik, Medtronic, St. Jude Medical, Actelion, GlaxoSmithKline, InfoBionic, Incarda, Johnson and Johnson, Mitsubishi, Novartis, Takeda Therapy for Ventricular Tachycardia Medical therapy Antiarrhythmic drugs Autonomic management Ventricular tachycardia Monomorphic Polymorphic Ventricular fibrillation Ventricular storms Ablation therapy Device therapy Surgical Defibrillation Catheter Antitachycardia pacing History of Antiarrhythmic Drugs 1914 - Quinidine 1950 - Lidocaine 1951 - Procainamide 1946 – Digitalis 1956 – Ajmaline 1962 - Verapamil 1962 – Disopyramide 1964 - Propranolol 1967 – Amiodarone 1965 – Bretylium 1972 – Mexiletine 1973 – Aprindine, Tocainide 1969 - Diltiazem 1975- Flecainide 1976 – Propafenone Encainide Ethmozine 2000 - Sotalol D-sotalol 1995 - Ibutilide (US) Recainam 2000 – Dofetilide US) IndecainideX Etc. -
Open Access Journal of Cardiology Ventricular Tachycardia During Ajmaline Challenge
Open Access Journal of Cardiology Ventricular Tachycardia During Ajmaline Challenge Estrada Parra I, Pavón Jimenez R, Leal del Ojo J, Garcia Medina D, Case Report Picon Heras R* and Pastor Torres L Volume 1 Issue 1 Received Date: May 22, 2017 Departamento de Cardiologia, Hospital Universitario Virgen de Valme, Spain Published Date: August 19, 2017 *Corresponding author: Rocio Picon, Departamento de Cardiologia, Hospital Universitario Virgen de Valme, Spain, E- mail: [email protected] Abstract We report the case of a 63 year old woman who comes to an ajmaline challenged. After 8 minutes of infusion her baseline ECG showed significant QRS complex prolongation and switched over to the typical coved-type ECG. Subsequently a sustained monomorphic ventricular tachycardia was developed, followed by a sustained polymorphyc VT onset, which finally degenerated in a hemodynamically non relevant sustained monomorphic VT. Finally, a 200J defibrillation was required to terminate the arrythmia. Sustained ventricular arrhytmia (SVA) is infrequent but not an exceptional event (0.1-18%) and ajmaline is considered a valuable drug. In addition, provocation testing must be performed in an appropiate environment with advanced life support facilities. The evidence shows that the occurrence of ajmaline-induced sustained ventricular arryhtmia in patients with BS might not identify a category at higher risk for further arrhythmic events during follow-up. Keywords: Brugada syndrome; Sodium channel blocker Challenge; Ajmaline Challenge; Ventricular arrhythmias; Proarrhythmia Abbrevations: ECG: Electrocardiography; BS: Brugada infusion she showed significant QRS complex Syndrome; SCB: Sodium Channel Blockers; VT: prolongation (174 ms) and ST elevation in the right Ventricular Tachycardia; SVA: Sustained ventricular precordial leads, which switched over to the typical arrhytmia coved-type ECG (Figure 2). -

1 the New Definition of Early Repolarisation Peter W. Macfarlane
1 The New Definition of Early Repolarisation Peter W. Macfarlane Institute of Cardiovascular and Medical Sciences University of Glasgow Address for Correspondence: Electrocardiology Group Level 1, New Lister Building Royal Infirmary, Glasgow G31 2ER Scotland, UK. e-mail: [email protected] 2 Introduction There has been an increasing interest in the electrocardiographic pattern of early repolarization in recent years following the publication of a paper by Haissaguerre and colleagues [1] in 2008, which linked their definition of the pattern to sudden cardiac arrest due to idiopathic ventricular fibrillation. However, earlier and later publications [2-17] by other groups on the topic of early repolarisation seemed to exhibit disagreement over what constituted the ECG pattern of early repolarisation suggesting a degree of confusion following the 2008 publication [1]. In 1947, Myers et al [2] reported that, among other features, an “elevation of the RS-T take off of 0.5 - 2.0mm may be considered as a normal variant” provided that the ST segment was concave upwards and followed by a tall T wave. In 1951, Goldman also reported on RS-T segment elevation in V3-V6 as a normal variant [3]. The original description of what for many years was regarded as the early repolarization pattern can probably be traced back to an early paper by Wasserburger and Alt [4] dealing with normal RS-T elevation in the relatively newly established full 12 lead ECG. The authors pointed out that the ST elevation mostly arose from a distinct notch on the downslope of the R wave but was occasionally associated with a “well-defined slur”. -

The Short QT Syndrome
The Short QT Syndrome A note from the SADS Foundation References We provide this information with the hope that informing 1. Gussak I, Brugada P, Brugada J, Wright RS, Kopecky SL, Chaitman A Guide for Patients BR, Bjerregaard P. Idiopathic short QT interval: a new clinical physicians and other health care providers, as well as the public, and Health Care will encourage early and correct diagnosis and proper therapy syndrome? Cardiology 2000;94:99 –102. for congenital short QT syndrome (SQTS), resulting in the 2. Giustetto C, Di Monte F. Wolpert C, Borggrefe M, Schimpf R, Providers reduction and ultimately elimination of sudden cardiac arrest Sbragia P, Leone G, Maury P, Anttonen O, Haissaguerre M, Gaita F. (SCA) and sudden cardiac death (SCD). Short QTsyndrome: clinical findings and diagnostic-therapeutic implications. Eur Heart J 2006;27:2440 –2447. 3. Gaita F, Giustetto C, Bianchi F, Wolptert C, Schimpf R, Riccardi R, Grossi S, Richiardi E, Borggrefe M. Short QT syndrome: a familial What do Patients and Parents Need to Know cause of sudden death. Circulation 2003;108:965–970. about SQTS? 4. Dhutia H, Malhotra A, Parpia S, et al. The Prevalence and • The warning signs and symptoms of SQTS. significance of a short QT interval in 18 825 low-risk individuals • Who to see for proper testing. including athletes. Br J Sports Med 2015;0:1-6 • How to protect their children and themselves. • How to expand their family pedigree and contact other family members who may be at risk What do Physicians need to know? • When to consider SQTS as a possible diagnosis. -

The Action Potential Label the Significant Membrane Potentials and Phases of the Action Potential in a Neuron
Worksheet by Andrey Michel The Action Potential Label the significant membrane potentials and phases of the action potential in a neuron. Indicate which gates are open/closed as well as the direction of the net movement of sodium and potassium ions across the cell membrane for A-G. H I D +30 0 C E -55 B Membrane Potential Membrane (mV) G -70 A -80 F 0 1 2 3 4 5 Time (ms) 1. What type of summation is shown for the graded potentials in the above graph? 2. What happens when the threshold potential is reached? 3. At approximately +30 mV on the graph, what happens in between the depolarization and repolarization phases? 4. What mechanism is responsible for the occurrence of the hyperpolarization phase? 5. How is the resting membrane potential of the neuron restored? 6. Is it possible to generate a second action potential during either refractory period? If so, which one and how? Place the following events in chronological order from 1-8: Na+ enters the cell, and depolarization occurs to approximately +30 mV. The voltage across the cell membrane is -70 mV, the resting membrane potential. Upon reaching the peak of the action potential, the VG Na+ channels are inactivated by the closing of their inactivation gate and the activation gate of each VG K+ channel opens. VG K+ channels close by the closing of their activation gate, and the resting membrane potential is gradually restored. An excitatory post-synaptic potential depolarizes the membrane to threshold and the activation gate of VG Na+ channels open. -

The Anti-Addiction Drug Ibogaine and the Heart: a Delicate Relation
Molecules 2015, 20, 2208-2228; doi:10.3390/molecules20022208 OPEN ACCESS molecules ISSN 1420-3049 www.mdpi.com/journal/molecules Review The Anti-Addiction Drug Ibogaine and the Heart: A Delicate Relation Xaver Koenig * and Karlheinz Hilber * Department of Neurophysiology and Neuropharmacology, Center for Physiology and Pharmacology, Medical University of Vienna, Schwarzspanierstrasse 17, Vienna 1090, Austria * Authors to whom correspondence should be addressed; E-Mails: [email protected] (X.K.); [email protected] (K.H.); Tel.: +43-1-40160-31232 (X.K.); +43-1-40160-31230 (K.H.); Fax: +43-1-40160-931300 (X.K. & K.H.). Academic Editor: Patricia Valentao Received: 24 October 2014 / Accepted: 26 November 2014 / Published: 29 January 2015 Abstract: The plant indole alkaloid ibogaine has shown promising anti-addictive properties in animal studies. Ibogaine is also anti-addictive in humans as the drug alleviates drug craving and impedes relapse of drug use. Although not licensed as therapeutic drug and despite safety concerns, ibogaine is currently used as an anti-addiction medication in alternative medicine in dozens of clinics worldwide. In recent years, alarming reports of life-threatening complications and sudden death cases, temporally associated with the administration of ibogaine, have been accumulating. These adverse reactions were hypothesised to be associated with ibogaine’s propensity to induce cardiac arrhythmias. The aim of this review is to recapitulate the current knowledge about ibogaine’s effects on the heart and the cardiovascular system, and to assess the cardiac risks associated with the use of this drug in anti- addiction therapy. The actions of 18-methoxycoronaridine (18-MC), a less toxic ibogaine congener with anti-addictive properties, are also considered. -
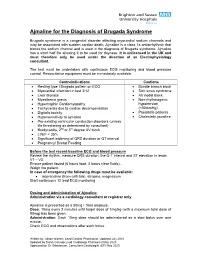
Use of Ajmaline for the Diagnosis of Brugada Syndrome
Ajmaline for the Diagnosis of Brugada Syndrome Brugada syndrome is a congenital disorder affecting myocardial sodium channels and may be associated with sudden cardiac death. Ajmaline is a class 1a antiarrhythmic that blocks the sodium channel and is used in the diagnosis of Brugada syndrome. Ajmaline has a short half life allowing it to be used for daycase. It is unlicensed in the UK and must therefore only be used under the direction of an Electrophysiology consultant. The test must be undertaken with continuous ECG monitoring and blood pressure control. Resuscitative equipment must be immediately available. Contraindications Cautions Resting type I Brugada pattern on ECG Bundle branch block Myocardial infarction in last 3/12 Sick sinus syndrome Liver disease AV nodal block Myasthenia gravis Non-rhythmogenic Hypertrophic Cardiomyopathy hypotension Tachycardia due to cardiac decompensation (<90mmHg) Digitalis toxicity Paediatric patients Hypersensitivity to ajmaline Cholestatic jaundice Pre-existing ventricular conduction disorders (unless life threatening as determined by consultant) Bradycardia, 2nd or 3rd degree AV block LVEF < 35% Significant widening of QRS duration or QT interval Pregnancy/ Breast Feeding Before the test record baseline ECG and blood pressure Review the rhythm, measure QRS duration, the Q-T interval and ST elevation in leads V1 – V3. Ensure patient fasted (6 hours food, 2 hours clear fluids). Weigh the patient. In case of emergency the following drugs must be available: isoprenaline (from cath lab), atropine, magnesium Start continuous 12 lead ECG monitoring Dosing and Administration of Ajmaline: Administration via a cardiology consultant or registrar only Ajmaline is presented as a 50mg / 10ml ampoule. Dose: 10mg every 2 minutes until target dose of 1mg/kg (with a maximum total dose of 80mg) has been given. -

Stembook 2018.Pdf
The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 WHO/EMP/RHT/TSN/2018.1 © World Health Organization 2018 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances. Geneva: World Health Organization; 2018 (WHO/EMP/RHT/TSN/2018.1). Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data.