4.. Pathol 1991;95:511-6
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
INTRODUCTION Time, Are Discussed in Full, for Without Accurate
Br J Ophthalmol: first published as 10.1136/bjo.31.Suppl.7 on 1 January 1947. Downloaded from INTRODUCTION This is a contribution to the study of vertical defects in the positions of the eyes. It includes a partial survey of the literature and an analysis of a series of 402 patients with horizontal and vertical defects of the concomitant and paralytic types. Methods of investigation, including two that are described for the first time, are discussed in full, for without accurate observations satis- factory treatment is unlikely. The value of the " division " of diplopia is stressed. There are many types of ocular vertical deviations. Their recog- nition is not always easy nor is their interpretation always simple. They must be studied in near and distant vision as well as when the gaze is directed obliquely. Any deviation may depend on the following: 1. The position of ocular rest. 2. The degree of fusion permitting true or alternating hyperphoria. 3. The presence of a paralysed muscle and its stage of recovery. 4. Contraction of antagonist and synergist and inhibitional paresis. 5. The fascial check ligaments restricting ocular rotation. 6. " Abnormal excitations of the centres controlling the non- copyright. parallel movements." Bielschowsky (August, 1938). These will now be considered at length. Position of Ocular Rest.-A vertical angle gamma is a very rare finding. It occurs when the visual line connecting the fovea passes above or below the geometrical axis. This is revealed by a study of the corneal reflexes. Many observers have been tempted to seek the so-called position of rest by withdrawing the bond of fusion. -

Multiple Intracerebral Hemorrhages in an Old Patient with Rheumatoid Arthritis
Multiple Intracerebral Hemorrhages in an Old Patient with Rheumatoid Arthritis INIMIOARA MIHAELA COJOCARU1, 2, V. ŞTEFĂNESCU2, DANIELA TRAŞCĂ2, ADELINA ŞERBAN-PEREŢEANU2, B. CHICOŞ3, M. COJOCARU3,4 1“Carol Davila” University of Medicine and Pharmacy, Bucharest 2Department of Neurology, “Colentina” Clinical Hospital 3“Dr. Ion Stoia” Clinical Center for Rheumatic Diseases 4“Titu Maiorescu” University, Faculty of Medicine, Bucharest, Romania A 78-year-old Caucasian man was admitted in the Department of Neurology for visual disturbances, started two days before. The next day the patient experienced headache, fever and gait disturbances. He had hypertension, diabetes mellitus, an ischemic stroke 13 years ago, longstanding seronegative rheumatoid arthritis (17 years), polynodular goiter, right ischio-pubian fracture and right femoral vein thrombosis a year ago due to a car accident, since he is treated with oral anticoagulants associated to antiaggregant, hypotensors, statin and oral antidiabetics. The neurologic examination had evidenced nuchal rigidity, left homonymous hemianopsia, left central facial palsy, ataxia of the inferior limbs with wide-based gait, achilean reflexes abolished bilaterally, bilaterally abolished plantar reflexes, ideomotor apraxia, dysarthria, hypoprosexia, and preserved consciousness patient. A non-contrast cerebral CT scan had shown right temporal and parieto-occipital intraparenchymatous hemorrhages, a right frontal sequelar lesion, multiple old lacunar infarcts, cortical atrophy. Laboratory findings included an inflammatory syndrome, absence of rheumatoid arthritis positive serology, normal coagulogram, an elevated proteinuria. The cerebral IRM performed on the seventh day of hospitalisation was suggestive for subacute right parietal hemorrhage, old cerebral infarction in the right anterior cerebral artery area, old lacunar infarcts and cerebral atrophy. The anticoagulant and antiaggregant treatment was stopped after a generalized tonic-clonic seizure occurred. -

Circuits in the Rodent Brainstem That Control Whisking in Concert with Other Orofacial Motor Actions
Neuroscience 368 (2018) 152–170 CIRCUITS IN THE RODENT BRAINSTEM THAT CONTROL WHISKING IN CONCERT WITH OTHER OROFACIAL MOTOR ACTIONS y y LAUREN E. MCELVAIN, a BETH FRIEDMAN, a provides the reset to the relevant premotor oscillators. HARVEY J. KARTEN, b KAREL SVOBODA, c FAN WANG, d Third, direct feedback from somatosensory trigeminal e a,f,g MARTIN DESCHEˆ NES AND DAVID KLEINFELD * nuclei can rapidly alter motion of the sensors. This feed- a Department of Physics, University of California at San Diego, back is disynaptic and can be tuned by high-level inputs. La Jolla, CA 92093, USA A holistic model for the coordination of orofacial motor actions into behaviors will encompass feedback pathways b Department of Neurosciences, University of California at San Diego School of Medicine, La Jolla, CA 92093, USA through the midbrain and forebrain, as well as hindbrain c areas. Howard Hughes Medical Institute, Janelia Research This article is part of a Special Issue entitled: Barrel Campus, Ashburn, VA 20147, USA Cortex. Ó 2017 IBRO. Published by Elsevier Ltd. All rights d Department of Neurobiology, Duke University Medical reserved. Center, Durham, NC 27710, USA e Department of Psychiatry and Neuroscience, Laval University, Que´bec City, G1J 2G3, Canada f Key words: coupled oscillators, facial nucleus, hypoglossal Section of Neurobiology, University of California at San Diego, La Jolla, CA 92093, USA nucleus, licking, orienting, tongue, vibrissa. g Department of Electrical and Computer Engineering, University of California at San Diego, La Jolla, CA 92093, USA Contents Introduction 153 Abstract—The world view of rodents is largely determined Coordination of multiple orofacial motor actions 153 by sensation on two length scales. -

Facial Nerve Electrodiagnostics for Patients with Facial Palsy: a Clinical Practice Guideline
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Helsingin yliopiston digitaalinen arkisto European Archives of Oto-Rhino-Laryngology (2020) 277:1855–1874 https://doi.org/10.1007/s00405-020-05949-1 REVIEW ARTICLE Facial nerve electrodiagnostics for patients with facial palsy: a clinical practice guideline Orlando Guntinas‑Lichius1,2,3 · Gerd Fabian Volk1,2 · Kerry D. Olsen4 · Antti A. Mäkitie5 · Carl E. Silver6 · Mark E. Zafereo7 · Alessandra Rinaldo8 · Gregory W. Randolph9 · Ricard Simo10 · Ashok R. Shaha11 · Vincent Vander Poorten3,12 · Alfo Ferlito13 Received: 14 March 2020 / Accepted: 27 March 2020 / Published online: 8 April 2020 © The Author(s) 2020 Abstract Purpose Facial nerve electrodiagnostics is a well-established and important tool for decision making in patients with facial nerve diseases. Nevertheless, many otorhinolaryngologist—head and neck surgeons do not routinely use facial nerve electro- diagnostics. This may be due to a current lack of agreement on methodology, interpretation, validity, and clinical application. Electrophysiological analyses of the facial nerve and the mimic muscles can assist in diagnosis, assess the lesion severity, and aid in decision making. With acute facial palsy, it is a valuable tool for predicting recovery. Methods This paper presents a guideline prepared by members of the International Head and Neck Scientifc Group and of the Multidisciplinary Salivary Gland Society for use in cases of peripheral facial nerve disorders based on a systematic literature search. Results Required equipment, practical implementation, and interpretation of the results of facial nerve electrodiagnostics are presented. Conclusion The aim of this guideline is to inform all involved parties (i.e. -

DR. Sanaa Alshaarawy
By DR. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific criteria of each level. 1. Medulla oblongata (closed, mid and open medulla) 2. Pons (caudal, mid “Trigeminal level” and rostral). 3. Mid brain ( superior and inferior colliculi). Describe the Reticular formation (structure, function and pathway) being an important content of the brain stem. 2 1. Traversed by the Central Canal. Motor Decussation*. Spinal Nucleus of Trigeminal (Trigeminal sensory nucleus)* : ➢ It is a larger sensory T.S of Caudal part of M.O. nucleus. ➢ It is the brain stem continuation of the Substantia Gelatinosa of spinal cord 3 The Nucleus Extends : Through the whole length of the brain stem and upper segments of spinal cord. It lies in all levels of M.O, medial to the spinal tract of the trigeminal. It receives pain and temperature from face, forehead. Its tract present in all levels of M.O. is formed of descending fibers that terminate in the trigeminal nucleus. 4 It is Motor Decussation. Formed by pyramidal fibers, (75-90%) cross to the opposite side They descend in the Decuss- = crossing lateral white column of the spinal cord as the lateral corticospinal tract. The uncrossed fibers form the ventral corticospinal tract. 5 Traversed by Central Canal. Larger size Gracile & Cuneate nuclei, concerned with proprioceptive deep sensations of the body. Axons of Gracile & Cuneate nuclei form the internal arcuate fibers; decussating forming Sensory Decussation. Pyramids are prominent ventrally. 6 Formed by the crossed internal arcuate fibers Medial Leminiscus: Composed of the ascending internal arcuate fibers after their crossing. -

Cranial Nerves 1, 5, 7-12
Cranial Nerve I Olfactory Nerve Nerve fiber modality: Special sensory afferent Cranial Nerves 1, 5, 7-12 Function: Olfaction Remarkable features: – Peripheral processes act as sensory receptors (the other special sensory nerves have separate Warren L Felton III, MD receptors) Professor and Associate Chair of Clinical – Primary afferent neurons undergo continuous Activities, Department of Neurology replacement throughout life Associate Professor of Ophthalmology – Primary afferent neurons synapse with secondary neurons in the olfactory bulb without synapsing Chair, Division of Neuro-Ophthalmology first in the thalamus (as do all other sensory VCU School of Medicine neurons) – Pathways to cortical areas are entirely ipsilateral 1 2 Crania Nerve I Cranial Nerve I Clinical Testing Pathology Anosmia, hyposmia: loss of or impaired Frequently overlooked in neurologic olfaction examination – 1% of population, 50% of population >60 years Aromatic stimulus placed under each – Note: patients with bilateral anosmia often report nostril with the other nostril occluded, eg impaired taste (ageusia, hypogeusia), though coffee, cloves, or soap taste is normal when tested Note that noxious stimuli such as Dysosmia: disordered olfaction ammonia are not used due to concomitant – Parosmia: distorted olfaction stimulation of CN V – Olfactory hallucination: presence of perceived odor in the absence of odor Quantitative clinical tests are available: • Aura preceding complex partial seizures of eg, University of Pennsylvania Smell temporal lobe origin -

Cortical Control of Facial Expression
Review The Journal of Comparative Neurology Research in Systems Neuroscience DOI 10.1002/cne.23908 Topical review Cortical control of facial expression. René M. Müri1,2,3 1Division of Cognitive and Restorative Neurology, Departments of Neurology and Clinical Research, University Hospital Inselspital, Bern, Switzerland 2Gerontechnology and Rehabilitation Group, University of Bern, Bern, Switzerland 3Center for Cognition, Learning, and Memory, University of Bern, Bern, Switzerland Abbreviated title: Cortical control of facial expression Key words: human, facial expression, emotion, facial innervation | downloaded: 13.3.2017 http://boris.unibe.ch/72088/ This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process which may lead to differences between this version and the Version of Record. Please cite this article as an ‘Accepted Article’, doi: 10.1002/cne.23908 source: © 2015 Wiley Periodicals, Inc. Received: Jan 31, 2015; Revised: Sep 19, 2015; Accepted: Sep 25, 2015 This article is protected by copyright. All rights reserved. Journal of Comparative Neurology Page 4 of 23 Abstract The present topical review deals with the motor control of facial expressions in humans. Facial expressions are a central part of human communication. Emotional face expressions have a crucial role in human non-verbal behavior, allowing a rapid transfer of information between individuals. Facial expressions can be both voluntarily or emotionally controlled. Recent studies in non-human primates and humans revealed that the motor control of facial expressions has a distributed neural representation. At least 5 cortical regions on the medial and lateral aspects of each hemisphere are involved: the primary motor cortex, the ventral lateral premotor cortex, the supplementary motor area on the medial wall, and, finally, the rostral and caudal cingulate cortex. -
Crossed Brainstem Syndrome Revealing
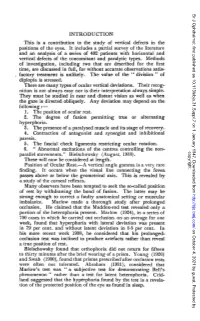
Beucler et al. BMC Neurology (2021) 21:204 https://doi.org/10.1186/s12883-021-02223-7 CASE REPORT Open Access Crossed brainstem syndrome revealing bleeding brainstem cavernous malformation: an illustrative case Nathan Beucler1,2* , Sébastien Boissonneau1,3, Aurélia Ruf4, Stéphane Fuentes1, Romain Carron3,5 and Henry Dufour1,6 Abstract Background: Since the nineteenth century, a great variety of crossed brainstem syndromes (CBS) have been described in the medical literature. A CBS typically combines ipsilateral cranial nerves deficits to contralateral long tracts involvement such as hemiparesis or hemianesthesia. Classical CBS seem in fact not to be so clear-cut entities with up to 20% of patients showing different or unnamed combinations of crossed symptoms. In terms of etiologies, acute brainstem infarction predominates but CBS secondary to hemorrhage, neoplasm, abscess, and demyelination have been described. The aim of this study was to assess the proportion of CBS caused by a bleeding episode arising from a brainstem cavernous malformation (BCM) reported in the literature. Case presentation: We present the case of a typical Foville syndrome in a 65-year-old man that was caused by a pontine BCM with extralesional bleeding. Following the first bleeding episode, a conservative management was decided but the patient had eventually to be operated on soon after the second bleeding event. Discussion: A literature review was conducted focusing on the five most common CBS (Benedikt, Weber, Foville, Millard-Gubler, Wallenberg) on Medline database from inception to 2020. According to the literature, hemorrhagic BCM account for approximately 7 % of CBS. Microsurgical excision may be indicated after the second bleeding episode but needs to be carefully weighted up against the risks of the surgical procedure and openly discussed with the patient. -

Somatotopic Organization of Perioral Musculature Innervation Within the Pig Facial Motor Nucleus
Original Paper Brain Behav Evol 2005;66:22–34 Received: September 20, 2004 Returned for revision: November 10, 2004 DOI: 10.1159/000085045 Accepted after revision: December 7, 2004 Published online: April 8, 2005 Somatotopic Organization of Perioral Musculature Innervation within the Pig Facial Motor Nucleus Christopher D. Marshall a Ron H. Hsu b Susan W. Herring c aTexas A&M University at Galveston, Galveston, Tex., bDepartment of Pediatric Dentistry, University of North Carolina, Chapel Hill, N.C., and cDepartment of Orthodontics, University of Washington, Seattle, Wash., USA Key Words pools of the lateral 4 of the 7 subnuclei of the facial motor Somatotopy W Innervation W Facial nucleus W Perioral nucleus. The motor neuron pools of the perioral muscles muscles W Orbicularis oris W Buccinator W Mammals were generally segregated from motoneurons innervat- ing other facial muscles of the rostrum. However, motor neuron pools were not confined to single nuclei but Abstract instead spanned across 3–4 subnuclei. Perioral muscle The orbicularis oris and buccinator muscles of mammals motor neuron pools overlapped but were organized so- form an important subset of the facial musculature, the matotopically. Motor neuron pools of portions of the perioral muscles. In many taxa, these muscles form a SOO overlapped greatly with each other but exhibited a robust muscular hydrostat capable of highly manipula- crude somatotopy within the SOO motor neuron pool. tive fine motor movements, likely accompanied by a spe- The large and somatotopically organized SOO motor cialized pattern of innervation. We conducted a retro- neuron pool in pigs suggests that the upper lip might be grade nerve-tracing study of cranial nerve (CN) VII in pigs more richly innervated than the other perioral muscles (Sus scrofa) to: (1) map the motor neuron pool distribu- and functionally divided. -

The Origin of Facial Palsy in Multiple Sclerosis
ISSN 2470-4059 OTOLARYNGOLOGY Open Journal PUBLISHERS Editorial The Origin of Facial Palsy in Multiple Sclerosis Arianna Di Stadio, MD, PhD1*; Evanthia Bernitsas, MD2 1Department of Neurology, San Camillo Hospital IRCCS, Venice, Italy 2Multiple Sclerosis Center, Wayne State University School of Medicine, Detroit, MI, USA *Corresponding author Arianna Di Stadio, MD, PhD Assistant Professor, Department of Neurology, San Camillo Hospital IRCCS, Venice, Italy; E-mail: [email protected] Article information Received: April 16th, 2018; Accepted: April 27th, 2018; Published: April 30th, 2018 Cite this article Di Stadio A, Bernitsas E. the origin of facial palsy in multiple sclerosis. Otolaryngol Open J. 2018; 4(1): e1-e4. doi: 10.17140/OTLOJ-4-e006 ultiple Sclerosis (MS) is an autoimmune neurodegenera- Mtive disease that affects several people especially in North Figure 1. The Image Summarizes the Facial Pathway from Periphery America and Canada. In 2013, 33 individuals over 100,000 were (Terminal Branch of Facial Nerve) to the Brain Motor Cortex Area (M1) affected from MS; the estimated increase for 5 years of observation ranged from an average of 4.7 per 100,000 in high-income coun- tries to just 0.04 per 100,000 in the low-income countries.1 Women are more affected than men (2.3-3.5:1), but in men, the disease is usually more aggressive and has a worse prog- nosis than in women.2 MS is a demyelinating disorder in which the immune system attacks the neural structures in the central nervous system (CNS)3; this mechanism is determined by a particular class of cells- Microglia- thathave been identified as responsible of the degenera- tive process. -
Lecture (6) Internal Structures of the Brainstem.Pdf
Internal structures of the Brainstem Neuroanatomy block-Anatomy-Lecture 6 Editing file Objectives At the end of the lecture, students should be able to: ● Distinguish the internal structure of the components of the brain stem in different levels and the specific criteria of each level. 1. Medulla oblongata (closed, mid and open medulla) 2. Pons (caudal and rostral). 3. Midbrain ( superior and inferior colliculi). Color guide ● Only in boys slides in Green ● Only in girls slides in Purple ● important in Red ● Notes in Grey Medulla oblongata Caudal (Closed) Medulla Traversed by the central canal Motor decussation (decussation of the pyramids) ● Formed by pyramidal fibers, (75-90%) cross to the opposite side ● They descend in the lateral white column of the spinal cord as the lateral corticospinal tract. ● The uncrossed fibers form the ventral corticospinal tract Trigeminal sensory nucleus. ● it is the larger sensory nucleus. ● The Nucleus Extends Through the whole length of the brainstem and its note :All CN V afferent sensory information enters continuation of the substantia gelatinosa of the spinal cord. the brainstem through the nerve itself located in the pons. Thus, to reach the spinal nucleus (which ● It lies in all levels of M.O, medial to the spinal tract of the trigeminal. spans the entire brain stem length) in the Caudal ● It receives pain and temperature from face, forehead. Medulla those fibers have to "descend" in what's known as the Spinal Tract of the Trigeminal ● Its tract present in all levels of M.O. is formed of descending (how its sensory and descend?see the note) fibers that terminate in the trigeminal nucleus. -

Vascular Complications After Radiosurgery for Meningiomas
Neurosurg Focus 22 (3):E9, 2007 Vascular complications after radiosurgery for meningiomas KAVEH BARAMI, M.D., PH.D.,1 ALLISON GROW, M.D., PH.D.,2 STEVEN BREM, M.D.,3 ELIAS DAGNEW, M.D.,1 AND ANDREW E. SLOAN, M.D.3 1Memorial Neuroscience Center; 2Cyberknife Cancer Center, Memorial Hospital Jacksonville; and 3H. Lee Moffitt Cancer Center & Research Institute, Tampa, Florida PDuring the past 25 years, radiosurgery has evolved as a primary treatment modality for certain menin- giomas when resection would be associated with high patient morbidity. In addition, radiosurgery is now routinely used as an adjunctive therapy for residual or recurrent meningiomas after surgical removal. In this review the authors summarize the vascular complications that occur after radiosurgery for menin- giomas as well as experimental study data that give insight into the pathogenesis of this complication. These data may be useful when discussing with patients the risk/benefit ratio of choosing among conserv- ative management, radiosurgery, and surgery. KEY WORDS • vascular complication • hemorrhage • occlusion • meningioma • radiosurgery OST MENINGIOMAS are histopathologically benign hemiparesis in convexity lesions, and hemianopia in lesions, and yet their rate of recurrence increases occipital lobe meningiomas.5,8,15,33 Vascular complications M if complete resection is not achieved.21,31 Despite following radiosurgery seem to be rare and can be classi- advances in the surgical approaches and techniques for fied as occlusion of vessels or hemorrhage. In this review removing these lesions, complete removal of parasellar, article we summarize the reported cerebrovascular com- cavernous, orbital, and petroclival meningiomas and those plications following radiosurgery for meningiomas as near the major venous sinuses remains difficult and is well as the experimental study data related to the his- associated with high morbidity.6,25 In reporting on the out- topathological findings of the cerebral vasculature after come of the aggressive removal of cavernous sinus men- applying radiation.